Discuss lesions of breast in children and adolescents
Reading File
Finding Sources
Finding Sources
Searching PubMed
breast lesions children adolescents
Finding Sources
Finding Sources
Reading Article
Reading Article
Finding Sources
Finding Sources
Finding Sources
Reading Article
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
I now have sufficient material to write a thorough, well-organized answer. Let me compile the response.
Lesions of the Breast in Children and Adolescents
Breast lesions are uncommon in pediatric and adolescent patients but form a distinct clinical group that differs substantially from adult breast disease. The vast majority (>95%) are benign. Malignant primary breast tumors are extremely rare in this age group. Because the breast bud is actively developing during puberty, any surgical or biopsy approach must be conservative to preserve future breast form and function.
1. Normal Breast Development: Context
Breast development (thelarche) begins at puberty (typically ages 8-13) under the influence of ovarian estrogen. The earliest sign is the breast bud, a disc of subareolar tissue. Normal development proceeds through Tanner stages I-V over 2-4 years. Any mass detected before full maturity must be assessed carefully to distinguish a normal developing bud from a true lesion, as inadvertent excision of the breast bud leads to permanent aplasia.
2. Non-Neoplastic / Developmental Abnormalities
Premature Thelarche
Unilateral or bilateral breast enlargement in girls under 2-4 years of age without other signs of sexual maturation. There is no significant nipple or areolar development. It may result from increased breast sensitivity to low estrogen levels or from estradiol secretion by follicular ovarian cysts. It is a benign self-limited condition; only reassurance and periodic follow-up are required. Normal onset of puberty, adult height, and reproductive function generally follow. Rarely, it can herald progressive precocious puberty. Uterine volume measurement is the most sensitive discriminator between premature thelarche and true precocious puberty. Breast ultrasound can exclude structural lesions such as fibroadenomas, cysts, or neurofibromas. - Berek & Novak's Gynecology, p. 350
Gynecomastia
Benign enlargement of breast glandular tissue in males. It has a bimodal age distribution, with a peak in adolescence (physiological pubertal gynecomastia) due to the temporary imbalance between estrogen and androgen during puberty. It typically presents as a firm or rubbery subareolar mass and is bilateral in most adolescent cases. It is usually self-limiting and resolves within 1-2 years. Pathological causes to exclude include Klinefelter syndrome, adrenal tumors, testicular tumors, liver disease, and drug use. - Current Surgical Therapy 14e
Accessory / Ectopic Breast Tissue (Polymastia / Polythelia)
Accessory breast tissue results from incomplete regression of the embryonic milk line (which extends from the axilla to the groin). It is most commonly found above the breast in the axilla and may present as an enlarging mass during puberty or pregnancy. Polythelia (supernumerary nipples) is the most common anomaly. Rarely symptomatic in childhood; management is usually conservative or cosmetic excision.
3. Benign Breast Lesions
Fibroadenoma (Most Common)
Fibroadenoma is the most common breast lesion in the pediatric and adolescent age group, accounting for approximately 95% of all breast masses in this population.
Epidemiology: Most common in women aged 15-25 years. The pericanalicular (hard) variety is particularly common in young girls aged 15-30 years. In women under 25, fibroadenomas are more common than cysts.
Pathology: Two histological types:
- Pericanalicular fibroadenoma - fibrous tissue surrounding small tubular glands; smaller and harder; predominates in young women.
- Intracanalicular fibroadenoma - glands stretched into elongated spidery shapes, indented by fibrous tissue; softer and larger; more common in middle-aged women. Both represent a benign proliferation of epithelial and stromal components arising from a single lobule. - S. Das Manual on Clinical Surgery, p. 434
Clinical features:
- Painless, slow-growing lump
- Smooth, firm, well-defined margins
- Not fixed to skin or deep structures
- Highly mobile - classically called a "breast mouse" or "floating tumour"
- No axillary lymphadenopathy
- Usually 1-3 cm at presentation; may rarely grow larger
Giant Fibroadenoma / Juvenile Fibroadenoma:
A fibroadenoma >5 cm is termed a giant fibroadenoma. These occasionally occur during puberty, grow rapidly, and can cause significant breast asymmetry. They can be enucleated through a submammary incision. - Bailey & Love's Short Practice of Surgery, p. 58.14
Imaging: Ultrasound (the preferred modality in this age group) shows a well-circumscribed, solid, oblong mass with clearly defined margins. BI-RADS 3 appearance is typical.
Natural history: About 15% regress spontaneously; 5-10% grow. Most stabilize at 2-3 cm.
Malignant risk: No increased risk with simple fibroadenoma. Complex fibroadenoma with family history carries a relative risk (RR) of 3.0-4.0, particularly for lobular carcinoma. - Bailey & Love
Management:
- A clinically typical fibroadenoma confirmed on ultrasound in a patient under 25 years can be observed without biopsy.
- Biopsy is indicated if: age >25, atypical imaging features, rapid growth.
- Indications for surgical excision: age >30, suspicious features, atypia on histology, size >5 cm, family history of breast cancer, or patient preference.
- In children and adolescents, the preferred approach is conservative observation with ultrasound every 6-12 months. - Frontiers in Pediatrics, PMID 39507494
Solitary Breast Cyst
Less common than in adults. A solitary cyst presents as the "blue-domed cyst of Bloodgood." Diagnosed by fluctuation test or ultrasound. Aspiration is both diagnostic and therapeutic. Benignity is confirmed if: aspirate is not blood-stained, no residual lump after aspiration, cyst does not refill, and cytology is negative for malignancy. - S. Das, p. 434
Galactocele
A rare milk-filled cyst, typically subareolar, seen during or just after lactation. Usually cured by single aspiration. Rarely requires surgical excision.
Breast Abscess / Mastitis
Neonatal mastitis can occur in the first few weeks of life due to maternal estrogen stimulation. Adolescent mastitis may follow ductal obstruction or infection. Presents with pain, erythema, swelling, and fever. Managed with antibiotics; incision and drainage if abscess forms. Surgical drainage must be performed carefully to avoid damage to the breast bud.
Duct Papilloma
An intraductal papillary lesion, usually arising in one of the major ducts. Presents with blood-stained nipple discharge. Can occur in adolescents. Management is microdochectomy (excision of the affected duct).
4. Fibroepithelial Lesions
Phyllodes Tumor (Cystosarcoma Phyllodes)
Phyllodes tumors are rare fibroepithelial tumors comprising both epithelial and mesenchymal elements. They represent <0.5% of all breast tumors. Although more common in women in their late 30s-50s, they can occur in younger women and adolescents. - Mulholland & Greenfield's Surgery, p. 3976
Classification by histology:
| Grade | Mitotic Rate | Proportion |
|---|---|---|
| Benign | <4 per 10 HPF | ~50-60% |
| Borderline | 4-9 per 10 HPF | ~20-25% |
| Malignant | >10 per 10 HPF | ~20-25% |
Classification also considers stromal cellularity, atypia, stromal overgrowth, and infiltrative margins.
Clinical features:
- Smooth, multinodular, well-demarcated, firm, mobile and painless mass
- Average size 4-7 cm; can be massive
- Overlying skin may be stretched and tense; subcutaneous veins become prominent
- Skin ulceration may occur from pressure necrosis in very large tumors (not true invasion)
- Rarely infiltrates skin until late; remains mobile on the chest wall
- Palpable axillary nodes in up to 20% but true lymph node involvement is rare

Key distinction from fibroadenoma: A previously stable nodule that suddenly increases in size is the classic history pointing toward phyllodes.
Imaging: Smooth, multi-lobulated mass resembling fibroadenoma. Core needle biopsy is recommended but has a false-negative rate of 25-30%; excisional biopsy is preferred for rapidly enlarging masses.
Metastasis: Malignant phyllodes tumors spread hematogenously, primarily to lungs (similar to sarcomas). Lymph node spread is rare.
Management:
- All grades: surgical excision to negative histological margins
- Breast-conserving surgery is appropriate even for large tumors
- SLNB is not routinely performed
- Adjuvant radiotherapy/chemotherapy: controversial; may be considered for large borderline or malignant tumors
- Post-treatment follow-up: chest X-ray every 6 months for 2 years, then annually for malignant phyllodes
- Systemic therapy for metastatic disease follows sarcoma protocols
- Mulholland & Greenfield, p. 3977; Berek & Novak, p. 985
5. Malignant Breast Lesions
Primary breast carcinoma in children and adolescents is extremely rare. However, malignancy must always be considered in the differential.
