Mri brachial plexus radiology 1. Normal anatomy 2. relevant pathology and it's imaging findings 3.normal mri appearance included images
Reading File
Finding Sources
Searching the Web
MRI brachial plexus normal anatomy imaging findings radiology
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Finding Sources
Loading Image
Finding Sources
Searching the Web
MRI brachial plexus sequences protocol STIR T2 normal appearance nerves
Loading Image
I now have everything needed. Let me compose a comprehensive, image-rich review of MRI brachial plexus.
MRI of the Brachial Plexus: Normal Anatomy, Pathology, and Imaging Findings
1. Normal Anatomy
Overview
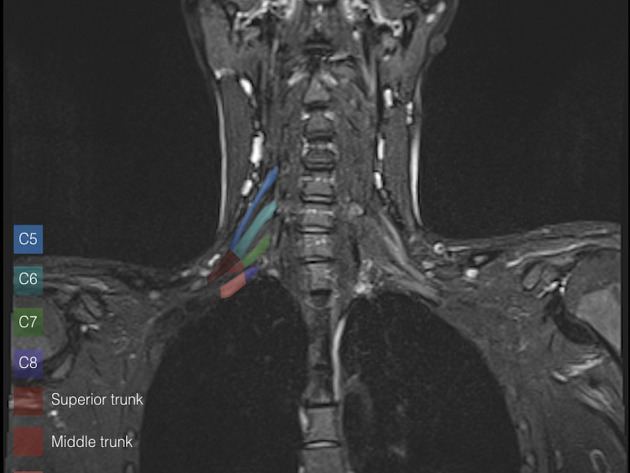
The brachial plexus is a somatic nerve network formed by the anterior rami of C5, C6, C7, C8, and T1. It originates in the posterior triangle of the neck, traverses the scalene triangle (between anterior and middle scalene muscles), passes over the first rib, and enters the axilla. All major nerves innervating the upper limb arise from it.

The "RTDC" Organization (Roots - Trunks - Divisions - Cords)
| Level | Components | Key Relations |
|---|---|---|
| Roots | Anterior rami C5-T1 | Between anterior & middle scalene muscles; posterior to subclavian artery |
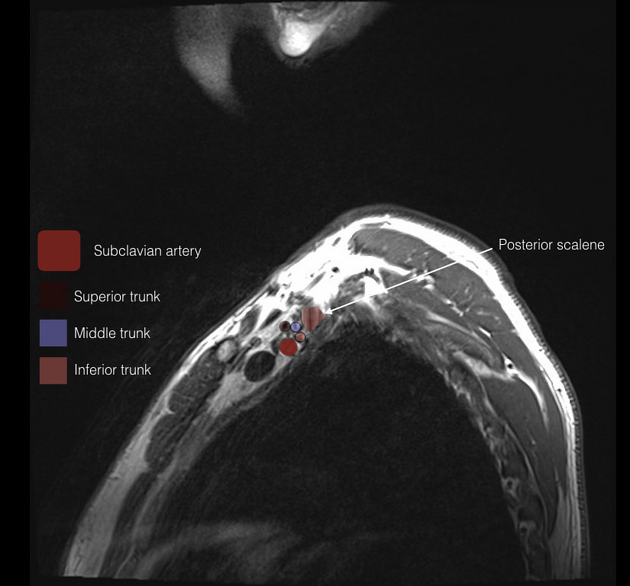
| Trunks | Superior (C5+C6), Middle (C7), Inferior (C8+T1) | Cross over rib I; inferior trunk lies on rib I posterior to subclavian artery |
| Divisions | Each trunk splits into anterior + posterior | At the level of the clavicle; no peripheral nerves arise directly from divisions |
| Cords | Lateral, Posterior, Medial | Named by relation to axillary artery; surround axillary artery in axilla |
Terminal branches arise at the lateral border of the pectoralis minor: ulnar, median, musculocutaneous, radial, and axillary nerves.
