Hey i am a first year student in kusms in nepal and i have a pbl session tomorrrow. I have some learnining objective and my pbl tutuor me to learn about the topics from a medical book i will ask you qustion and the answer you give everything must be from a medical book. also give me the source . tell me tell me about why zinc is given to baby in diarrhoea? also tell me about layer of abdomen and blood cs, its important and about blood culture sensitivity with a diagram remeber every answer must be with respect to a book
PBL Study Notes - KUSMS First Year
TOPIC 1: Why Is Zinc Given to Babies in Diarrhoea?
Source: Park's Textbook of Preventive and Social Medicine (p. 721 & Diarrhoeal Disease Control chapter)
"Zinc deficiency is common in children from developing countries due to lack of intake of animal food, high dietary phytate content, inadequate food intake and increased faecal losses during diarrhoea."
- Park's Textbook of Preventive and Social Medicine, p. 721
"Zinc supplementation in combination with oral rehydration therapy has been shown to significantly reduce the duration and severity of acute and persistent diarrhoea and to increase survival in a number of randomized control trials."
- Park's Textbook of Preventive and Social Medicine, p. 721
"Adequate zinc intake is essential for maintaining the integrity of the immune system."
- Park's Textbook of Preventive and Social Medicine, p. 721
"When a zinc supplement is given during an episode of acute diarrhoea, it reduces the episode's duration and severity. In addition, zinc supplements given for 10 to 14 days lower the incidence of diarrhoea in the following 2 to 3 months."
- Park's Textbook of Preventive and Social Medicine, Diarrhoeal Disease Control chapter
| Age | Dose | Duration |
|---|---|---|
| Infants under 6 months | 10 mg/day | 10-14 days |
| Children older than 6 months | 20 mg/day | 10-14 days |
"WHO and UNICEF therefore recommend daily 10 mg of zinc for infants under 6 months of age, and 20 mg for children older than 6 months for 10-14 days."
- Park's Textbook of Preventive and Social Medicine, p. 885
TOPIC 2: Layers of the Abdomen (Anterior Abdominal Wall)
Source: Mulholland and Greenfield's Surgery - Scientific Principles and Practice, 7e (p. 3632-3639) & THIEME Atlas of General Anatomy
Layers (Superficial to Deep):
| # | Layer | Details |
|---|---|---|
| 1 | Skin | Segmentally innervated (dermatome pattern, 7th-12th intercostal nerves) |
| 2 | Superficial fascia (Camper's fascia) | Contains fat (panniculus adiposus); continuous with perineal fascia; contains superficial epigastric and superficial circumflex iliac vessels |
| 3 | Deep fascia (Scarpa's fascia) | Compressed fibrous layer; forms fundiform ligament of penis |
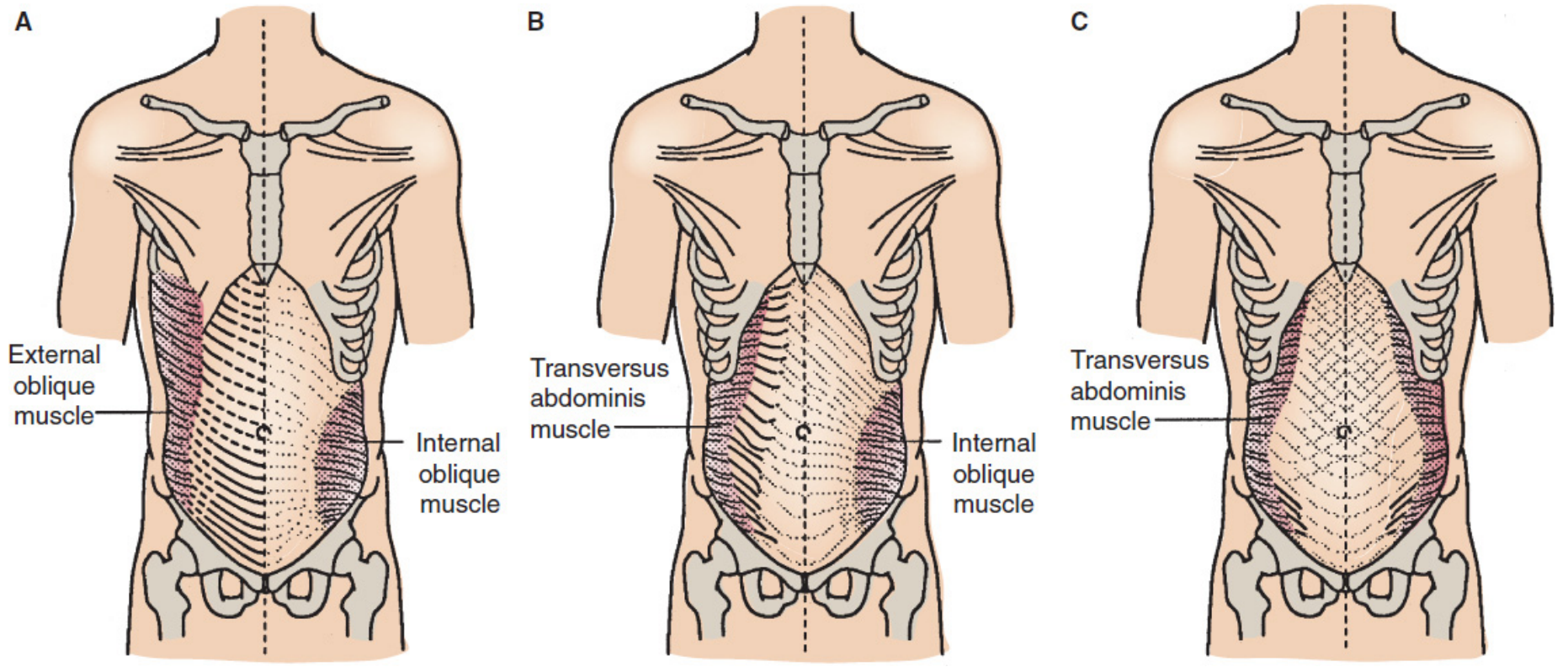
| 4 | External abdominal oblique muscle & aponeurosis | Most superficial of three flat muscles; fibres run obliquely downward and medially; aponeurosis forms anterior rectus sheath and inguinal ligament |
| 5 | Internal abdominal oblique muscle & aponeurosis | Fibres run perpendicular to external oblique; aponeurosis splits to enclose rectus abdominis |
| 6 | Transversus abdominis muscle & aponeurosis | Deepest flat muscle; fibres run transversely; forms arcuate line (line of Douglas) |
| 7 | Transversalis fascia | Thin fibrous layer lining the inner surface of transversus abdominis |
| 8 | Extraperitoneal (preperitoneal) fat | Loose fatty connective tissue between transversalis fascia and peritoneum |
| 9 | Peritoneum (parietal) | Innermost layer |
"The three muscles of the lateral aspect of the anterior abdominal wall are composed of a variable amount of muscle with a large aponeurosis. The aponeurosis is the tendon of insertion for the lateral muscles, and it also forms the sheath of the rectus abdominis. The midline decussation of the three aponeuroses forms the linea alba."
- Mulholland and Greenfield's Surgery, p. 3634
Central Muscle - Rectus Abdominis:
"The rectus abdominis forms the central and anchoring muscle mass of the anterior abdomen. The rectus muscle arises from the fifth to the seventh costal cartilages and inserts on the pubic symphysis and pubic crest. Each rectus muscle is segmented by tendinous intersections at the levels of the xiphoid process and the umbilicus and at a point midway between these two. The principal blood supply reaches the muscle from the superior and inferior epigastric arteries."