Primary Breast Carcinoma
- Rare before age 18; incidence increases after puberty
- Secretory (juvenile) carcinoma is the most common type in children - a low-grade carcinoma with relatively favorable prognosis
- Other types: infiltrating ductal carcinoma (rare), adenocarcinoma
- Risk factors in pediatric patients include: prior thoracic radiation (e.g., for lymphoma), hereditary syndromes (BRCA1/2, Li-Fraumeni syndrome, Cowden syndrome/PTEN hamartoma)
Secondary / Metastatic Involvement
The breast may be secondarily involved by hematological malignancies or other pediatric tumors. Rhabdomyosarcoma, non-Hodgkin lymphoma, and leukemic infiltrates should be considered when a breast mass occurs in a child with a known malignancy.
Breast Implant-Associated Anaplastic Large Cell Lymphoma (BIA-ALCL)
This is a rare T-cell lymphoma associated with textured breast implants. It can present as a pericapsular seroma or a discrete mass. While more relevant to adults, it is worth knowing for patients who have received implants.
6. Diagnostic Approach
History: Age, rate of growth (rapid growth favors phyllodes or malignancy), pain, nipple discharge, systemic symptoms, family history of breast cancer, radiation history.
Physical exam: Characteristics of the mass (mobile vs. fixed, soft vs. firm, smooth vs. irregular), skin changes, nipple discharge, lymphadenopathy.
Imaging - Ultrasound is the primary modality in children and adolescents (no radiation, excellent soft tissue resolution, avoids unnecessary radiation to developing glandular tissue). Mammography is reserved for selected older adolescents when malignancy is suspected. MRI is used in specific cases (e.g., BRCA carriers, implant evaluation).
Biopsy:
- Core needle biopsy (CNB) is the standard for tissue diagnosis when needed.
- Excisional biopsy is preferred over CNB in children when feasible, to minimize sampling error and to preserve breast architecture.
- Fine needle aspiration cytology (FNAC) is less preferred due to limited tissue.
Algorithm (APSA 2025 guidelines): Evaluation begins with history and physical exam → ultrasound-guided algorithm for palpable masses → observation without resection is appropriate for most presumed benign lesions → surgical management when indicated should conserve developing breast tissue and nipple-areolar complex. - Journal of Pediatric Surgery, PMID 39384492
7. Key Principles of Management in Children and Adolescents
- Conservative approach first: Most lesions in this age group are benign and can be managed with watchful waiting and serial ultrasound.
- Protect the breast bud: Never inadvertently excise the breast bud when draining an abscess or removing a periareolar mass in a prepubertal girl.
- Multidisciplinary team: Malignant lesions require pediatric oncology, surgery, radiation oncology, and pathology input.
- Patient and family counseling: Education about breast self-examination and when to seek attention for new or changing masses.
- Imaging choice: Ultrasound first; avoid mammography in this population unless malignancy is strongly suspected.
- Surgical conservatism: When excision is necessary, aim for enucleation or local excision with minimal tissue sacrifice to preserve cosmesis and lactation potential.
Summary Table
| Lesion | Age Peak | Character | Key Feature | Management |
|---|---|---|---|---|
| Premature thelarche | <2-4 years | Bilateral soft enlargement | No nipple/areolar development | Reassurance, follow-up |
| Fibroadenoma | 15-25 years | Firm, mobile, smooth | "Breast mouse"; painless | Observe; excise if >5 cm or atypical |
| Giant/Juvenile fibroadenoma | Puberty | >5 cm, rapidly growing | Puberty onset | Enucleation |
| Phyllodes tumor | 30s-50s; adolescent possible | Bosselated, rapid growth | Previously stable, then rapid enlargement | Excision to negative margins |
| Breast abscess | Neonatal/adolescent | Tender, erythema, fever | Inflammatory signs | Antibiotics, drainage (careful) |
| Breast carcinoma | Rare in <18 years | Fixed, irregular | Prior radiation, BRCA | Multidisciplinary, sarcoma-like for phyllodes |
Recent evidence (2024-2025):
- A 2024 scoping review (Sosnowska-Sienkiewicz et al., Frontiers in Pediatrics, PMID 39507494) confirmed fibroadenomas account for ~95% of all pediatric breast lesions, advocated conservative management with ultrasound surveillance every 6-12 months for most cases, and emphasized that excisional biopsy should be reserved for complex or suspicious clinical/imaging scenarios.
- The 2025 APSA Cancer Committee expert consensus (Schwartz et al., J Pediatr Surg, PMID 39384492) provides an algorithm for pediatric surgeons emphasizing ultrasound-first evaluation, tissue preservation, and multidisciplinary management of the rare malignant lesion.
Papillary lesions of breast
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
papillary lesions breast pathology management
Finding Sources
Finding Sources
Reading Article
Reading Article
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the material needed for a comprehensive answer. Let me compile it.
Papillary Lesions of the Breast
Papillary lesions of the breast form a spectrum ranging from entirely benign intraductal papillomas to frankly malignant invasive papillary carcinoma. They are unified by a defining histological feature: epithelial proliferations supported by fibrovascular stalks or cores, forming true papillae (finger-like projections) within ducts or cysts. They are often grouped under the "B3" category (lesions of uncertain malignant potential) when encountered on core needle biopsy, which creates important management implications.
Classification Overview
Papillary lesions of the breast are broadly categorized as:
| Category | Lesion |
|---|---|
| Benign | Intraductal papilloma (solitary or multiple/peripheral) |
| Atypical | Papilloma with atypical ductal hyperplasia (ADH) |
| In situ | Papillary DCIS, Micropapillary DCIS |
| Borderline / In situ vs. invasive | Encapsulated papillary carcinoma (EPC), Solid papillary carcinoma (SPC) |
| Invasive | Invasive papillary carcinoma, Invasive micropapillary carcinoma |
1. Intraductal Papilloma (Benign)
Definition
An intraductal papilloma is a benign epithelial lesion with supporting stroma that grows within a duct, forming true papillae with fibrovascular cores lined by both luminal epithelial cells and a myoepithelial cell layer. The presence of myoepithelial cells is the hallmark distinguishing benign papilloma from malignant papillary lesions.
Epidemiology and Types
Solitary (Central) Papilloma:
- Most common type; arises in the large lactiferous ducts near the nipple
- Occurs predominantly in women 30-50 years of age
- The most common cause of bloody/serous nipple discharge
- Generally not associated with increased cancer risk
- Presents as a small soft mass just deep or lateral to the areola
Multiple (Peripheral) Papillomas:
- Arise in the terminal duct lobular unit (TDLU), peripheral to the nipple
- More likely to be bilateral
- Associated with a modestly increased risk of breast cancer (relative risk ~1.5-2x) compared to central papillomas
- May harbor atypical epithelial hyperplasia within them
Clinical Features
- Nipple discharge is the hallmark: spontaneous, unilateral, from a single ductal orifice
- Discharge character: serous, serosanguineous, or frankly bloody (bright red)
- A trigger point (localized pressure point) may be identified on the breast
- Occult blood test on the discharge is often positive
- A small, soft, cystic mass may be palpable just beneath/lateral to the areola
- Axillary lymphadenopathy is absent (unless malignant transformation has occurred)
- Considered pre-malignant if features of atypia are present - S. Das Manual on Clinical Surgery, p. 434
Important: Distinguishing Pathologic from Physiologic Discharge
Pathologic nipple discharge is:
- Spontaneous (not elicited)
- Unilateral and from a single duct orifice
- Bloody, serous, or serosanguineous
- Associated with a mass
Age predicts malignancy risk in nipple discharge: cancer found in ~3% of women <40 years, ~10% in those 40-60 years, and ~32% in women over 60 years. - Mulholland & Greenfield's Surgery, p. 3897
Physiologic discharge (milky, bilateral, multiductal, elicited) is not worrying and should prompt evaluation for galactorrhea (prolactin, thyroid, medications).