Key Anatomic Spaces
- Scalene triangle (interscalene): between anterior scalene, middle scalene, and first rib - contains roots and trunks
- Costoclavicular space: between clavicle and first rib - trunks/divisions pass here
- Retropectoralis minor (subcoracoid) space: cords and terminal branches here
2. Normal MRI Appearance
Imaging Protocol
MRI brachial plexus requires a dedicated protocol. The standard sequences at most centers include:
| Sequence | Plane | Purpose |
|---|---|---|
| T1W | Coronal oblique | Anatomical detail, fat planes, nerve identification |
| STIR / T2FS | Coronal oblique | Neural edema detection (nerves bright), fat suppression |
| 3D T2 SPACE/CUBE/VISTA | Multiplanar | High-resolution nerve anatomy, MIP reconstructions |
| T1 +Gd FS | Axial + coronal | Enhancement pattern (neoplasm vs. inflammation) |
| Axial T1 / T2 | Axial | Root-level assessment, foraminal evaluation |
| Myelogram sequence (CISS/FIESTA) | Coronal | Intradural nerve roots, avulsion/meningocele |
Field strength: 3T preferred; 1.5T acceptable. The patient is positioned supine with arms by the side.
Normal MRI Signal Characteristics
On a properly performed brachial plexus MRI:
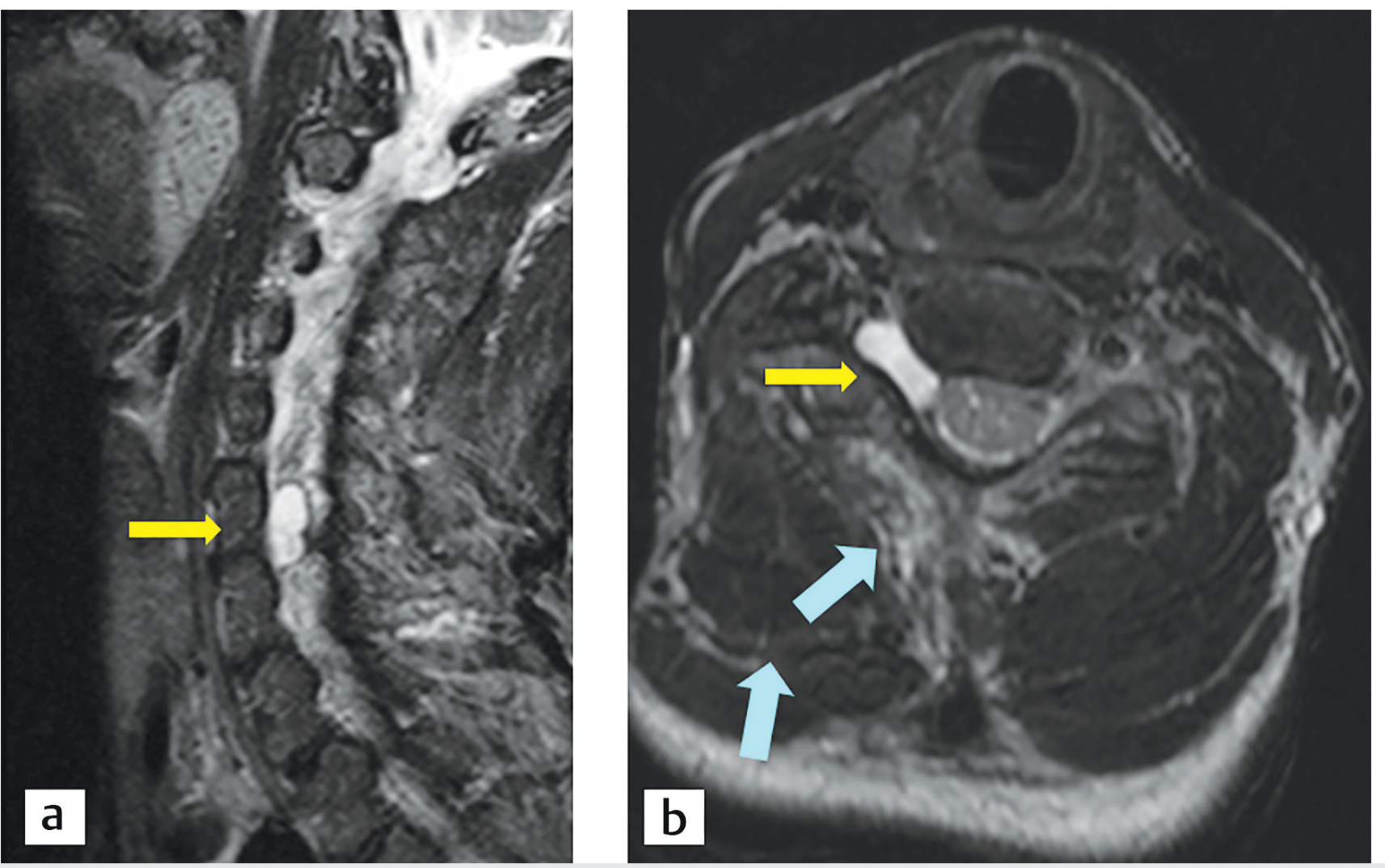
- T1W: Nerves appear as isointense to slightly hypointense cord-like structures surrounded by hyperintense fat. The nerve fascicles are uniform in caliber.