- Mulholland and Greenfield's Surgery, p. 3639
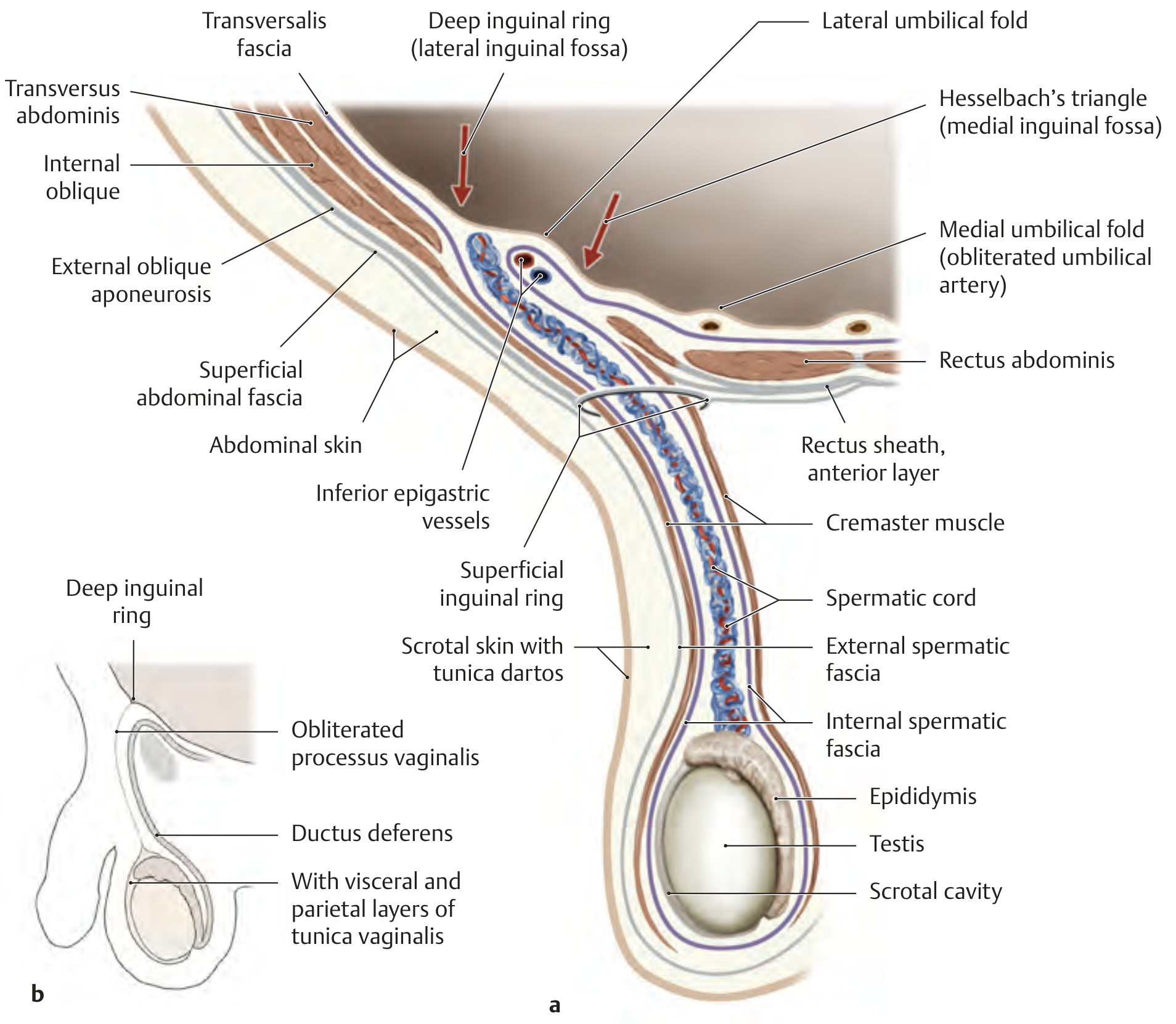
Diagram of Abdominal Wall Layers:
Relationship to Spermatic Cord (Clinically Important):
| Abdominal Wall Layer | Spermatic Cord/Testes Covering |
|---|---|
| Abdominal skin + membranous superficial fascia | Scrotal skin with tunica dartos |
| External oblique fascia | External spermatic fascia |
| Internal oblique muscle and fascia | Cremaster muscle with cremasteric fascia |
| Transversalis fascia | Internal spermatic fascia |
| Peritoneum | Tunica vaginalis (parietal and visceral layers) |
TOPIC 3: Blood Culture and Sensitivity (Blood C/S)
Source: Tietz Textbook of Laboratory Medicine, 7th Edition & Roberts and Hedges' Clinical Procedures in Emergency Medicine
What is Blood Culture and Sensitivity?
Types of Bloodstream Infections (BSI):
"BSIs occur for a variety of reasons. In general, they can be categorised as either intravascular or extravascular. Intravascular infections include infective endocarditis and intravenous catheter-related infection. Extravascular BSI results when organisms multiply at a body site, are drained by the lymphatic system, and gain access to the bloodstream. Common extravascular sites that lead to BSI are abscesses, wounds, surgical wounds, the respiratory tract, and the genitourinary tract."
- Tietz Textbook of Laboratory Medicine, 7th Edition
Specimen Collection - Critical Points:
"A critical aspect of blood culture draws is the disinfection of the skin (for peripheral blood draws). The CDC recommends disinfecting the site with 70% alcohol and then using povidone-iodine. Alternative methods include the use of chlorhexidine and chlorine peroxide."
- Tietz Textbook of Laboratory Medicine, 7th Edition
"The most critical factor influencing the sensitivity of blood cultures for the detection of BSI is the volume of blood drawn."
- Tietz Textbook of Laboratory Medicine, 7th Edition
| Patient | Recommended Volume | Notes |
|---|---|---|
| Adults | 40-60 mL total (20 mL per draw) | Each bottle (aerobic + anaerobic) gets 10 mL each |
| Children | 1 mL per 2.5 kg body weight (max 4-5% of total blood volume) | Bacteraemia levels are 10x higher in neonates than adults |
"In adults, a number of studies have assessed the blood volume required to maximize sensitivity and found that the ideal total volume for blood culture is 40 to 60 mL. Each draw should be 20 mL, with each bottle (aerobic and anaerobic) inoculated with 10 mL."
- Tietz Textbook of Laboratory Medicine, 7th Edition
"Most institutions encourage the order of two blood culture sets that include both aerobic and anaerobic bottles. These cultures should be collected from two distinct sites (i.e., a peripheral venous draw from the right and left arm or a central line and peripheral venous draw)."
- Tietz Textbook of Laboratory Medicine, 7th Edition
"These paired cultures help the provider differentiate between contamination and true infection. True bacteraemia will result in multiple positive cultures, whereas single positive cultures with skin or respiratory microbiota suggest contamination."
- Tietz Textbook of Laboratory Medicine, 7th Edition
- In typhoid fever: only 40-60% sensitive (Harrison's Principles of Internal Medicine, 22e)
- With proper technique and adequate volume: up to 80% per set, nearly 99% with two sets of 20 mL each
"An individual set is typically not more than 80% sensitive... sensitivity is typically at approximately 99% with two sets consisting of 20 mL of blood per set."
- Roberts and Hedges' Clinical Procedures in Emergency Medicine
Summary Diagram: Blood Culture Process
PATIENT (suspected BSI/sepsis)
↓
SKIN DISINFECTION
(70% alcohol → povidone-iodine OR chlorhexidine)
↓
BLOOD DRAW (2 separate sites)
SET 1 (Left arm) SET 2 (Right arm)
↓ ↓ ↓ ↓
Aerobic Anaerobic Aerobic Anaerobic
bottle bottle bottle bottle
(10 mL) (10 mL) (10 mL) (10 mL)
↓
INCUBATION (5 days, continuously monitored)
↓
ORGANISM IDENTIFIED
↓
ANTIBIOTIC SENSITIVITY TESTING
(MIC determined → report Sensitive / Intermediate / Resistant)
↓
TARGETED ANTIBIOTIC THERAPY
"Levels of bacteremia are typically 10-fold higher in neonates than in adults. The sicker the child, the greater the likelihood of a high level of bacteremia."
- Roberts and Hedges' Clinical Procedures in Emergency Medicine
Quick Summary Table for PBL Revision
| Topic | Key Point | Source |
|---|---|---|
| Zinc in diarrhoea | Reduces duration + severity; protective for 2-3 months post-episode | Park's PSM |
| Zinc dose (<6 months) | 10 mg/day for 10-14 days with ORS | Park's PSM / WHO-UNICEF |
| Zinc dose (>6 months) | 20 mg/day for 10-14 days with ORS | Park's PSM / WHO-UNICEF |
| Abdominal layers | Skin → Camper → Scarpa → EO → IO → TA → Transversalis fascia → Extraperitoneal fat → Peritoneum | Mulholland's Surgery 7e |
| Linea alba | Formed by midline decussation of all 3 aponeuroses | Mulholland's Surgery 7e |
| Blood C/S key factor | Volume of blood drawn | Tietz Lab Medicine 7e |
| Adult volume | 40-60 mL total, 2 sets from 2 sites | Tietz Lab Medicine 7e |
| Two sets reason | Distinguish true bacteraemia from contamination | Tietz Lab Medicine 7e |
tell me about the toxic dose of pcm in a normal and alcholic person and tell me the mechanism of pcm in flowchart and why n-acetyl is given here also define technical terms used
Paracetamol (PCM) Toxicity - Complete PBL Notes
PART 1: Therapeutic vs Toxic vs Lethal Doses
Source: The Essentials of Forensic Medicine and Toxicology, 36th Edition (2026) - Table 31.1 & Sleisenger and Fordtran's GI and Liver Disease
| Category | Adults | Children |
|---|---|---|
| Therapeutic dose | 500-1000 mg per dose (max 4 g/day) | 10-15 mg/kg/dose (max 60 mg/kg/day) |
| Toxic dose | ≥150 mg/kg (single ingestion) | 150-200 mg/kg |
| Lethal dose | >350 mg/kg | 250-350 mg/kg |
"When a large dose (>150 mg/kg or >10g in an adult) is taken, it causes serious toxicity. Fatality is common with doses >250 mg/kg."