Investigations
- Mammography and ultrasound are first-line imaging
- Breast MRI with contrast has largely replaced ductography as the investigation of choice for pathologic nipple discharge
- Ductography (galactography): contrast instilled into the involved duct; shows filling defect, ductal irregularity, or complete obstruction - valuable when MRI is unavailable
- Ductoscopy: fiberoptic scope placed into the duct for direct visualization; allows more precise excision localization
- Core needle biopsy: when a lesion is identified on imaging; however, excision is still recommended even after benign CNB result
Histopathology
- True fibrovascular cores lined by two cell layers: inner luminal epithelial cells and outer myoepithelial cells
- Myoepithelial cells are retained (key distinction from malignant papillary lesions)
- IHC: positive for myoepithelial markers (p63, calponin, smooth muscle actin, CK5/6) along the stalk and at the periphery
Management
- When a papilloma is diagnosed on core biopsy, surgical excision is the standard recommendation, as it may be associated with atypia or DCIS in the adjacent tissue
- Surgical technique:
- Pressure applied around nipple to identify the discharging duct
- Lacrimal duct probe placed into the affected duct
- Duct excised via a periareolar incision (microdochectomy)
- If single duct cannot be identified, a central duct excision (Hadfield's operation) is performed
- Methylene blue dye can be injected after ductography to stain the duct for easier localization
- Women of reproductive age should be counseled about potential difficulty breastfeeding following central duct excision - Mulholland & Greenfield's Surgery; Current Surgical Therapy 14e
2. Papilloma with Atypical Ductal Hyperplasia (ADH)
A papilloma may contain foci of ADH within its substance. This combination carries a higher risk for subsequent invasive carcinoma (relative risk ~4-5x baseline). Management requires complete surgical excision with close follow-up. On core needle biopsy showing a papilloma + ADH, surgical excision reveals DCIS or invasive carcinoma in approximately 10-20% of cases. - Robbins Pathologic Basis of Disease, p. 967
3. Papillary DCIS and Micropapillary DCIS (In Situ)
Papillary DCIS
- Ductal carcinoma in situ growing in a true papillary pattern: papillae with fibrovascular cores
- Key distinction from benign papilloma: the papillae in papillary DCIS lack a myoepithelial cell layer - this is the most important diagnostic feature
- The cells lining the papillae are monotonous, cytologically atypical, and there is no admixed myoepithelial cell population
- Often ER-positive, HER2-negative (low-grade pathway)
- May present as nipple discharge or be detected incidentally on imaging
Micropapillary DCIS
- A distinct architectural subtype of DCIS characterized by bulbous, club-shaped projections without fibrovascular cores (pseudo-papillae)
- The projections have no true fibrovascular stalk - this distinguishes it from true papillary DCIS
- More commonly multicentric and tends to involve larger areas of breast tissue, making margin assessment more difficult
- Can present as nipple discharge
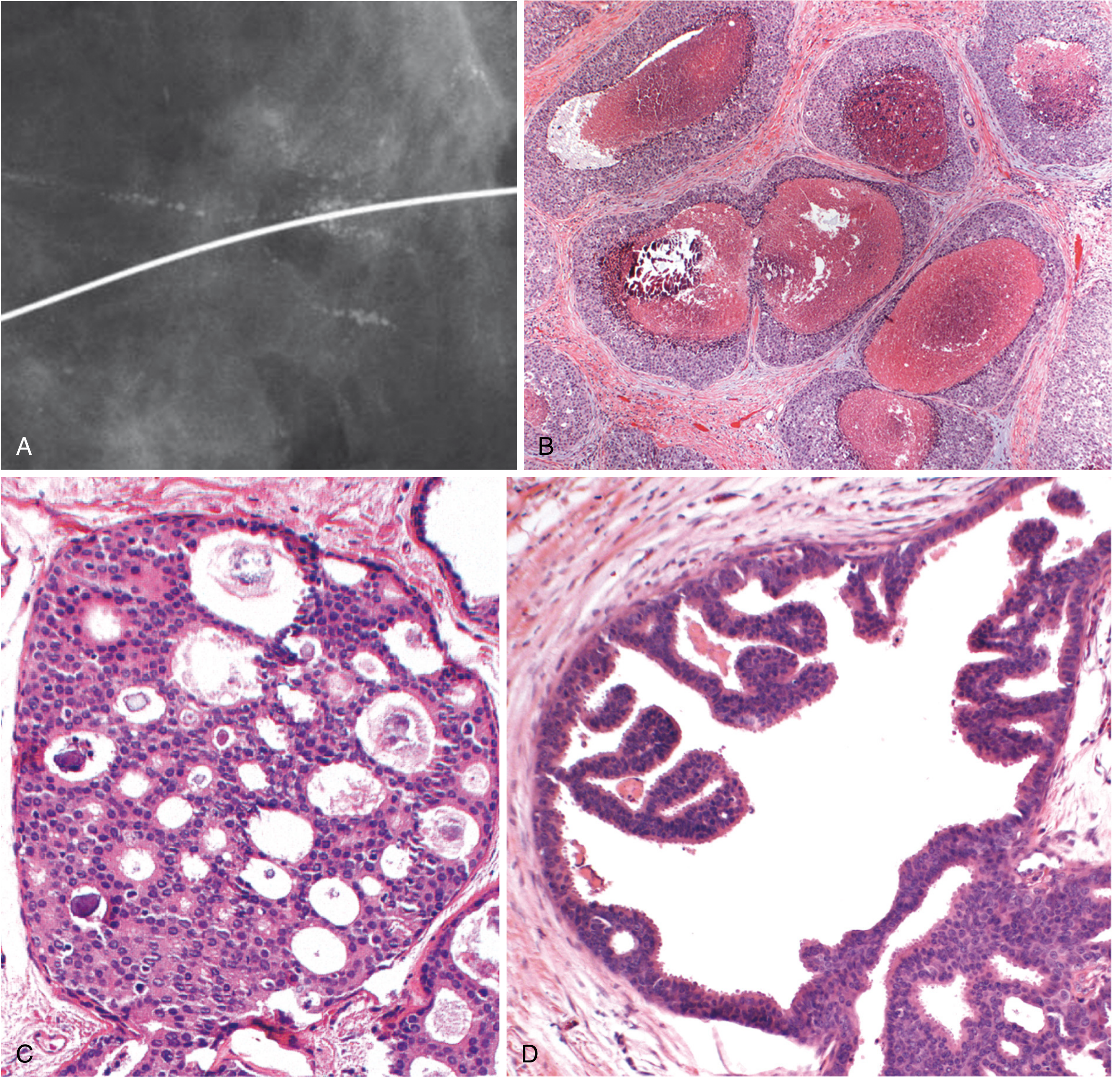
4. Encapsulated Papillary Carcinoma (EPC)
Formerly called intracystic papillary carcinoma, this entity is one of the most diagnostically challenging papillary lesions.
Morphology
- A papillary carcinoma enclosed within a fibrous capsule, without invasion of surrounding breast parenchyma
- The papillae are lined by low-grade atypical epithelial cells lacking myoepithelial cells (both on the stalks and at the periphery of the lesion)
- Absence of myoepithelial cells throughout is demonstrated by IHC (negative for p63, CK5/6, smooth muscle actin)
Controversy: In Situ or Invasive?
- One of the most debated areas in breast pathology (see [Rakha & Quinn, Histopathology 2025, PMID 39209705])
- Morphologically resembles in situ carcinoma (contained within capsule), but the absence of myoepithelial cells suggests it may represent an extremely low-grade form of invasive carcinoma
- Current WHO classification treats EPC as in situ unless there is clear invasion of surrounding stroma
- Prognosis is excellent regardless of designation
Clinical Features
- Typically presents as a palpable mass, sometimes with nipple discharge
- More common in older, postmenopausal women
- On imaging: well-circumscribed, cystic-solid mass; can be quite large
Management
- Surgical excision with clear margins
- Sentinel lymph node biopsy is generally not required for pure EPC
- Adjuvant therapy follows the usual guidelines for DCIS/early breast cancer (usually endocrine therapy given ER positivity)
5. Solid Papillary Carcinoma (SPC)
- A variant where the papillary fronds are so tightly packed that the lesion appears solid on low-power microscopy
- Often shows neuroendocrine differentiation (synaptophysin, chromogranin positive)
- Lacks myoepithelial cells
- May produce mucin (overlap with mucinous carcinoma)
- Like EPC, the in situ vs. invasive distinction is debated
- Often ER-positive, with a generally favorable prognosis
- Can be confused with invasive lobular carcinoma on biopsy - Hoda & Wen, Human Pathology 2025, PMID 40118257
6. Invasive Papillary Carcinoma
Epidemiology
- A special histological type of invasive breast carcinoma accounting for 2% of all invasive breast cancers
- Presents characteristically in the seventh decade of life
- Occurs disproportionately in non-white women
Morphology
- Defined by true papillary fronds with fibrovascular cores lined by multilayered atypical epithelium infiltrating beyond the duct walls into breast stroma
- Papillae are lined by malignant cells without myoepithelial cells
- Usually small tumors, rarely attaining >3 cm
- Typically ER-positive: ~87% express estrogen receptor (SEER data)
Behavior
- Low frequency of axillary lymph node metastases - one of the most favorable special types
- 5- and 10-year survival rates are similar to mucinous carcinoma and tubular carcinoma (both excellent prognoses among special-type cancers) - Schwartz's Principles of Surgery, p. 593
Management
- Breast-conserving surgery or mastectomy depending on tumor size and patient preference
- Axillary staging (SLNB) recommended
- Adjuvant endocrine therapy for ER-positive tumors
7. Invasive Micropapillary Carcinoma
This is a distinct and clinically aggressive entity - it is a misnomer in that the micropapillary structures it forms are not true papillae.