- T2W / STIR: Normal nerves show mild intermediate-to-slightly high signal - somewhat brighter than muscle but less bright than fluid. A faint internal fascicular pattern may be visible on high-resolution sequences.
- Post-contrast T1 FS: Normal nerve roots show minimal or no enhancement. Moderate enhancement of the nerve root sleeves at the level of the dorsal root ganglia is a normal finding.
- Caliber: Smooth and uniform. Normal root diameter at 3T is approximately 2-4 mm.
MRI Views: Coronal Orientation with C5-C8, T1

Key Landmarks on Normal MRI
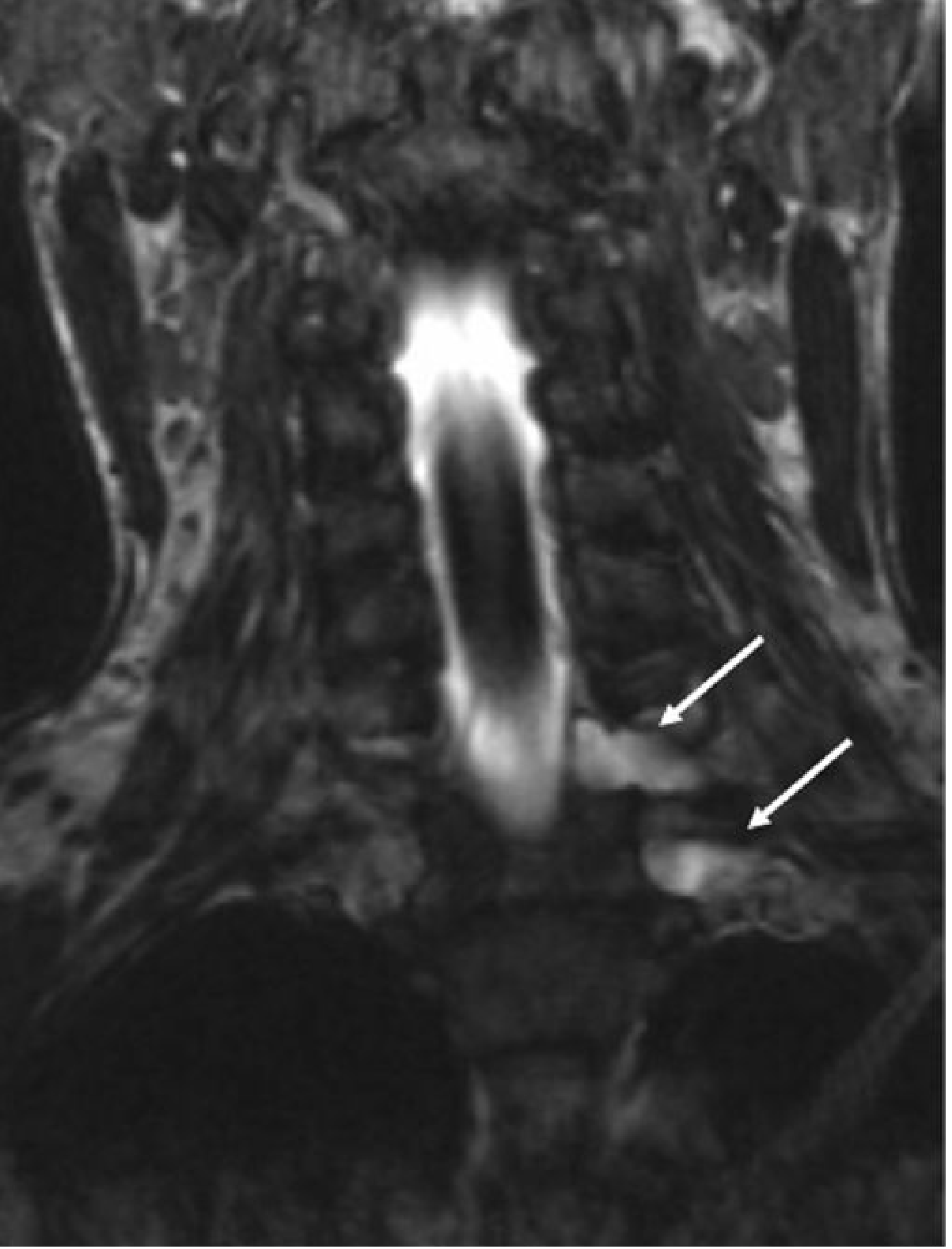
- Coronal images: Roots exit foramina as linear structures, trunks run obliquely through the posterior triangle. The three trunks group tightly together before passing over rib I.
- Axial images: At the C5-C6 level, roots are seen between scalene muscles. At the supraclavicular level, three distinct trunks with uniform signal are grouped around the subclavian artery.
- Normal fat planes: Preserved fat planes between the nerves and surrounding structures are a key sign of normality.
3. Relevant Pathology and Imaging Findings
A. Traumatic Brachial Plexus Injury
Trauma accounts for the majority of brachial plexus pathology, most commonly from high-velocity injuries (motorcycle accidents, birth injury). 75% of clinical cases involve root avulsion; 25% are confined to the distal (infraclavicular) plexus.
Preganglionic (Root Avulsion) Injury
- Mechanism: Traction force pulling the head away from the shoulder tears the rootlets at the cord-root junction (intradural).
- MRI signs:
- Traumatic pseudomeningocele: CSF-filled sac (T2 hyperintense, T1 hypointense) at the site of dural tear - pathognomonic for root avulsion
- Absent nerve root sleeves on myelographic sequences
- Cord edema / myelomalacia: Diffuse T2 hyperintensity of the cervical cord (do not mistake for direct cord injury)