- P.C. Dikshit Textbook of Forensic Medicine and Toxicology, p. 578
"Overdoses of 20 g or more are potentially lethal."
- P.C. Dikshit Textbook of Forensic Medicine and Toxicology
PART 2: Toxic Dose in an ALCOHOLIC Person - Why is it LOWER?
Source: Sleisenger and Fordtran's Gastrointestinal and Liver Disease & Goldman-Cecil Medicine
"Among heavy drinkers, daily acetaminophen doses of 2 to 6 g have been associated with fatal hepatotoxicity."
- Sleisenger and Fordtran's GI and Liver Disease, p. 1670
"In chronic alcoholics, even 5-6 g/day taken for a few days can cause hepatotoxicity."
- P.C. Dikshit Textbook of Forensic Medicine and Toxicology
- CYP2E1 induction: Alcohol induces (upregulates) the CYP2E1 enzyme. This pushes MORE paracetamol down the toxic pathway, producing MORE NAPQI than normal.
- Glutathione depletion: Chronic alcohol use depletes hepatic glutathione stores, so even normal NAPQI production cannot be neutralised.
"Excessive ethanol intake can induce CYP2E1, resulting in a greater fraction of the dose being converted to NAPQI. Patient-specific factors that can significantly reduce the dose threshold for acetaminophen toxicity include poor nutrition and fasting (depleting glucuronidation substrates) as well as excessive ethanol intake."
- Goldman-Cecil Medicine, International Edition
Risk Factors That Lower the Toxic Threshold (Table from Sleisenger & Fordtran)
| Risk Factor | Effect |
|---|---|
| Chronic alcohol ingestion | Toxic dose threshold lowered; worsens prognosis; nephrotoxicity common |
| Fasting / malnutrition | Toxic dose threshold lowered ("therapeutic misadventure") |
| Concomitant drugs (isoniazid, phenytoin, zidovudine) | Toxic threshold lowered |
| Cirrhosis | Recommendation: do NOT exceed 2 g in 24 hours |
| Late presentation / delayed treatment (>16 hr) | Predicts worse outcome |
PART 3: Mechanism of PCM Toxicity - FLOWCHART
Source: The Essentials of Forensic Medicine and Toxicology, 36th Ed. (Fig. 31.1) & Goldman-Cecil Medicine & Rosen's Emergency Medicine
PARACETAMOL (PCM) ingested
|
├──────────────────────────────────────┐
▼ ▼
~90% SAFE PATHWAY ~10% TOXIC PATHWAY
| |
Conjugation with CYP2E1 (P450 enzyme)
GLUCURONIC ACID oxidizes PCM
and SULFATE |
| ▼
NON-TOXIC metabolites NAPQI formed
excreted in urine (N-Acetyl-p-Benzoquinone Imine)
|
┌──────────┴───────────┐
▼ ▼
NORMAL DOSE OVERDOSE
(Glutathione (Glutathione
adequate) EXHAUSTED)
| |
▼ ▼
NAPQI neutralized NAPQI accumulates
by glutathione freely in liver cells
| |
▼ ▼
CYSTEINE + COVALENT BINDING
MERCAPTURIC ACID to liver cell proteins
(non-toxic, excreted) (especially mitochondria)
|
▼
OXIDATIVE STRESS
↓
CENTRILOBULAR HEPATIC NECROSIS
↓
RENAL TUBULAR NECROSIS
↓
ACUTE LIVER FAILURE → DEATH
"N-acetyl-benzoquinone-imine is a highly reactive arylating minor metabolite of paracetamol, which is detoxified by conjugation with glutathione. When a very large dose is taken, hepatic glutathione is depleted and this metabolite binds covalently to proteins in liver cells and renal tubules causing necrosis. Toxicity thus shows a threshold phenomenon, manifesting only when glutathione is depleted to a critical point."
- P.C. Dikshit Textbook of Forensic Medicine and Toxicology, p. 578
"The binding of acetaminophen to hepatocyte macromolecules leads to hepatocyte necrosis... Mitochondrial enzymes are a particular target of NAPQI."
- Harrison's Principles of Internal Medicine, 22E & Sleisenger and Fordtran's
PART 4: Clinical Stages of PCM Poisoning
Source: The Essentials of Forensic Medicine and Toxicology, 36th Ed. - Table 31.2
| Stage | Timeframe | Clinical Features |
|---|---|---|
| Stage I | 0-24 hours | Nausea, vomiting, anorexia, malaise, diaphoresis (sweating); LFTs usually normal |
| Stage II | 24-72 hours | Right upper quadrant pain; rising AST/ALT and bilirubin; prolonged PT; possible renal involvement |
| Stage III | 72-96 hours | Peak hepatotoxicity: jaundice, coagulopathy, hypoglycaemia, hepatic encephalopathy, renal failure, metabolic acidosis, multi-organ failure |
| Stage IV | 4-14 days | Recovery if survived - gradual normalisation of liver function (liver can regenerate) |
PART 5: Why is N-Acetylcysteine (NAC) Given?
Source: P.C. Dikshit Textbook of Forensic Medicine and Toxicology & The Essentials of Forensic Medicine, 36th Ed.
"N-acetylcysteine... replenishes the glutathione stores of the liver and prevents binding of the toxic metabolite to other cellular constituents."
- P.C. Dikshit Textbook of Forensic Medicine, p. 578
"Acetaminophen toxicity is due to the depletion of hepatic glutathione, resulting in the accumulation of toxic metabolic intermediates."
- Morgan and Mikhail's Clinical Anesthesiology, 7e
NAC Dosing (from Textbooks):
- Loading: 150 mg/kg IV over 1 hour
- Then: 50 mg/kg over next 4 hours
- Then: 100 mg/kg over 16 hours
- Total: 21-hour regimen (FDA-approved)
- Loading: 140 mg/kg, then 70 mg/kg every 4 hours
- Duration: 24-72 hours (6-18 doses)
"Treatment should be started as early as possible as it is practically ineffective if started 16 hours or more after paracetamol ingestion."
- P.C. Dikshit Textbook of Forensic Medicine, p. 578
"Most beneficial when administered within 8-10 hours of overdose."
- The Essentials of Forensic Medicine and Toxicology, 36th Ed.