Morphology
- Tumor cells form hollow balls ("morulae") that appear to float within intercellular fluid-filled spaces, mimicking papillae but without fibrovascular cores
- The cells show reversed polarity (apical surfaces face outward, toward the stroma - the "inside-out" pattern)
- This reversed polarity is demonstrated by EMA (epithelial membrane antigen) staining on the outside of the cell clusters
Clinical Behavior
- More aggressive than ordinary invasive carcinoma of no special type
- High rate of lymphovascular invasion and lymph node metastases
- Tends to overexpress HER2
- Management follows standard protocols for invasive carcinoma but with attention to aggressive locoregional management
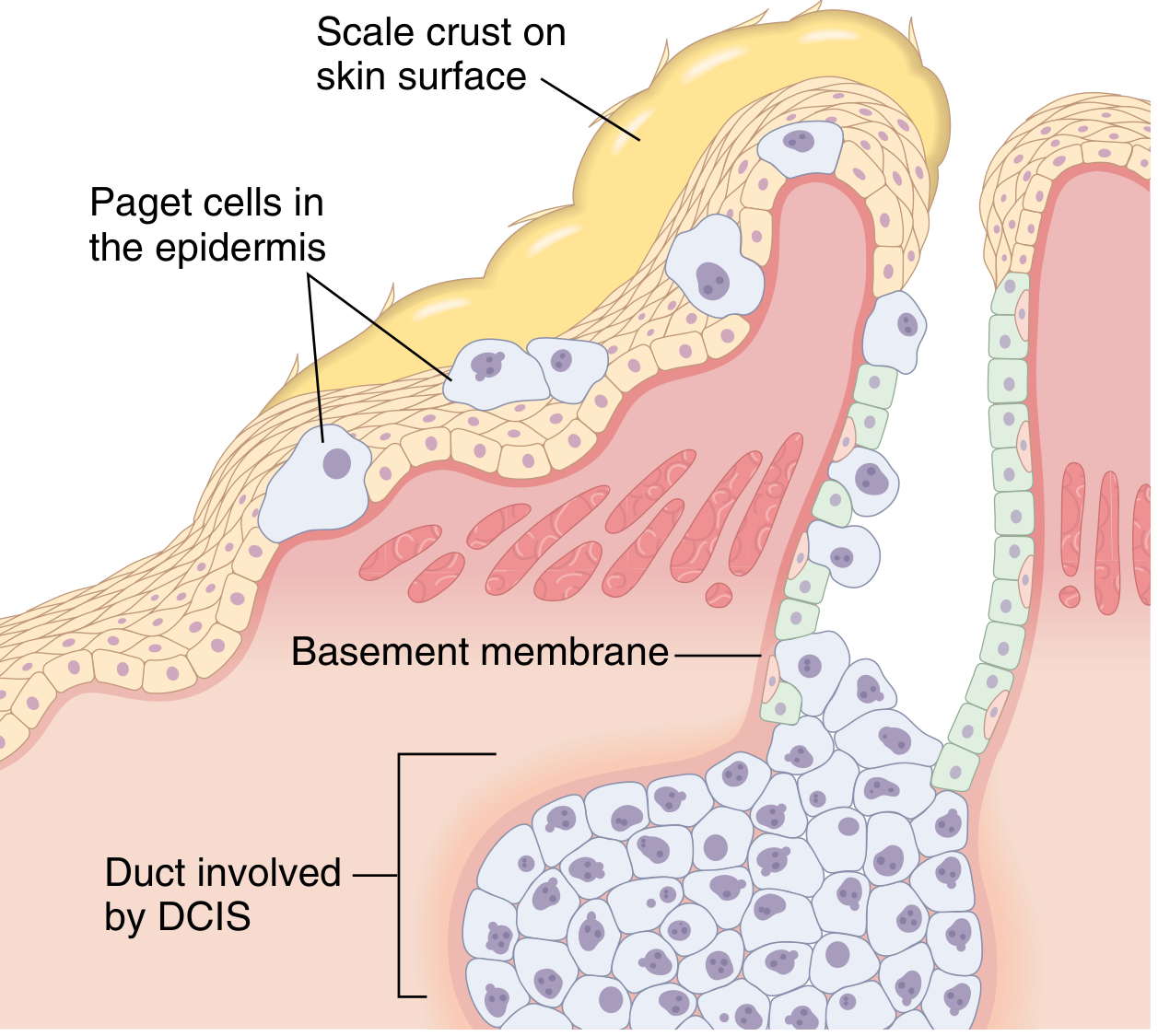
8. Paget's Disease of the Nipple (Papillary/Ductal Extension)
Although not strictly a "papillary lesion," Paget's disease represents the intraepidermal extension of underlying DCIS (often of papillary/micropapillary type) along the lactiferous ducts into the nipple skin.
- Presents as a chronic eczematous, erythematous, scaling eruption of the nipple with pruritus
- Pathognomonic: large, pale, vacuolated Paget cells in the rete pegs of the epidermis
- Paget cells are identical to the underlying DCIS cells (pagetoid change)
- ~50% of patients have a palpable mass (usually associated with invasive carcinoma)
- Without a palpable mass, underlying DCIS is the rule
- IHC distinction: CK7+ and CEA+ (Paget's) vs. S-100+ (melanoma - which it can mimic)
Key Diagnostic Distinguishing Features
| Feature | Benign Papilloma | Papillary DCIS | EPC / SPC | Invasive Papillary Ca |
|---|---|---|---|---|
| Myoepithelial cells | Present (on stalks + periphery) | Absent | Absent | Absent |
| Fibrovascular cores | Yes | Yes | Yes | Yes |
| Cell layer | Two (luminal + myoepithelial) | Monotonous single layer | Monotonous single layer | Monotonous single layer |
| Capsule | No | No | Yes | No (invasive) |
| IHC (p63/CK5) | Positive | Negative | Negative | Negative |
| Invasion of stroma | No | No | Debated | Yes |
| ER status | Positive | Often positive | Often positive | ~87% positive |
| Prognosis | Excellent | Excellent | Excellent | Very good |
The "B3" Problem: Papilloma on Core Needle Biopsy
Papillary lesions on CNB are classified as B3 (lesion of uncertain malignant potential) by European guidelines. This is because:
- Sampling error on CNB may miss associated atypia or DCIS
- Even a benign-appearing papilloma on CNB may harbor atypia at surgical excision
- The 2024 EUSOMA/EUSOBI/ESP guidelines (Rubio et al., PMID 38061151) recommend surgical excision for most papillary lesions on CNB, with observation acceptable only for small (<1 cm), incidentally found peripheral papillomas without atypia, after multidisciplinary discussion
Summary of Management
| Lesion | Primary Management |
|---|---|
| Solitary intraductal papilloma | Microdochectomy / surgical duct excision |
| Multiple peripheral papillomas | Excision; enhanced surveillance |
| Papilloma with ADH on CNB | Surgical excision mandatory |
| Papillary DCIS | Wide local excision + radiotherapy; endocrine therapy if ER+ |
| EPC (pure) | Wide local excision; SLNB generally not required |
| SPC (pure) | Wide local excision; treat as DCIS |
| Invasive papillary carcinoma | BCS or mastectomy + SLNB + adjuvant therapy |
| Invasive micropapillary carcinoma | Standard invasive carcinoma treatment; aggressive locoregional approach |
| Paget's disease | Nipple excision (if confined) or mastectomy depending on extent |
Recent evidence updates (2025):
- A 2025 pathology review (Hoda & Wen, Human Pathology, PMID 40118257) highlights persistent challenges in diagnosing SPC and EPC on CNB, noting overlap with invasive lobular carcinoma as a major pitfall, and stresses that a "fibroepithelial lesion" or papillary pattern on CNB always warrants excision.
- Rakha & Quinn, Histopathology 2025, PMID 39209705 provides a framework for EPC categorization and addresses the unresolved in situ vs. invasive debate, recommending that pathologists apply IHC for myoepithelial markers systematically and recognize morphologic overlap with high-grade circumscribed invasive carcinomas.
Prognostic markers in breast carcinoma
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
breast cancer prognostic biomarkers molecular subtypes
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Loading Image
Finding Sources
I now have comprehensive material from the library and PubMed. Let me compile the full answer.
Prognostic Markers in Breast Carcinoma
Prognostic markers are factors that provide information about the likely natural history of a cancer - they predict outcomes (recurrence, survival) independently of treatment. In breast cancer, they are distinct from predictive markers (which predict response to a specific therapy), though many markers serve both functions. The AJCC 8th edition staging system now incorporates both anatomic and biologic (molecular) prognostic factors.
Classification of Prognostic Markers
Breast cancer prognostic markers fall into three broad categories:
- Clinicopathological markers - tumor size, lymph node status, histological grade, histological type, lymphovascular invasion
- Biomarker/IHC markers - hormone receptors (ER, PR), HER2, Ki67, p53
- Molecular/genomic markers - gene expression profiling (Oncotype DX, MammaPrint, PAM50), molecular subtypes
I. Clinicopathological Prognostic Markers
1. Axillary Lymph Node Status
The single most powerful prognostic indicator in breast cancer.