- Denervation edema of paraspinal muscles (multifidus, semispinalis) - T2 hyperintense, swollen acutely; fatty replaced chronically

Postganglionic (Distal) Injury
- Occurs distal to the dorsal root ganglion
- MRI signs:
- No pseudomeningocele
- Nerve root sleeves are intact on myelographic sequences
- Nerve discontinuity, swelling, or T2 hyperintensity in the supraclavicular or infraclavicular region
- Neuroma-in-continuity: fusiform nerve thickening, heterogeneous T2 signal
B. Thoracic Outlet Syndrome (TOS)
- Neurogenic TOS is the most common form, caused by compression of the inferior trunk (C8-T1) by a cervical rib, fibrous band, or anomalous scalene muscle.
- MRI findings:
- Cervical rib or elongated C7 transverse process
- Compression/displacement of the inferior trunk
- In chronic cases: nerve thickening with T2 hyperintensity
- Dynamic MRI (arms raised) can demonstrate positional vascular or neural compression
- STIR may show reactive edema in compressed segments

C. Neoplastic (Malignant) Plexopathy
The most common tumors involving the brachial plexus are lung carcinoma (especially Pancoast/superior sulcus tumors) and breast carcinoma, followed by lymphoma, sarcoma, and melanoma.
- MRI findings:
- Mass lesion adjacent to or encasing plexus elements - the key distinguishing feature from radiation plexopathy
- T1: isointense to muscle; T2: heterogeneously hyperintense
- Post-contrast: heterogeneous enhancement
- Focal "mass-like" enhancement of plexus
- Destruction of adjacent bone (vertebral body, ribs, clavicle)
- Obliteration of normal fat planes around nerves
- MRI sensitivity for tumor infiltration: 96%, specificity 95%, positive predictive value 95% (Bradley & Daroff's Neurology in Clinical Practice)
- Pancoast tumor: apical lung mass with inferior trunk involvement; Horner syndrome from stellate ganglion invasion
D. Radiation-Induced Plexopathy
Most commonly follows radiotherapy for breast cancer, lung cancer, or lymphoma involving axillary, apical, or base-of-neck fields.