PART 6: Glossary of Technical Terms Used
| Term | Definition |
|---|---|
| NAPQI | N-Acetyl-p-Benzoquinone Imine - the toxic intermediate metabolite of paracetamol produced by CYP2E1 |
| CYP2E1 | Cytochrome P450 2E1 - a liver enzyme responsible for the toxic oxidative metabolism of paracetamol; induced by chronic alcohol |
| Glutathione | A tripeptide (glutamate-cysteine-glycine) and the body's main antioxidant/detoxifier; neutralizes NAPQI under normal conditions |
| Hepatotoxicity | Toxic damage to liver cells (hepatocytes) |
| Centrilobular necrosis | Death of liver cells in the central zone of the liver lobule (zone 3) - the area richest in CYP enzymes and most vulnerable to NAPQI |
| Covalent binding | A chemical bond where NAPQI permanently attaches to liver cell proteins, destroying their function |
| Glucuronidation | The safe metabolic pathway where paracetamol is conjugated (joined) with glucuronic acid to form a harmless, water-soluble metabolite |
| Sulfation | Another safe metabolic pathway - conjugation of PCM with sulfate to form a harmless metabolite |
| N-Acetylcysteine (NAC) | The antidote for PCM poisoning; replenishes glutathione; most effective within 8-10 hours |
| Hepatic encephalopathy | Brain dysfunction caused by liver failure - confusion, drowsiness, coma |
| Coagulopathy | Inability of blood to clot properly, caused by liver failure (the liver makes clotting factors) |
| ALT/AST | Alanine aminotransferase / Aspartate aminotransferase - liver enzymes that rise when liver cells are damaged |
| Threshold phenomenon | Toxicity only occurs AFTER glutathione is depleted below a critical level; below that level, the body safely neutralizes NAPQI |
| Mercapturic acid | The harmless end-product formed when glutathione neutralizes NAPQI; excreted safely in urine |
| Oxidative stress | Cell damage caused by accumulation of reactive oxygen species (free radicals), triggered when NAPQI binds to mitochondria |
Quick Summary for PBL
NORMAL ADULT: Toxic >150 mg/kg (>10 g single dose); Lethal >350 mg/kg
ALCOHOLIC: Toxic at just 5-6 g/day (threshold massively reduced)
REASON: Alcohol → ↑CYP2E1 → ↑NAPQI + depleted glutathione
ANTIDOTE: NAC - replenishes glutathione; must give within 8-10 hours
- P.C. Dikshit Textbook of Forensic Medicine and Toxicology (p. 578)
- The Essentials of Forensic Medicine and Toxicology, 36th Edition (2026) (Table 31.1, 31.2, Fig. 31.1)
- Goldman-Cecil Medicine, International Edition
- Sleisenger and Fordtran's GI and Liver Disease (Table 88.5, p. 1670)
- Rosen's Emergency Medicine
- Morgan and Mikhail's Clinical Anesthesiology, 7e
Tell me the metabolism chart of pcm
-
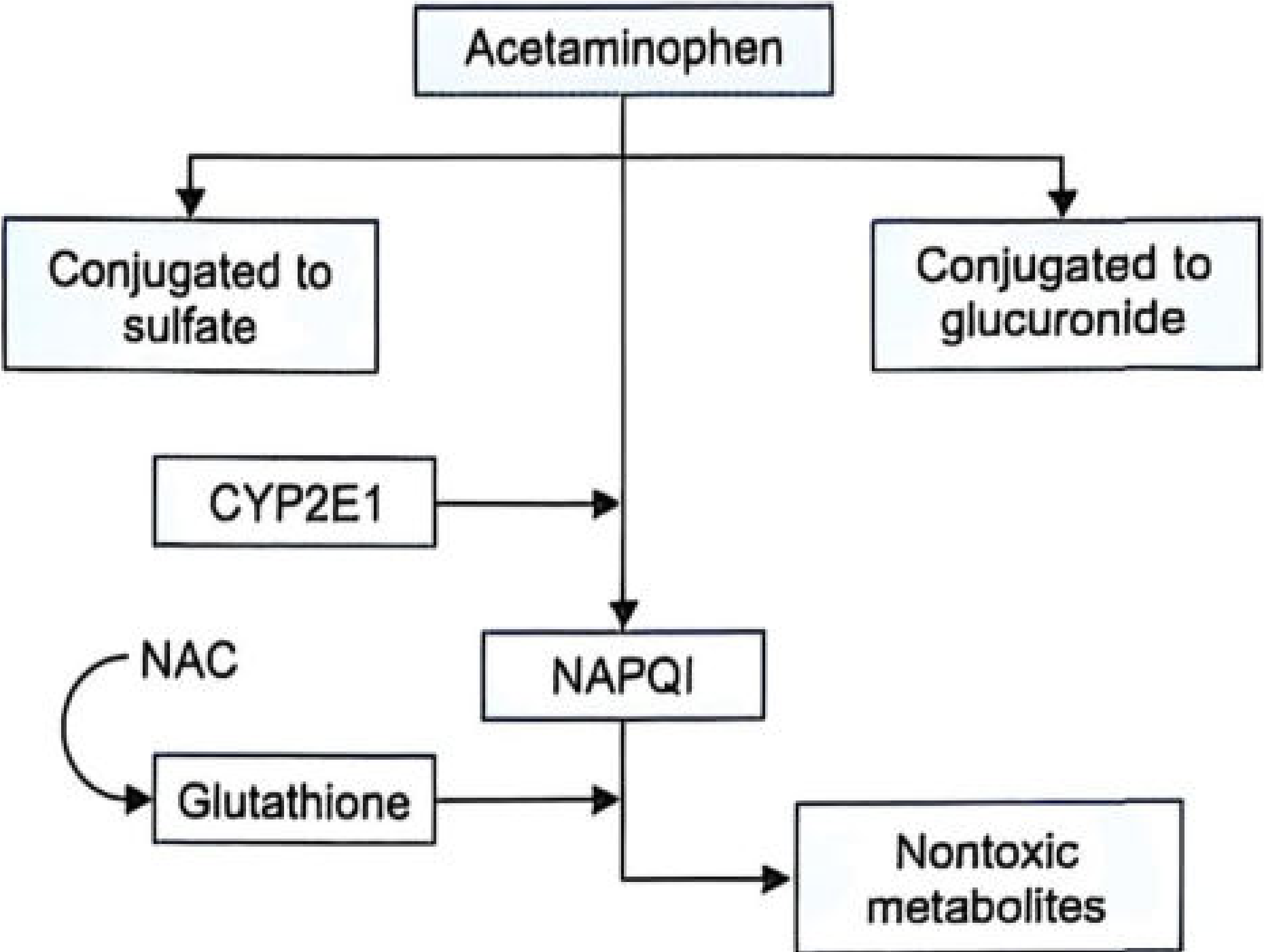
Acetaminophen (PCM) at the top splits into 3 paths:
- Left - Conjugated to sulfate (safe, non-toxic)
- Right - Conjugated to glucuronide (safe, non-toxic)
- Middle (the dangerous path) - Goes through CYP2E1 enzyme → produces NAPQI (the toxic metabolite)
-
NAPQI is then neutralized by Glutathione → forms non-toxic metabolites (safely excreted)
-
NAC (N-Acetylcysteine) shown on the left feeds into glutathione - this is exactly why NAC is the antidote. It replenishes glutathione so it can keep neutralizing NAPQI.
I am asking the metabolism pathway of PCM in a normal person.
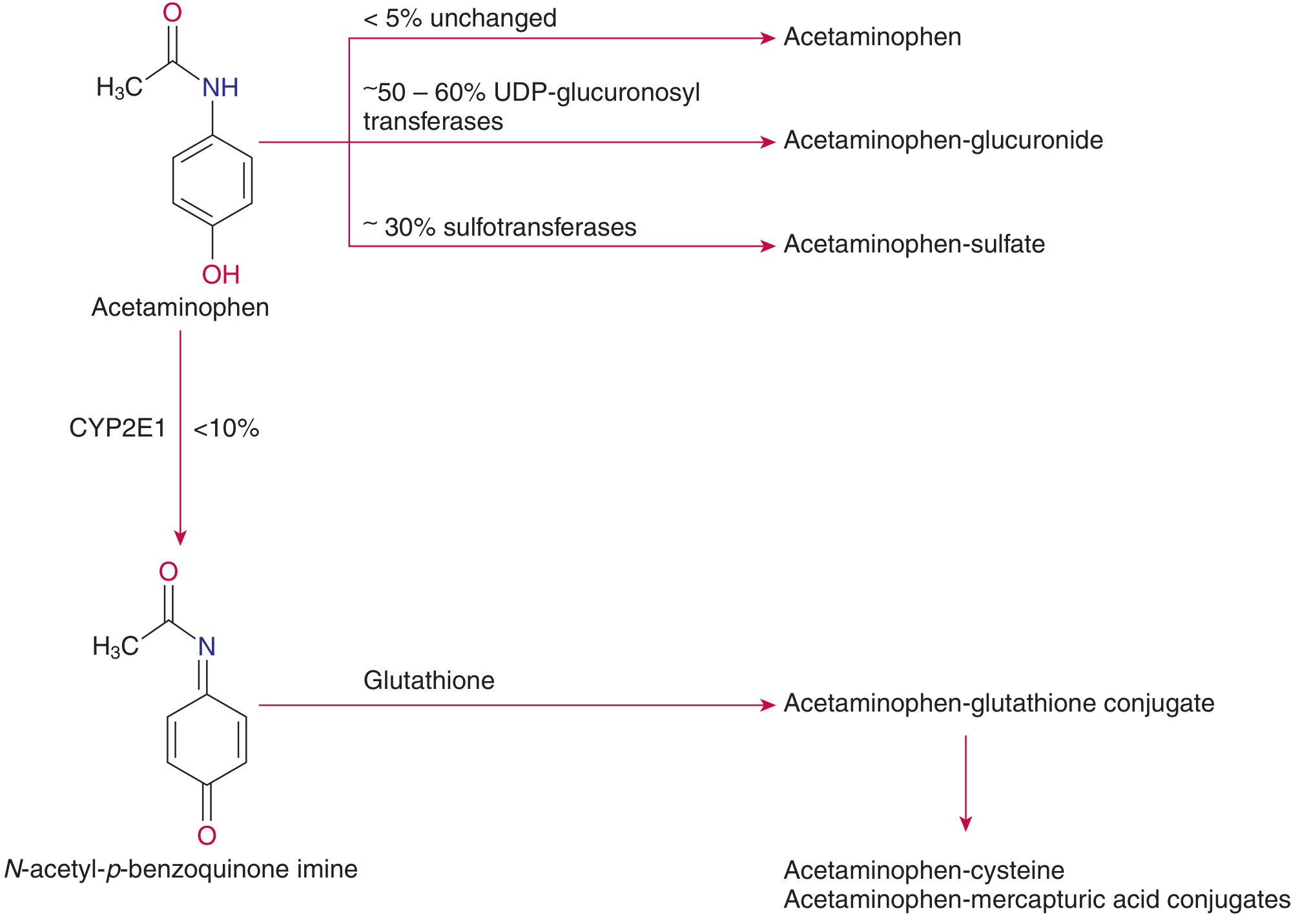
Metabolism of Paracetamol (PCM) in a Normal Person
Textbook Diagram (Figure 43.2):
Reading the Chart Step by Step:
| Route | Enzyme Used | % of Dose | Product | Safe or Toxic? |
|---|---|---|---|---|
| Glucuronidation | UDP-glucuronosyltransferases | ~50-60% | Acetaminophen-glucuronide | ✅ Safe - excreted in urine |
| Sulfation | Sulfotransferases | ~30% | Acetaminophen-sulfate | ✅ Safe - excreted in urine |
| Unchanged excretion | None | <5% | Acetaminophen unchanged | ✅ Excreted in urine |
| CYP2E1 oxidation | CYP2E1 (P450 enzyme) | <10% | NAPQI (toxic intermediate) | ⚠️ Toxic BUT neutralized by glutathione |
"Acetaminophen is normally metabolized in the liver to glucuronide (50 to 60%) and sulfate (<30%) conjugates. A smaller amount (<10%) is metabolized by a cytochrome P450 mixed-function oxidase pathway... forming NAPQI. This intermediate normally undergoes electrophilic conjugation with glutathione and then subsequent transformation to cysteine and mercapturic acid conjugates of acetaminophen."