- Node-negative disease: 10-year survival ~70-80%
- 1-3 positive nodes (pN1): significantly worse prognosis
- 4-9 positive nodes (pN2): markedly worse
- ≥10 positive nodes (pN3): poorest prognosis in this category
The number of involved axillary nodes correlates with the occurrence of distant metastases and is one of the most important predictors of 10- and 20-year survival rates. Accurate assessment requires pathological analysis of ≥10 Level I and II axillary nodes for maximum prognostic information. Even the internal mammary nodes and low axillary nodes carry prognostic weight: when both an internal mammary and low axillary node are positive, prognosis declines to the level associated with apical node positivity. - Schwartz's Principles of Surgery, p. 602
Nodal micrometastases (pN0(i+)): Isolated tumour cells ≤0.2 mm are included in staging but their independent prognostic significance remains uncertain.
2. Tumor Size (T Stage)
Tumor size correlates with axillary lymph node metastases and disease-free survival:
| T Stage | Size | Description |
|---|---|---|
| T1mi | ≤1 mm | Microinvasion |
| T1a | >1 to ≤5 mm | - |
| T1b | >5 to ≤10 mm | - |
| T1c | >10 to ≤20 mm | - |
| T2 | >20 to ≤50 mm | - |
| T3 | >50 mm | - |
| T4 | Any size + chest wall/skin | - |
Larger tumors have higher rates of nodal positivity and distant recurrence. However, tumor size must be interpreted in the context of nodal status - small tumors with nodal involvement can behave more aggressively than larger node-negative tumors.
3. Histological Grade (Nottingham Grading System)
All invasive breast carcinomas are graded using the Nottingham Histologic Score based on three parameters, each scored 1-3:
| Parameter | Score 1 | Score 2 | Score 3 |
|---|---|---|---|
| Tubule formation | >75% of tumor | 10-75% | <10% |
| Nuclear pleomorphism | Small, uniform | Moderate variation | Marked variation |
| Mitotic rate | Low (count/HPF) | Intermediate | High |
Total score:
- 3-5 = Grade 1 (well differentiated) - best prognosis
- 6-7 = Grade 2 (moderately differentiated) - intermediate prognosis
- 8-9 = Grade 3 (poorly differentiated) - worst prognosis
Grade 3 tumors are associated with high Ki67, ER negativity, lymph node metastases, and reduced overall survival. - Robbins Pathologic Basis of Disease, p. 978
4. Histological Type / Special Type
Special-type carcinomas (which must consist ≥90% of the defining histology) generally have a better prognosis than invasive carcinoma of no special type (NST):
| Type | Proportion | Prognosis |
|---|---|---|
| NST (ductal NOS) | 80% | Intermediate (varies with grade) |
| Tubular carcinoma | 2% | Excellent - distant mets rare |
| Mucinous (colloid) carcinoma | 2% | Favorable; 5-yr survival 73% |
| Papillary carcinoma | 2% | Very favorable; low nodal involvement |
| Invasive lobular | 10-15% | Variable; often ER+ |
| Medullary pattern | 4% | Paradoxically better despite high grade |
| Metaplastic carcinoma | <1% | Poor; usually TNBC |
| Invasive micropapillary | <1% | Aggressive; high LVI, LN mets |
Long-term survival for tubular and papillary carcinoma approaches 100%, while metaplastic carcinoma carries a markedly worse outcome. - Schwartz's Principles of Surgery, p. 593
5. Lymphovascular Invasion (LVI)
The presence of tumor emboli within lymphatic or blood vessel channels is an independent adverse prognostic factor:
- Predicts lymph node positivity even when nodes appear negative
- Associated with higher risk of systemic recurrence
- Particularly significant in node-negative patients (upstages risk)
- Strong indicator for adjuvant chemotherapy in otherwise low-risk cases
6. Margins of Excision
Positive surgical margins (tumor at ink) predict locoregional recurrence after breast-conserving surgery and are associated with worse disease-specific survival. Re-excision or mastectomy is indicated for positive margins.
II. Biomarker / Immunohistochemical Prognostic Markers
All invasive breast cancers must be tested for ER, PR, and HER2 at the time of primary diagnosis.
1. Estrogen Receptor (ER) and Progesterone Receptor (PR)
Measured by: IHC on FFPE tissue; reported as % of nuclei staining positive and staining intensity (Allred score or H-score). Positive threshold: ≥1% nuclear staining (ASCO/CAP guidelines).
Prognostic significance:
- ER/PR positivity predicts a more favorable long-term prognosis (though early outcome may be similar)
- Patients with hormone receptor-positive tumors survive 2-3 times longer after a diagnosis of metastatic disease than patients with hormone receptor-negative tumors
- ER/PR-negative status is associated with higher grade, higher Ki67, earlier relapse, and worse 5-year survival
Predictive significance:
- ER positivity predicts benefit from endocrine therapy (tamoxifen, aromatase inhibitors)
- PR positivity confirms a functional ER pathway
- ER-/PR+ is rare; ER+/PR- has intermediate hormonal sensitivity
- Tumors negative for both ER and PR are not candidates for endocrine therapy
Testing should be performed on all primary invasive breast cancers (both premenopausal and postmenopausal). - Schwartz's Principles of Surgery, p. 605
2. HER2 (Human Epidermal Growth Factor Receptor 2 / ErbB2)
HER2 is a transmembrane tyrosine kinase receptor. HER2 amplification or overexpression occurs in approximately 15-20% of breast cancers.
Testing methods:
- IHC (protein overexpression): scored 0, 1+, 2+, 3+
- 0 or 1+ = negative
- 2+ = equivocal → reflex FISH/ISH testing
- 3+ = positive (>10% complete, intense membrane staining)
- FISH/CISH (gene amplification): ratio of HER2 gene signals to chromosome 17 centromere signals ≥2.0 = amplified
Prognostic significance:
- HER2 overexpression/amplification is associated with:
- Poorly differentiated tumors with high proliferation rates
- Higher incidence of positive lymph nodes
- Decreased hormone receptor expression
- Increased risk of recurrence and death
- More aggressive clinical behavior
- Before anti-HER2 therapy: HER2+ was one of the worst prognostic subtypes
- With trastuzumab + pertuzumab: outcomes have dramatically improved (40-50% reduction in recurrence risk)
Emerging category - HER2-low (IHC 1+ or 2+/FISH non-amplified): Now recognized as a separate therapeutic target for trastuzumab deruxtecan (T-DXd). - PMID 38291745 (Kang & Kim, 2024)
HER2 testing should be performed on all invasive breast cancers. - Schwartz's Principles of Surgery, p. 605
3. Ki67 (Proliferation Index)
Ki67 is a nuclear protein expressed in all phases of the cell cycle except G0 (rest). It is the most widely used marker of tumor proliferation.