- MRI findings:
- Diffuse, uniform swelling and thickening of plexus elements - no focal mass
- T2/STIR: hyperintense signal of the BP within the radiation field
- Low signal on T1 and T2 FS suggests fibrosis with tethering/downward traction
- Mild, diffuse enhancement (vs. focal/asymmetric enhancement in tumor)
- No bony destruction
- Surrounding soft-tissue radiation change (skin thickening, subcutaneous edema/fibrosis)
- Key differentiator: Radiation plexopathy = no focal mass; metastatic plexopathy = focal enhancing mass
(Grainger & Allison's Diagnostic Radiology; Bradley & Daroff's Neurology in Clinical Practice)
E. Neurogenic Tumors (Schwannoma, Neurofibroma)
- Schwannoma: Arises eccentrically from a single fascicle; the nerve can be displaced but remains largely intact.
- T1: isointense; T2: markedly hyperintense ("target sign" - central hypointense with peripheral hyperintense rim)
- Well-defined, smooth margins; homogeneous or slightly heterogeneous enhancement
- Neurofibroma: Diffusely involves the nerve fascicles; fusiform expansion.
- Similar signal but nerve cannot be separated from mass
- "Target sign" also possible
- Multiple neurofibromas = neurofibromatosis type 1 (NF1)
- Malignant peripheral nerve sheath tumor (MPNST): Large, irregular, infiltrative; rapid growth; heterogeneous signal with necrosis; aggressive enhancement; associated with NF1 in ~50% of cases
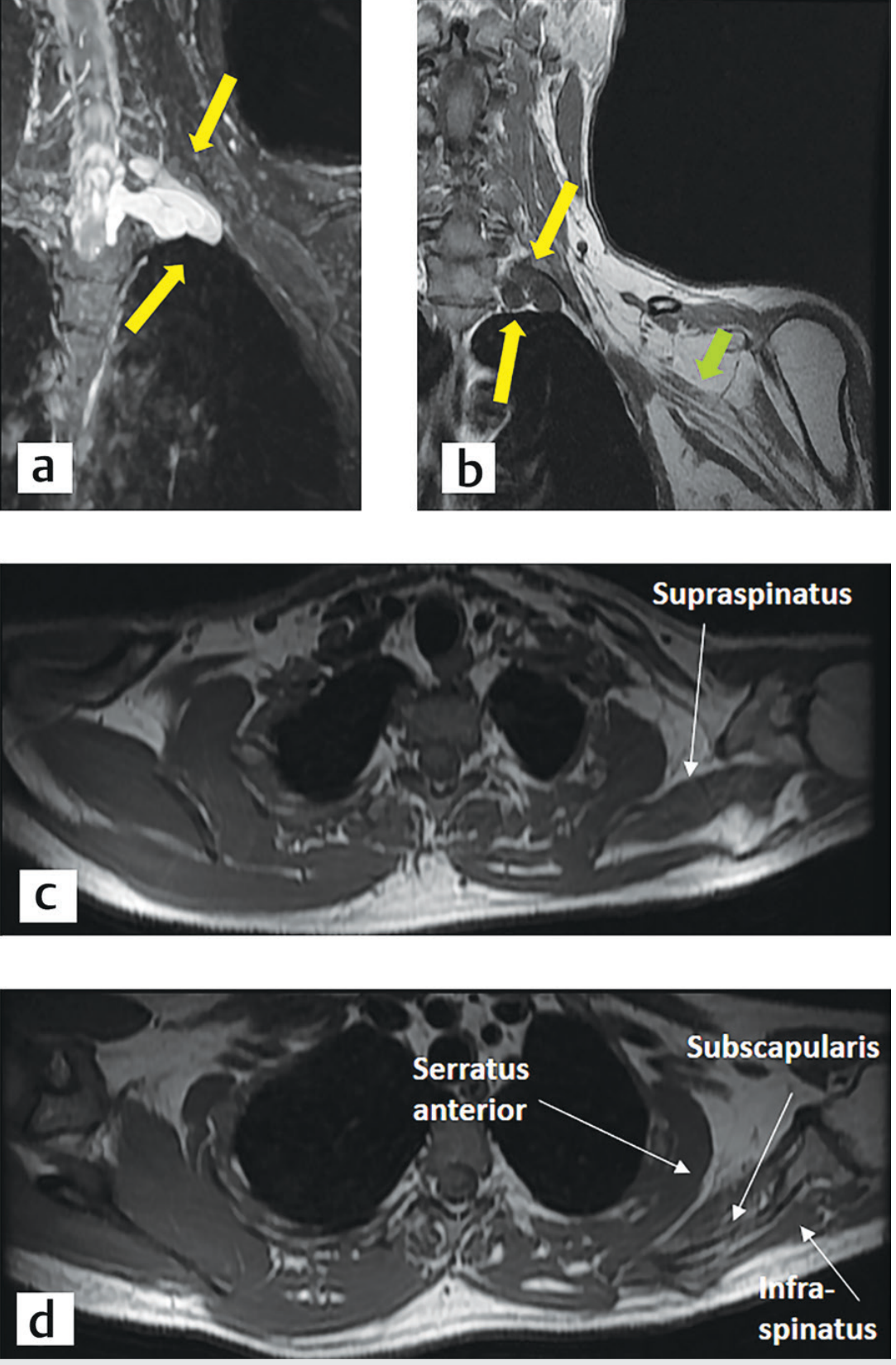
F. Inflammatory / Immune Brachial Plexopathy (Parsonage-Turner Syndrome / Neuralgic Amyotrophy)
- Acute, often post-viral or post-vaccination immune-mediated plexitis
- MRI findings (often normal acutely):
- T2/STIR: patchy hyperintensity of plexus elements and early denervation of innervated muscles
- Nerve enlargement and increased signal on STIR
- Denervation edema of shoulder girdle muscles (supraspinatus, infraspinatus, deltoid, serratus anterior)