- Tietz Textbook of Laboratory Medicine, 7th Edition
The NAPQI pathway in a NORMAL person (safe outcome):
PCM → CYP2E1 → NAPQI
↓
+ Glutathione (abundant in normal liver)
↓
Acetaminophen-glutathione conjugate
↓
Acetaminophen-CYSTEINE conjugate
+
Acetaminophen-MERCAPTURIC ACID conjugate
↓
Safely excreted in URINE
Why does this go wrong in overdose?
"With acetaminophen overdose, the sulfation pathway becomes saturated; consequently, a greater portion is metabolized by the P450 mixed-function oxidase pathway. When the tissue stores of glutathione become depleted, arylation of cellular molecules by the benzoquinoneimine intermediate leads to hepatic necrosis."
- Tietz Textbook of Laboratory Medicine, 7th Edition
Simply teach me the metabolism pathway of pcm in normal human
PCM Metabolism in a Normal Person
The Diagram (from Tietz Textbook of Laboratory Medicine, 7th Ed.):
Simple Explanation:
PCM taken orally
|
Absorbed from gut
|
Reaches LIVER
|
┌───────────────┼─────────────────┐
▼ ▼ ▼
~50-60% ~30% ~10%
GLUCURONIDATION SULFATION CYP2E1 enzyme
↓ ↓ ↓
PCM-glucuronide PCM-sulfate NAPQI
(safe, harmless) (safe, harmless) ↓
↓ ↓ + Glutathione
Excreted in Excreted in ↓
URINE URINE PCM-mercapturic acid
(safe, harmless)
↓
Excreted in URINE
In Simple Words:
| Path | What happens | Safe? |
|---|---|---|
| 50-60% | Joins with glucuronic acid → flushed out in urine | ✅ Yes |
| ~30% | Joins with sulfate → flushed out in urine | ✅ Yes |
| ~10% | Liver enzyme CYP2E1 converts it to NAPQI → glutathione immediately destroys NAPQI → flushed out in urine | ✅ Yes (in normal dose) |
Source: Tietz Textbook of Laboratory Medicine, 7th Edition, Figure 43.2
explain the chart in simple words and also define the terms
Step-by-Step Simple Explanation
STEP 1 - You swallow a PCM tablet
STEP 2 - The liver breaks PCM down into 4 routes
🔵 STREAM 1 - The Biggest Safe Route (~50-60%)
- The liver sticks a molecule called glucuronic acid onto PCM
- This makes PCM water-soluble (dissolves in water)
- The kidney then flushes it out in your urine
- Completely harmless
Terms defined:
Glucuronidation - A process where the liver adds glucuronic acid to a drug to make it water-soluble so the kidneys can remove it. Think of it as "gift wrapping" the drug so the kidney can throw it away.
UDP-glucuronosyltransferase - The enzyme (a biological tool/machine) in the liver that performs glucuronidation. "UDP" is just the energy molecule that powers this reaction.
Conjugation - The general word for "joining/attaching" one molecule to another. Glucuronidation and sulfation are both types of conjugation.
🟡 STREAM 2 - Second Safe Route (~30%)
- The liver sticks a sulfate group (a sulfur-containing molecule) onto PCM
- Again becomes water-soluble → flushed out in urine
- Completely harmless
Terms defined:
Sulfation - Similar to glucuronidation, but instead of glucuronic acid, a sulfate molecule is attached to PCM. End result is the same - PCM is made harmless and removed in urine.
Sulfotransferase - The enzyme that performs sulfation in the liver.
🟢 STREAM 3 - Tiny Unchanged Route (<5%)
- A tiny bit of PCM escapes the liver without being changed at all
- Goes straight out in urine as PCM
- Harmless (too small an amount to matter)
🔴 STREAM 4 - The Important Dangerous Route (<10%)
PCM → CYP2E1 → NAPQI (toxic!)
↓
Glutathione grabs it
↓
PCM-Glutathione conjugate
↓
PCM-Cysteine + PCM-Mercapturic acid
↓
Out in URINE (safe ✅)
All Technical Terms - Simple Definitions
| Term | Simple Definition |
|---|---|
| Metabolism | How the body chemically breaks down and processes a drug |
| Liver | The body's main "drug-processing factory" - handles almost all medications |
| Enzyme | A biological tool/machine made of protein that speeds up a chemical reaction in the body |
| Glucuronidation | Liver sticks glucuronic acid onto PCM → makes it water-soluble → kidney removes it in urine. The BIGGEST safe pathway (~50-60%) |
| Glucuronic acid | A sugar molecule that the liver attaches to drugs to make them easier to remove |
| UDP-glucuronosyltransferase | The enzyme that performs glucuronidation. "UDP" = uridine diphosphate, the energy source |
| Sulfation | Liver sticks a sulfate group onto PCM → also water-soluble → removed in urine. Second safe pathway (~30%) |
| Sulfotransferase | The enzyme that performs sulfation |
| Conjugation | "Joining" - the general term for attaching one molecule to another to make it harmless |
| CYP2E1 | Cytochrome P450 2E1 - a liver enzyme that converts PCM into the dangerous NAPQI. Works on about 10% of PCM in a normal person. Alcohol INCREASES this enzyme |
| Cytochrome P450 | A family of liver enzymes responsible for metabolising most drugs. They use oxygen to chemically modify drug molecules |
| NAPQI | N-Acetyl-p-Benzoquinone Imine - the TOXIC chemical produced from PCM by CYP2E1. The "villain" in PCM toxicity |
| Glutathione | The body's natural "fire extinguisher" - a protective molecule in the liver that grabs and neutralizes NAPQI. Made of 3 amino acids (glutamate + cysteine + glycine) |
| Glutathione conjugate | The safe product formed when glutathione grabs NAPQI - completely harmless |
| Cysteine conjugate | A further breakdown product of the glutathione conjugate - harmless, excreted in urine |
| Mercapturic acid | The final harmless end-product - excreted in urine. Seeing it in urine is proof that PCM was processed safely |
| Water-soluble | Can dissolve in water - important because kidneys can only remove water-soluble substances in urine |
| Excretion | Removing waste products from the body - mainly through urine (kidneys) |
The One-Line Summary
In a normal person, 90% of PCM is safely converted to harmless products (glucuronide + sulfate) and flushed out in urine. The remaining 10% becomes toxic NAPQI, but the liver's glutathione immediately destroys it before it can cause any harm.
what is cpk, alp,tlc what is its normal range ,significance and when does it increas
CPK, ALP, and TLC - Complete Notes for PBL
1. CPK (Creatine Phosphokinase) = Also called CK (Creatine Kinase)
What is it?