- Measured by: IHC, expressed as percentage of positively staining tumor cells
- Thresholds:
- Low: <15-20%
- High: >20-30% (cut-offs vary by institution; international consensus seeks standardization)
Prognostic significance:
- High Ki67 correlates with:
- High histological grade
- ER negativity
- p53 overexpression
- Aneuploidy and high S-phase fraction
- Lymph node metastases
- Worse disease-free and overall survival
- Ki67 forms part of the IHC4 panel (ER, PR, HER2, Ki67) that provides prognostic information comparable to the 21-gene Oncotype DX recurrence score, at lower cost - though reproducibility across labs remains a limitation
- Ki67 is key in distinguishing Luminal A (Ki67 <20%) from Luminal B (Ki67 ≥20%) subtypes - Schwartz's Principles of Surgery, p. 606
4. p53 / TP53
- p53 overexpression (by IHC) reflects mutant p53 accumulation due to loss of normal ubiquitin-mediated degradation
- Mutant TP53 is found in ~20-30% of breast cancers overall; ~80% of TNBC
- Associated with: high grade, ER negativity, lymph node metastases, high Ki67, high S-phase fraction, and reduced overall survival
- p53 overexpression predicts worse outcome, particularly in node-negative disease
- An angiogenesis index combining microvessel density (CD31), thrombospondin, and p53 has been developed as a composite prognostic tool
5. bcl-2 and Apoptosis Markers
- bcl-2 (anti-apoptotic protein): paradoxically, bcl-2 expression in breast cancer is associated with ER positivity and better prognosis (inverse to its oncogenic role in lymphoma)
- bax (pro-apoptotic): decreased bax expression correlates with lymph node metastases, poor chemotherapy response, and decreased overall survival
- The bax:bcl-2 ratio influences whether cells undergo apoptosis; overexpression of bcl-2 and a decreased bax:bcl-2 ratio correlate with high grade, lymph node positivity, and reduced survival
- Schwartz's Principles of Surgery, p. 691
6. Angiogenesis Markers (VEGF / Microvessel Density)
- VEGF (vascular endothelial growth factor) overexpression in invasive breast cancer correlates with increased microvessel density and recurrence, particularly in node-negative disease
- A combined angiogenesis index (microvessel density by CD31 + thrombospondin + p53) has prognostic value
- Currently used primarily in research; bevacizumab (anti-VEGF) did not produce durable clinical benefit in trials and is no longer routinely used in breast cancer
7. EGFR (Epidermal Growth Factor Receptor / HER1)
- EGFR overexpression correlates with:
- ER-negative status
- p53 overexpression
- Higher grade
- Worse prognosis
- EGFR expression is a hallmark of basal-like/TNBC (basal cytokeratins CK5/6 + EGFR positivity defines a subgroup with particularly poor outcomes)
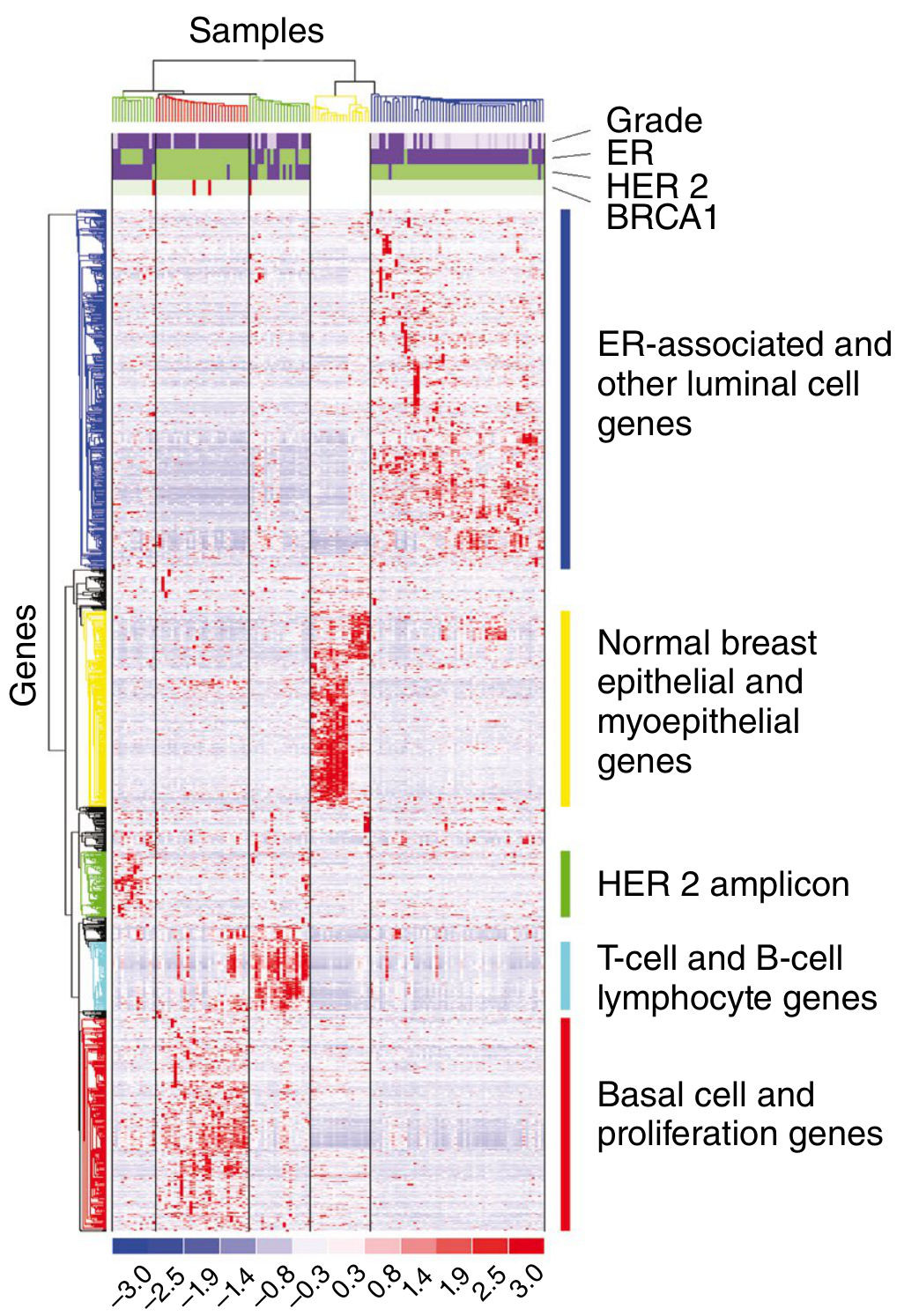
III. Molecular Subtypes (Gene Expression Profiling)
Unsupervised gene expression profiling has divided breast cancer into four major intrinsic molecular subtypes with distinct biological behavior and clinical outcomes.
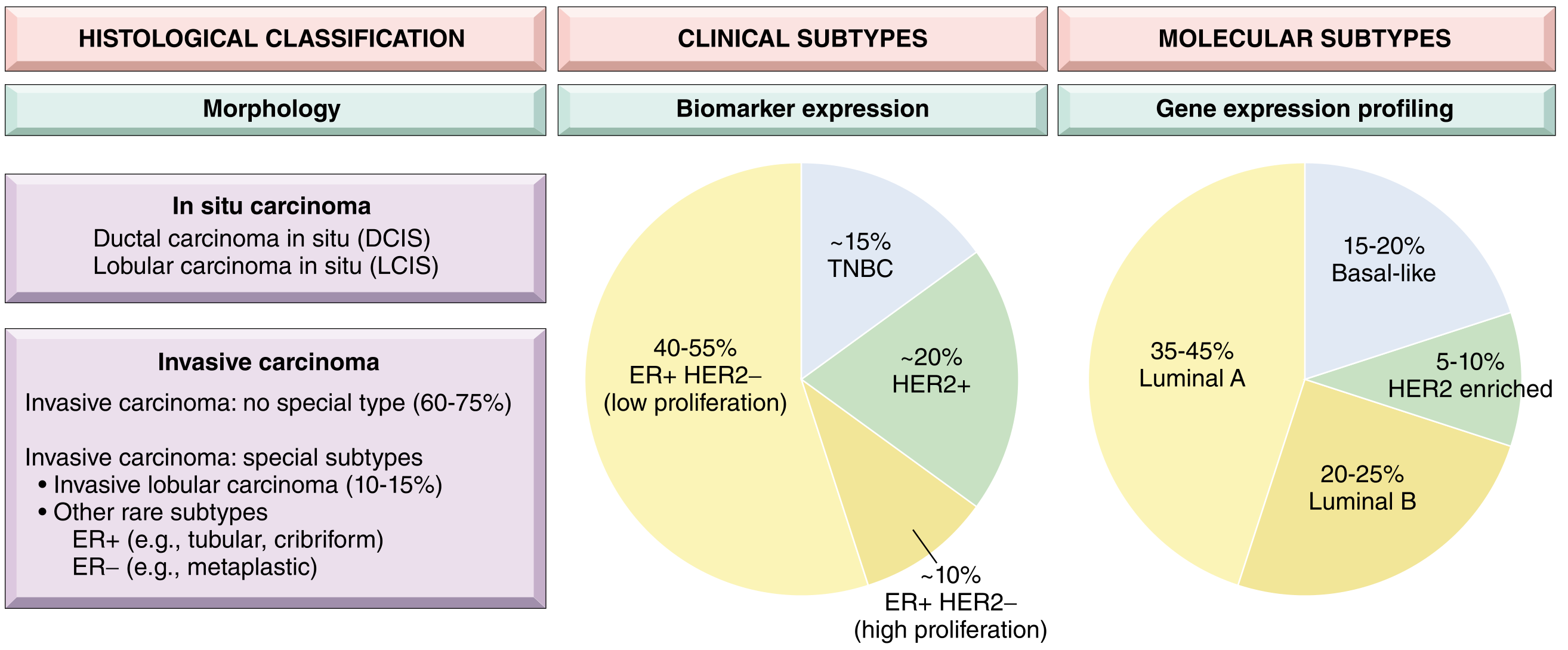
Luminal A (35-45% of breast cancers)
- IHC profile: ER+, PR+ (high), HER2-, Ki67 low (<20%)
- Molecular features: High ER/luminal gene expression; 1q gain, 16q loss
- Behavior: Low grade (typically Grade 1-2), slow proliferation, excellent prognosis
- Treatment: Endocrine therapy alone usually sufficient; chemotherapy often avoidable
- 10-year survival: Approximately 80-90%
Luminal B (20-25% of breast cancers)
- IHC profile: ER+ (lower levels), PR-, HER2- or HER2+, Ki67 high (≥20%)
- Molecular features: Higher genomic instability than Luminal A
- Behavior: Higher grade (typically Grade 2-3), greater proliferation, higher risk of recurrence
- Treatment: Endocrine therapy + chemotherapy (anthracycline/taxane-based)
- Prognosis: Intermediate; worse than Luminal A
HER2-Enriched (5-10% of breast cancers)
- IHC profile: HER2 overexpression/amplification; may be ER+/-
- Molecular features: HER2 amplicon overexpression; often TP53 mutation
- Behavior: High grade, high proliferation, historically aggressive
- Treatment: Anti-HER2 therapy (trastuzumab + pertuzumab) + chemotherapy; outcomes markedly improved with targeted therapy
- Prognosis: Poor without anti-HER2 therapy; much improved with it
Basal-Like / Triple Negative Breast Cancer (TNBC) (15-20%)
- IHC profile: ER-, PR-, HER2- (triple negative); often expresses basal markers CK5/6, EGFR
- Molecular features: High frequency of TP53 mutations; BRCA1 dysfunction common (80% of BRCA1-mutated cancers are basal-like)
- Behavior: High grade (usually Grade 3), very high Ki67, early visceral metastases (lung, brain - not bone/liver as often seen in luminal types)
- Treatment: Chemotherapy (no targeted therapy until recently); pembrolizumab (PD-L1+), olaparib (BRCA mutated), sacituzumab govitecan
- Prognosis: Worst overall survival; paradoxically, higher complete response rates to neoadjuvant chemotherapy; poor prognosis if residual disease after neoadjuvant therapy
- Sabiston Textbook of Surgery, p. 1390
Note: The clinical IHC classification does not exactly overlap with gene expression profiling. Approximately 20% of IHC-defined TNBC are NOT basal-like by molecular profiling, and some HER2+ tumors are luminal by profiling.