- No mass lesion
- MRI neurography (3D STIR with MIP) best demonstrates the patchy distribution
G. Diabetic and Other Inflammatory Plexopathies
- CIDP / multifocal motor neuropathy: Diffuse thickening of roots, trunks, and peripheral nerves with increased T2 signal and marked post-contrast enhancement
- Sarcoidosis: Can involve brachial plexus - diffuse nerve thickening with T2 hyperintensity; may show enhancement
Summary Table: MRI Differential Diagnosis
| Condition | T2/STIR Signal | Enhancement | Mass | Key Feature |
|---|---|---|---|---|
| Traumatic avulsion | Pseudomeningocele (bright) | None | No | Meningocele, cord edema |
| Neurogenic TOS | Mild/focal hyperintense | None-mild | No | Cervical rib, nerve compression |
| Malignant infiltration | Heterogeneous high | Focal, "mass-like" | YES | Adjacent mass, bone destruction |
| Radiation plexopathy | Diffuse high | Diffuse, mild | No | Fibrosis, no mass; post-RT history |
| Schwannoma | High, "target sign" | Strong, homogeneous | YES | Eccentric to nerve |
| Neurofibroma | High, "target sign" | Moderate | YES | Fusiform, inseparable from nerve |
| Parsonage-Turner | Patchy high | Variable | No | Denervation edema, clinical acute pain |
| CIDP | Diffuse high | Diffuse, marked | No | Bilateral, symmetrical thickening |
References
- Gray's Anatomy for Students, Gray's Anatomy for Students, pp. 858-860
- Grainger & Allison's Diagnostic Radiology, Brachial Plexus Injury section, pp. 1338-1340
- Imaging Anatomy: Bones, Joints, Vessels and Nerves, Vol. 3, pp. 189-291
- Bradley & Daroff's Neurology in Clinical Practice, Brachial Plexopathy and Cancer chapters
- Neuroanatomy through Clinical Cases, 3rd ed.
- Applied Radiology: "MRI of the brachial plexus: A practical review" (appliedradiology.com)
- Radiopaedia: Brachial plexus MRI
This is a shared conversation. Sign in to Orris to start your own chat.