"Creatine kinase (CK) catalyzes the reversible phosphorylation of creatine by ATP... Physiologically, when muscle contracts, ATP is converted to ADP, and CK catalyzes the re-phosphorylation of ADP to ATP using creatine phosphate as the phosphorylation reservoir."
- Tietz Textbook of Laboratory Medicine, 7th Edition
Where is it found in the body?
| Source | CPK content |
|---|---|
| Skeletal muscle | Highest - 2500 U/g protein |
| Heart muscle | High - 550 U/g protein |
| Brain | Some |
| Liver & red blood cells | Almost NONE |
Normal Range
Males: 46-171 U/L | Females: 34-145 U/L (Tietz Textbook of Laboratory Medicine, 7th Edition)
CPK Isoforms (Sub-types) - Very Important!
| Isoform | Full Name | Found in | Clinical use |
|---|---|---|---|
| CK-MM (CK-3) | Muscle-Muscle | Skeletal muscle | 97-100% of normal serum CK |
| CK-MB (CK-2) | Muscle-Brain | Heart muscle | Marker of heart attack (MI) |
| CK-BB (CK-1) | Brain-Brain | Brain | Brain injury (rarely measured) |
When does CPK INCREASE?
| Cause | Why |
|---|---|
| Myocardial Infarction (heart attack) | Heart muscle cells die → CK-MB released into blood |
| Muscular Dystrophy | Muscle fibres breaking down |
| Rhabdomyolysis | Massive muscle destruction (crush injury, extreme exercise) |
| Polymyositis / Dermatomyositis | Inflammatory muscle disease |
| After surgery / IM injection | Muscle trauma |
| Hypothyroidism | Slow metabolism affects muscle |
| Strenuous exercise | Temporary rise - normal |
| Epileptic seizures | Muscle overactivity |
| Blunt chest trauma | Heart/muscle injury |
| Brain injury / stroke | CK-BB released (rarely elevated in serum) |
"An elevated serum creatine kinase (CK) concentration can result from recent exercise, electromyography (EMG), intramuscular injection, liver disease, or myocardial infarction (MI) as well as from a primary muscle disease."
- Bradley and Daroff's Neurology in Clinical Practice
"CK-MB is no longer a recommended marker for the initial diagnosis of NSTEMI. It lacks specificity because it is present in both skeletal and cardiac muscle cells... Troponin is the recommended biomarker for assessment of myocardial necrosis."
- The Washington Manual of Medical Therapeutics
2. ALP (Alkaline Phosphatase)
What is it?
Where is it found?
"Alkaline phosphatase (ALP) is expressed in liver, bile ducts, bone, intestine, placenta, kidney, and leukocytes."
- Sabiston Textbook of Surgery, The Biological Basis of Modern Surgical Practice
Normal Range
30-140 IU/L
- Bailey and Love's Short Practice of Surgery, 28th Edition - Table 69.1
ALP Isoforms by source:
| Source | When elevated |
|---|---|
| Liver ALP | Liver disease, biliary obstruction |
| Bone ALP | Bone disorders, fractures, growing children |
| Placental ALP | Normal in pregnancy |
| Intestinal ALP | Intestinal disease |
When does ALP INCREASE?
| Cause | Explanation |
|---|---|
| Cholestasis (blocked bile flow) | ALP is most elevated here - bile duct obstruction causes ALP to be produced in huge amounts |
| Biliary obstruction (gallstones, tumour) | Bile backs up → ALP rises dramatically |
| Hepatitis / Liver disease | Liver cell damage |
| Liver cancer / metastasis | Tumour stimulates ALP production |
| Primary Biliary Cirrhosis | Autoimmune bile duct destruction |
"The serum ALP is particularly elevated with cholestatic liver disease or biliary obstruction."
- Bailey and Love's Short Practice of Surgery, 28th Edition
| Cause | Explanation |
|---|---|
| Paget's Disease of bone | Overactive bone remodelling |
| Bone fractures (healing) | Bone formation requires ALP |
| Bone cancer / metastasis | Tumour invades bone |
| Osteomalacia / Rickets | Vitamin D deficiency → abnormal bone |
| Hyperparathyroidism | Excess PTH stimulates bone breakdown |
| Growing children | Normally higher due to bone growth |
- Pregnancy (placental ALP - normal)
- Prostate cancer with bone metastasis
"It is important to note that routine laboratory analysis of ALP is not isoform specific and so ALP from a skeletal source may also lead to elevation, particularly Paget's disease and prostate cancer."
- Bailey and Love's Short Practice of Surgery, 28th Edition
- If GGT is also raised → ALP is from the liver
- If GGT is normal → ALP is from bone
3. TLC (Total Leukocyte Count) = WBC Count (White Blood Cell Count)
What is it?
Normal Range
4,500 - 10,000 cells/μL (mean = 7,500/μL)
- Goldman-Cecil Medicine, International Edition
WBC Differential (breakdown of types):
| Cell Type | % of WBC | Function |
|---|---|---|
| Neutrophils | ~60% | Fight bacteria (most important) |
| Lymphocytes | ~30% | Fight viruses, produce antibodies |
| Monocytes | ~5% | Engulf and destroy pathogens |
| Eosinophils | ~2-4% | Fight parasites, allergic reactions |
| Basophils | ~0.5-1% | Allergic reactions |
"The normal peripheral white blood cell count ranges between 4500/μL and 10,000/μL, with a mean of 7500/μL, and is composed of neutrophils, lymphocytes, monocytes, basophils, and eosinophils. Because neutrophils usually represent about 60% of the peripheral WBC, derangement in the WBC usually reflects elevation or reduction in the absolute neutrophil count."
- Goldman-Cecil Medicine, International Edition
When TLC INCREASES (Leukocytosis = WBC > 10,000/μL):
| Cause | Type of WBC elevated |
|---|---|
| Bacterial infection | Neutrophilia (↑ neutrophils) |
| Viral infection | Lymphocytosis (↑ lymphocytes) |
| Parasitic infection / Allergy | Eosinophilia (↑ eosinophils) |
| Sepsis / severe infection | Very high neutrophils + "left shift" |
| Leukaemia (blood cancer) | All types - massive increase |
| Myocardial Infarction | Reactive neutrophilia |
| Chronic inflammation | Neutrophilia (e.g., TB, abscess, Crohn's) |
| Corticosteroid drugs | Neutrophilia |
| Cigarette smoking | Neutrophilia |
| Post-splenectomy | Lymphocytosis |
| Physical/emotional stress | Neutrophilia (mobilized from marginated pool) |
"Many acute bacterial infections can present with leukocytosis with a 'left shift', referring to the circulation of more immature myeloid cells."
- Goldman-Cecil Medicine, International Edition
When TLC DECREASES (Leukopenia = WBC < 4,000/μL):
| Cause | Explanation |
|---|---|
| Viral infections (HIV, dengue, typhoid) | Virus suppresses marrow |
| Bone marrow failure | Not producing enough cells |
| Chemotherapy / radiation | Destroys marrow cells |
| Autoimmune disease (SLE) | Antibodies destroy WBCs |
| Severe sepsis / early sepsis | WBCs consumed rapidly |
| Nutritional deficiency (B12, folate) | Marrow needs these to make cells |
Quick Summary Table
| Test | Full Form | Normal Range | Main Organ | Increases When |
|---|---|---|---|---|
| CPK/CK | Creatine Phosphokinase | 46-171 U/L (M), 34-145 U/L (F) | Skeletal muscle, Heart | MI, muscle disease, trauma, rhabdomyolysis |
| ALP | Alkaline Phosphatase | 30-140 IU/L | Liver, Bone | Biliary obstruction, cholestasis, bone disease |
| TLC | Total Leukocyte Count | 4,500-10,000/μL | Blood (bone marrow) | Infection, inflammation, leukaemia, drugs |
- Tietz Textbook of Laboratory Medicine, 7th Edition (CPK normal range, isoenzymes)
- Bailey and Love's Short Practice of Surgery, 28th Edition (ALP normal range, Table 69.1)
- Goldman-Cecil Medicine, International Edition (TLC normal range, leukocytosis)
- Sabiston Textbook of Surgery (ALP sources)
- Bradley and Daroff's Neurology in Clinical Practice (CPK causes)
Tell me about HPE report
HPE Report (Histopathological Examination Report)
What is HPE?