IV. Genomic / Multigene Assays
These assays overcome the limitations of individual IHC markers by analyzing panels of genes to generate composite risk scores. They are most useful in early-stage, ER+/HER2-, node-negative or limited node-positive disease where the benefit of adding chemotherapy to endocrine therapy is uncertain.
1. Oncotype DX (21-Gene Recurrence Score) - Most Widely Used
- Technology: RT-PCR on FFPE paraffin-embedded tumor tissue
- Genes: 16 cancer-related genes + 5 reference genes
- Output: Recurrence Score (RS) 1-100
| RS | Risk Category | Interpretation |
|---|---|---|
| <18 | Low | Chemotherapy can be avoided |
| 18-30 | Intermediate | Intermediate benefit from chemo |
| >30 | High | Chemotherapy significantly beneficial |
- Evidence: TAILORx trial validated that women with RS 0-25 (age >50) and RS 0-15 (age <50) derive no benefit from adding chemotherapy to endocrine therapy
- Predicts both recurrence risk AND benefit from chemotherapy in ER+/HER2-/N0 and N1 (1-3 nodes) disease
- Ki67 included in the gene panel; the four-marker IHC4 panel (ER, PR, HER2, Ki67) provides similar information at lower cost - Bailey & Love's Surgery, p. 962; Sabiston Textbook of Surgery, p. 1390
2. MammaPrint (70-Gene Recurrence Assay)
- Technology: Microarray analysis of 70 genes; can use fresh/frozen or FFPE tissue
- Output: Binary readout - low risk or high risk
- Applicable to both ER+ and ER- tumors; Node-negative AND limited node-positive disease
- Evidence: MINDACT trial showed ~46% of clinically high-risk patients were genomically low risk and could safely avoid chemotherapy
- Validated in premenopausal and postmenopausal women - Bailey & Love's Surgery, p. 962
3. PAM50 / Prosigna
- Identifies the four molecular subtypes (Luminal A, Luminal B, HER2-enriched, Basal-like) using 50-gene expression analysis
- Provides a Risk of Recurrence (ROR) score
- Particularly useful for determining late distant recurrence risk (years 5-10) in ER+ patients on endocrine therapy
4. EndoPredict and Breast Cancer Index (BCI)
- Both provide prognostic information for late recurrence risk in ER+/HER2- early breast cancer
- BCI uniquely predicts benefit from extended endocrine therapy (beyond 5 years)
V. Genetic / Germline Markers
BRCA1 and BRCA2
- BRCA1 mutations confer susceptibility to breast AND ovarian cancer; ~45% of hereditary breast cancers carry BRCA1 germline mutations
- BRCA2 mutations also increase breast cancer risk; associated with male breast cancer, ovarian, pancreatic, and prostate cancers
- BRCA1-associated breast cancers: typically triple negative, high grade, basal-like subtype
- BRCA2-associated breast cancers: more commonly ER+ luminal type
- Germline BRCA1/2 mutation carriers: ~10% of women with breast cancer diagnosed at ≤40 years
- Therapeutic implications: PARP inhibitors (olaparib, talazoparib) have demonstrated survival benefit in BRCA-mutated HER2-negative metastatic breast cancer - making this both a prognostic AND predictive marker
- Other hereditary syndromes: TP53 (Li-Fraumeni), PTEN (Cowden), CDH1, PALB2, ATM, CHEK2
VI. Pathological Complete Response (pCR) after Neoadjuvant Therapy
In the neoadjuvant treatment setting, pCR (no residual invasive tumor in breast and lymph nodes - ypT0/Tis ypN0) is a powerful surrogate prognostic marker:
- pCR predicts superior event-free and overall survival
- Most predictive in TNBC and HER2-enriched subtypes
- Luminal A tumors rarely achieve pCR (low chemosensitivity), but have good outcomes regardless
- Residual disease after neoadjuvant therapy in TNBC is an indication for adjuvant capecitabine (CREATE-X trial)
Summary: Integrated Prognostic Assessment
Traditional markers (still clinically mandatory):
| Marker | Good Prognosis | Poor Prognosis |
|---|---|---|
| Lymph nodes | Node-negative (pN0) | ≥4 nodes (pN2-3) |
| Tumor size | T1 (≤2 cm) | T3-T4 (>5 cm) |
| Grade | Grade 1 | Grade 3 |
| ER/PR | Positive | Negative |
| HER2 | Negative | Amplified/Overexpressed* |
| Ki67 | Low (<15%) | High (>30%) |
| LVI | Absent | Present |
| Histological type | Tubular, mucinous, papillary | NST, metaplastic |
| p53 | Normal | Overexpressed (mutant) |
*With anti-HER2 therapy, HER2+ prognosis has greatly improved
Molecular subtype hierarchy (worst to best prognosis without targeted therapy):
TNBC / Basal-like > HER2-enriched > Luminal B > Luminal A
Genomic assay guidance:
- Oncotype DX (RS <18): Safely omit chemotherapy in ER+/HER2-/N0-N1 disease
- MammaPrint (low risk): Safely omit chemotherapy in genomically low-risk patients regardless of clinical risk
Current evidence (2024-2026):
- The 2024 molecular classification review (Roy et al., PET Clinics, PMID 37268505) consolidates the correlation between IHC subtypes and molecular subtypes, and highlights emerging PET-based molecular characterization of breast tumors.
- Kang & Kim, Cancer Research and Treatment 2024 (PMID 38291745) defines HER2-low (IHC 1+ or 2+/ISH-) as a newly actionable prognostic/predictive category, constituting ~55-60% of all breast cancers, now targetable with trastuzumab deruxtecan (T-DXd).
- Dvir et al., Int J Mol Sci 2024 (PMID 39062758) updates immunotherapy biomarkers: PD-L1 CPS ≥10 (by VENTANA SP142 assay) predicts pembrolizumab benefit in early TNBC and metastatic TNBC.
Premalignant lesions of skin short question
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
I have all the material needed. Let me now compose the concise short-answer response.
Premalignant Lesions of Skin
A premalignant (or precancerous) skin lesion is an epithelial proliferation with the potential to transform into an invasive skin cancer. Almost all are confined above the dermo-epidermal junction, and the majority are induced by chronic UV radiation exposure. - Scott-Brown's Otorhinolaryngology, p. 1365
1. Actinic (Solar) Keratosis (AK)
The most common premalignant skin lesion.
Pathology: Intraepithelial neoplasm formed by proliferation of atypical keratinocytes, with the potential to grow into invasive squamous cell carcinoma (SCC).
Epidemiology:
- Appear after age 50; more common in men
- Fitzpatrick skin types I-III (fair skin, tendency to burn) at highest risk
- 40-50% of Australians over 40 years affected; 11-25% in the US
- Prevalent on face, scalp, dorsal hands, neck (>80% of lesions)
Risk factors: Chronic sun exposure, outdoor occupations, sun beds, immunosuppression, albinism, xeroderma pigmentosum, ionizing radiation
Clinical features:
- Usually asymptomatic; noticed due to rough texture
- Dry, erythematous, scaly lesions on sun-exposed skin
- Thin lesions more easily palpable than visible
- Covered with an adherent scale; may be pigmented or telangiectatic
- Thick lesions may have marked hyperkeratosis forming a cutaneous horn
- Surrounding skin shows solar elastosis (thickened, yellow, wrinkled skin)
Features suspicious for SCC transformation: induration, rapid growth, ulceration, bleeding
Histology: Atypical keratinocytes confined to the epidermis; increased mitoses, nuclear polymorphism, hyperchromasia, loss of polarity
Malignant potential: Risk of transformation to SCC is low for individual lesions but cumulatively significant in patients with many AKs
Management:
- Thin/small lesions: moisturizer, keratolytic (salicylic acid); spontaneous resolution in 21%
- Cryotherapy (liquid nitrogen): effective for thicker lesions; painful, may scar
- 5-Fluorouracil (5-FU) cream: once/twice daily for 6 weeks; excellent cosmetic result
- Imiquimod cream: immune response modifier; 3x/week for 4 weeks
- Ingenol mebutate: 2 daily applications for head/neck AKs
- Photodynamic therapy (PDT) with methyl aminolevulinic acid + red light: highly effective, good cosmesis
- Surgery (curettage or excision): when other treatments fail or diagnostic doubt
- Prevention: sunscreen is the only intervention that reduces AK formation; photoprotection counseling is mandatory - Scott-Brown's Otorhinolaryngology, p. 1365-1366
2. Bowen's Disease (BD) - Squamous Cell Carcinoma In Situ
Definition: Intraepidermal carcinoma (SCC in situ) involving the full thickness of the epidermis without invasion of the basement membrane. First described by John Bowen in 1912.
Epidemiology:
- Adults >60 years; slightly more common in women (UK data); men more commonly on scalp and trunk
- Head and neck, lower limbs (in UK, 67% on lower limbs)
- Usually solitary; multiple in ~20% of cases
Etiology:
- Chronic UV radiation (most common)
- Arsenic exposure
- Immunosuppression
- HPV infection (mucosal BD)
- Ionizing radiation, PUVA therapy
Malignant potential: Risk of progression to invasive SCC is ~3-5% - remains stable for many years
Clinical features:
- Long-standing, slowly growing, usually asymptomatic lesion
- Well-defined, sharply demarcated, scaly erythematous plaque on sun-exposed skin
- Surface: scaling, crusting, or hyperkeratotic
- Usually pink/red; may be gray or brownish; rarely pigmented
- Flat plaque may eventually become nodular or verrucous (suggests invasive SCC)

Histology: Full-thickness epidermal dysplasia with:
- Disordered architecture
- Abnormal mitoses, nuclear hyperchromasia and pleomorphism
- Hyperkeratosis
- Dysplastic cells extending along hair follicle epithelium (but NOT invading basement membrane)
Differential: Lichen simplex, eczema, psoriasis, fungal infection, superficial BCC
Management:
- 5-Fluorouracil cream: highly effective for most lesions
- Imiquimod: particularly useful for HPV-associated BD
- Cryotherapy: effective; limited by pain and slow healing in large lesions
- PDT: cure rates ~90%; preferred for large or difficult sites
- Curettage and cautery: simple, effective; allows histology but cannot always exclude invasion
- Surgical excision with 2 mm margin: for clinically suspicious lesions or when conservative treatment fails; Mohs surgery for difficult sites
- Skin biopsy is recommended to confirm diagnosis before treatment - Scott-Brown's p. 1366-1367; Fitzpatrick's Dermatology
3. Keratoacanthoma (KA)
- Rapidly growing crateriform nodule with a central keratin plug, usually on sun-exposed skin
- Considered by many a well-differentiated SCC variant (low-grade SCC)
- Characteristically enlarges rapidly over weeks then may spontaneously involute
- Features suspicion of malignancy: size >2 cm, failure to involute, perineural invasion on histology
- Management: Surgical excision (preferred); allows histological confirmation and excludes invasive SCC - Goldman-Cecil Medicine
4. Dysplastic (Atypical) Melanocytic Nevi
- Melanocytic nevi with atypical clinical and histological features
- Dysplastic nevi exist in 2-8% of the general population
- Development of >5 atypical melanocytic nevi carries a 5-fold increase in melanoma risk
- Development of >100 acquired melanocytic nevi = 10-fold increase in melanoma risk
- Dysplastic nevus syndrome (DNS) / Familial Atypical Multiple Mole Melanoma (FAMMM): autosomal dominant; markedly elevated lifetime risk of melanoma
Features (ABCDE rule applied to nevi): Asymmetry, irregular Border, Color variation, Diameter >6 mm, Evolution/Enlargement
Management: Surveillance with regular dermoscopy; excision of lesions with high-grade atypia or those showing change - Current Surgical Therapy 14e, p. 946
5. Congenital Melanocytic Nevi (CMN)
- Present at birth or appear in infancy
- Giant CMN (>20 cm) carries the highest risk of melanoma transformation (~5-12% lifetime risk)
- Small/medium CMN: very low malignant risk
- Management: prophylactic excision considered for giant CMN; surveillance for smaller lesions
6. Solar (Actinic) Lentigo
- Flat, well-circumscribed, tan-brown macules on chronically sun-exposed skin (face, dorsal hands)
- Also called "liver spots" or "age spots"
- Groups of solar lentigines carry a 4-fold increase in melanoma risk
- Lentigo maligna (Hutchinson's melanotic freckle) is a special form that represents melanoma in situ on chronically sun-damaged skin and can progress to lentigo maligna melanoma
7. Leukoplakia
- White patch or plaque on a mucous membrane (oral cavity, vulva, glans penis) that cannot be scraped off and cannot be classified as any other definable lesion
- Histologically shows a range from hyperkeratosis → mild dysplasia → severe dysplasia → carcinoma in situ
- Malignant transformation rate: ~5% over 10 years for oral leukoplakia
- Erythroplakia (red velvety patch): higher malignant potential than leukoplakia; ~40-50% contain carcinoma at time of biopsy
- Speckled leukoplakia (mixed red and white): intermediate risk
- Management: biopsy to establish grade of dysplasia; excision or ablation for high-grade dysplasia; cessation of tobacco/alcohol
8. Chronic Scars, Ulcers, and Sinuses (Marjolin's Ulcer)
- Malignant transformation can occur in chronic non-healing wounds, burn scars, osteomyelitis sinuses, and post-irradiation scars
- The resulting tumor is usually a well-differentiated but aggressive SCC - Marjolin's ulcer
- Long latent period (typically 20-40 years after original injury)
- Diagnosis often delayed due to being hidden in existing wound
- More aggressive than de novo SCC: higher rate of lymph node metastasis despite well-differentiated histology
- Management: wide excision; regional node assessment
9. Radiation Dermatitis (Radiodermatitis)
- Chronic radiation damage following therapeutic or occupational ionizing radiation exposure
- Presents as atrophic, telangiectatic, dyspigmented skin with loss of adnexal structures
- Progresses to SCC after a latency of years to decades
- Risk is also elevated for BCC in irradiated fields
Summary Table
| Lesion | Derived Malignancy | Risk of Transformation | Key Feature |
|---|---|---|---|
| Actinic keratosis | SCC | Low per lesion; cumulative in many lesions | Rough scaly patch on sun-exposed skin |
| Bowen's disease | SCC (invasive) | 3-5% | Full-thickness epidermal carcinoma in situ |
| Keratoacanthoma | SCC (low-grade) | Moderate | Crateriform nodule with keratin plug; rapid growth |
| Dysplastic nevus | Melanoma | 5x risk if >5 lesions | Atypical melanocytic lesion; irregular pigment |
| Congenital giant nevus | Melanoma | 5-12% lifetime | Present at birth; >20 cm |
| Solar lentigo (lentigo maligna) | Melanoma | ~5-10% (lentigo maligna) | Irregular tan-brown macule; sun-damaged skin |
| Leukoplakia | SCC (oral) | ~5% over 10 years | White plaque on mucous membrane |
| Erythroplakia | SCC (oral) | ~40-50% already carcinoma | Red velvety mucosal plaque |
| Marjolin's ulcer | SCC | High after decades | Chronic scar/ulcer transformation |
| Radiodermatitis | SCC/BCC | Significant | Post-irradiation atrophic skin |
Key points:
- Most premalignant skin lesions are induced by ultraviolet light
- Photoprotection (sunscreen, avoidance of UV) is the only intervention proven to reduce AK formation
- Any premalignant lesion showing induration, ulceration, rapid growth, or bleeding warrants urgent biopsy to exclude invasive SCC
- Patients with precursor lesions must be educated to recognize early signs of skin cancer and seek early medical attention - Scott-Brown's Otorhinolaryngology, p. 1367
This is a shared conversation. Sign in to Orris to start your own chat.