- Normal
- Inflamed / infected
- Benign (non-cancerous)
- Malignant (cancerous)
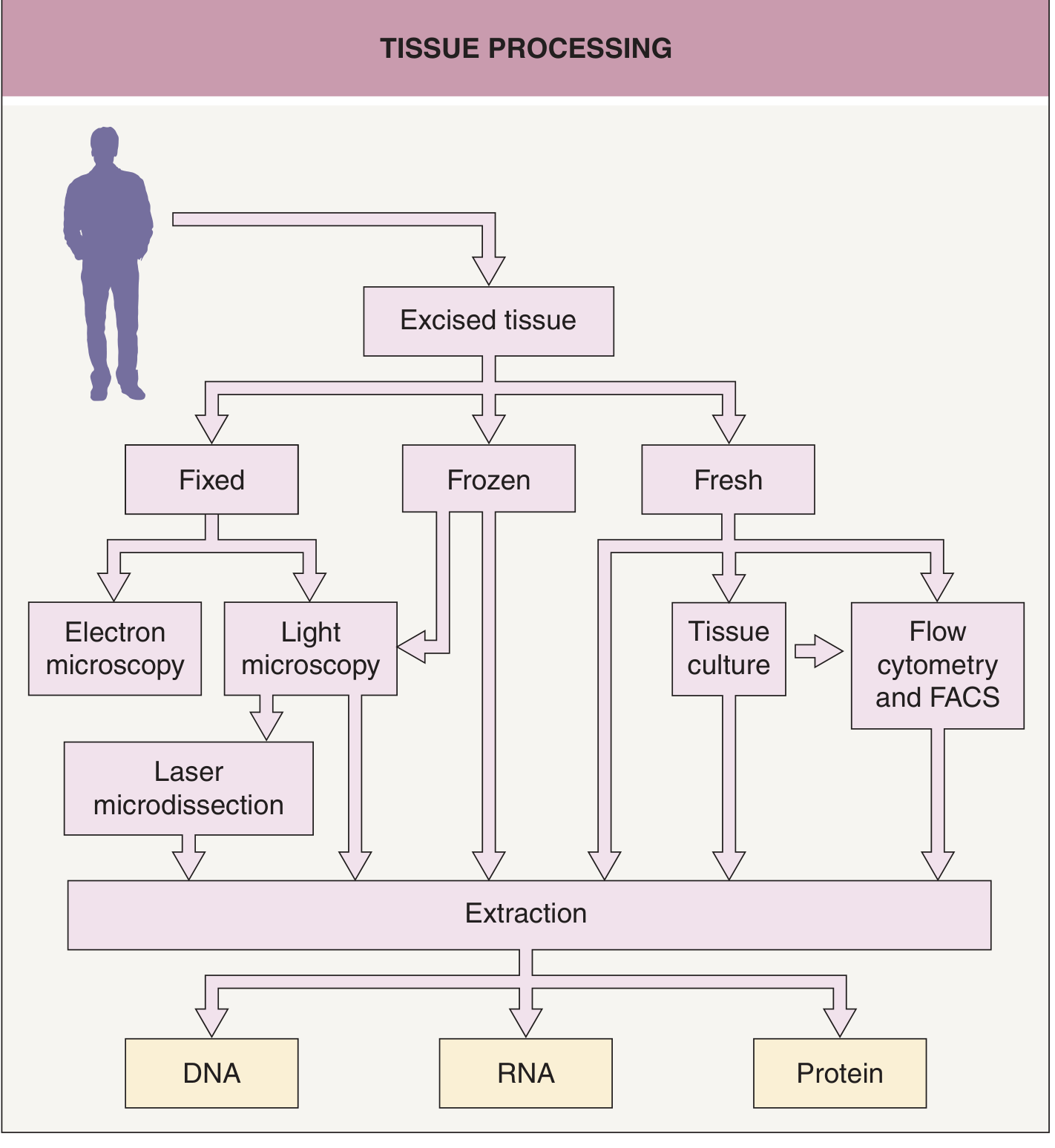
"Dermatologists are accustomed to placing a biopsy specimen in formalin followed by paraffin embedding and then staining tissue sections with hematoxylin and eosin. However, this is just one of several possible starting points for tissue processing."
- Dermatology, 2-Volume Set, 5th Edition
How Is a Tissue Sample Processed Before the Report?
Diagram (from Dermatology, 5th Ed., Fig. 3.1):
Step-by-Step Process (from Biopsy to Report):
PATIENT
↓
BIOPSY taken (tissue removed)
↓
FIXATION in 10% formalin
(preserves the tissue, prevents decay)
↓
PROCESSING & PARAFFIN EMBEDDING
(tissue hardened in wax block so it can be cut thin)
↓
SECTIONING
(very thin slices cut with a machine called microtome - 3-5 micrometres thick)
↓
STAINING (most common = H&E stain)
Hematoxylin → stains NUCLEUS blue/purple
Eosin → stains CYTOPLASM pink
↓
MICROSCOPIC EXAMINATION by Pathologist
↓
HPE REPORT written
"By placing the sample in formalin (for light microscopy), glutaraldehyde (for electron microscopy), or freezing a fresh sample before processing and sectioning, the sample can be analyzed histologically in various ways."
- Dermatology, 5th Edition
What Does an HPE Report Contain?
SECTION 1 - Patient Information (Header)
- Patient name, age, sex
- Hospital/lab registration number
- Referring doctor's name
- Date of biopsy and date of report
SECTION 2 - Clinical Information
- Why the biopsy was taken (clinical diagnosis/suspicion)
- Site of biopsy (e.g., "mass from right breast", "polyp from sigmoid colon")
- Type of specimen (e.g., fine needle aspirate, core biopsy, excision biopsy, surgical specimen)
SECTION 3 - Gross Examination (Macroscopic / Naked Eye)
| What is noted | Example |
|---|---|
| Type of specimen | Excision biopsy, wedge biopsy, mastectomy specimen |
| Size | 3 cm × 2 cm × 1.5 cm |
| Shape | Oval, irregular, lobulated |
| Colour | Grey-white, yellow, red, brown |
| Consistency | Soft, firm, hard, rubbery |
| Cut surface | Homogeneous, necrotic areas, cystic spaces |
| Margin | Well-defined vs poorly defined |
| Capsule | Present or absent |
| Number of pieces | "Received in multiple fragments" |
SECTION 4 - Microscopic Examination (The Most Important Part)
| What is noted | Details |
|---|---|
| Type of cells | Epithelial, mesenchymal, inflammatory, etc. |
| Cell arrangement | Sheets, glands, nests, cords |
| Nuclear features | Size, shape, chromatin pattern, nucleoli |
| Mitotic figures | Number of dividing cells (important in cancer) |
| Necrosis | Areas of dead tissue |
| Invasion | Does tumour invade blood vessels, nerves, margins? |
| Inflammation | Type - acute (neutrophils), chronic (lymphocytes, plasma cells, granulomas) |
| Stroma | Supporting connective tissue |
| Margins | Are the cut edges free of disease? |
| Special stains | PAS, ZN, Congo red - if needed |
SECTION 5 - Diagnosis (Final Impression)
- "Sections show features consistent with moderately differentiated adenocarcinoma"
- "Features consistent with chronic granulomatous inflammation - suggestive of tuberculosis"
- "Benign fibroadenoma of the breast"
- "Reactive lymph node - no evidence of malignancy"
- "Acute appendicitis with periappendicitis"
SECTION 6 - Additional Tests (if done)
| Test | What it does |
|---|---|
| Immunohistochemistry (IHC) | Uses antibodies to identify specific proteins in cells (e.g., ER/PR/HER2 in breast cancer) |
| Special stains | PAS (fungi/glycogen), ZN (TB bacilli), Congo red (amyloid), Gram stain (bacteria) |
| FNAC | Fine Needle Aspiration Cytology - cells examined (not a full tissue section) |
Key Terms in an HPE Report - Defined Simply
| Term | Simple Definition |
|---|---|
| Biopsy | Removing a small piece of tissue from the body to examine it |
| Histopathology | "Histo" = tissue; "Patho" = disease; "Logy" = study of. Study of diseased tissue under microscope |
| Fixation | Preserving the tissue with a chemical (usually 10% formalin) to prevent it from decaying |
| Formalin | The chemical (formaldehyde solution) used to fix/preserve tissue for HPE |
| Paraffin embedding | Hardening tissue in wax so it can be cut into very thin slices |
| Microtome | The machine that cuts tissue into very thin sections (3-5 micrometres) |
| H&E stain | Hematoxylin & Eosin - the most common stain. Blue = nucleus, Pink = cytoplasm |
| Gross examination | Examining the specimen with the naked eye |
| Microscopic examination | Examining stained tissue sections under a microscope |
| Benign | Non-cancerous - does not invade or spread |
| Malignant | Cancerous - invades surrounding tissue and can spread (metastasize) |
| Differentiation | How much cancer cells look like normal cells. Well differentiated = looks more normal = less aggressive. Poorly differentiated = looks very abnormal = more aggressive |
| Mitotic figures | Cells caught in the process of dividing; many = fast-growing tumour |
| Necrosis | Areas of dead/dying tissue within the tumour |
| Margins | The cut edges of the removed tissue. "Clear margins" = no cancer at the edge = good |
| IHC (Immunohistochemistry) | A special technique using antibodies to identify specific proteins/markers in cells |
| FNAC | Fine Needle Aspiration Cytology - a quick test where cells (not full tissue) are sucked out with a needle and examined |
| Frozen section | Tissue rapidly frozen and examined while patient is still in the operation theatre - gives quick diagnosis |
| Granuloma | A special type of inflammation formed when the immune system walls off something it cannot destroy (e.g., TB bacteria, fungi) |
Types of Biopsy
| Type | How done | Used for |
|---|---|---|
| FNAC | Thin needle sucks cells | Quick diagnosis, lymph nodes, thyroid, breast lumps |
| Core/Tru-cut biopsy | Thick needle takes a core of tissue | Liver, kidney, breast, prostate |
| Incisional biopsy | Part of the lesion removed | Large tumours |
| Excisional biopsy | Entire lesion removed | Small lumps (diagnostic + curative) |
| Punch biopsy | Circular punch removes skin plug | Skin lesions |
| Frozen section | Rapid intraoperative biopsy | During surgery to guide the surgeon |
Quick Summary
BIOPSY → FORMALIN FIXATION → PARAFFIN EMBEDDING
→ THIN SECTIONS (microtome) → H&E STAINING
→ MICROSCOPE EXAMINATION by PATHOLOGIST
→ HPE REPORT:
1. Patient details
2. Clinical history
3. Gross (naked eye) description
4. Microscopic description
5. DIAGNOSIS (benign / malignant / inflammatory etc.)
6. Special stains / IHC if needed
what does pleomorphic cells with hyperchromatic nuclei, bizarre tumor giant cells with production of unmineralized bones means?
What Does That HPE Description Mean?
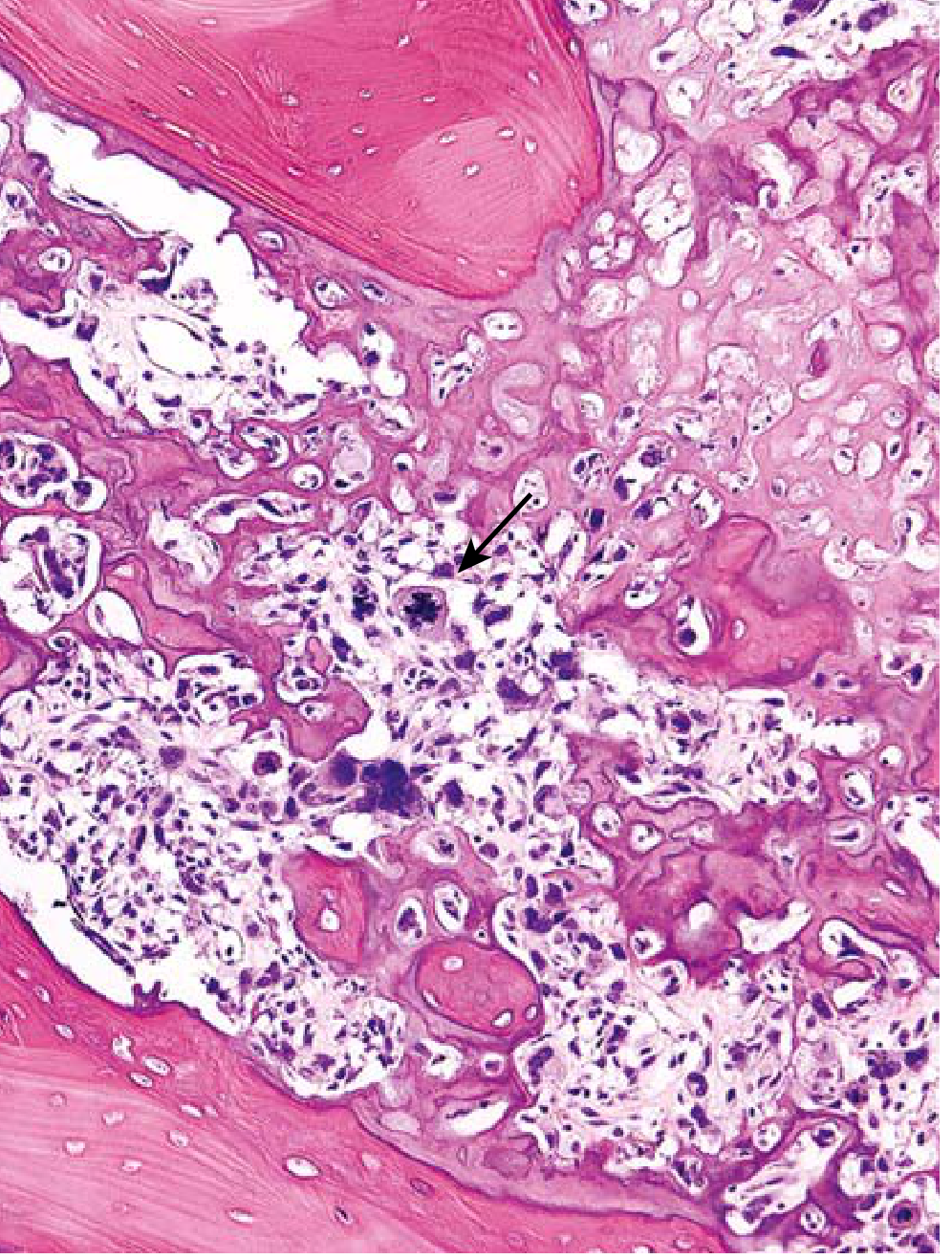
"Pleomorphic cells with hyperchromatic nuclei, bizarre tumor giant cells with production of unmineralized bone"
"The tumor cells demonstrate pleomorphism, large hyperchromatic nuclei, bizarre tumor giant cells, and abundant mitoses including abnormal (e.g., bipolar) forms... Diagnosis of osteosarcoma requires the presence of malignant tumor cells producing unmineralized osteoid or mineralized bone, which is typically fine and lacelike but can also appear as broad sheets or primitive trabeculae."
- Robbins & Kumar Basic Pathology, p. 783
Microscopic Image (H&E stain of Osteosarcoma):
X-Ray of Osteosarcoma (for context):

Now Let's Break Down Each Term Simply
1. "Pleomorphic cells"
- "Pleo" = many / "morph" = shape
- In a NORMAL tissue, all cells look roughly the same - same size, same shape
- In a MALIGNANT (cancerous) tumour, cells look wildly different from each other - some are huge, some small, odd shapes
- This variation is called pleomorphism - it is a hallmark sign of malignancy
- The more pleomorphic the cells, the MORE aggressive and malignant the tumour
2. "Hyperchromatic nuclei"
- "Hyper" = too much / "chromatic" = colour/stain
- In H&E staining, a normal nucleus stains light blue/purple
- In cancer cells, the nucleus stains VERY DARK (intensely blue/purple)
- Why? Because cancer cells have MORE DNA than normal - extra chromosomes, genetic material - so more hematoxylin binds, making it darker
- Also the nucleus is often ENLARGED (big nucleus relative to cytoplasm = high N:C ratio)
3. "Bizarre tumor giant cells"
- Normal cells have ONE nucleus
- In highly malignant tumours, cell division goes wrong - the cell grows huge and ends up with 2, 3, or even many nuclei in one giant cell
- Called "bizarre" because they look completely abnormal - no resemblance to any normal cell type
- These are NOT the same as the "foreign body giant cells" seen in inflammation - these are MALIGNANT giant cells
4. "Production of unmineralized bone" (= Osteoid production)
- Osteoid = unmineralized bone = the organic matrix of bone (mainly collagen) BEFORE calcium is deposited into it
- Normal bone formation: Osteoblasts lay down osteoid → then calcium minerals are deposited → becomes hard bone
- In osteosarcoma: the malignant (cancer) cells are producing this osteoid matrix, BUT it is abnormal and often NOT properly mineralized
- Seeing malignant cells producing osteoid/bone matrix is the absolute diagnostic requirement for osteosarcoma
"Diagnosis of osteosarcoma requires the presence of malignant tumor cells producing unmineralized osteoid or mineralized bone"
- Robbins & Kumar Basic Pathology
What is Osteosarcoma?
"Osteosarcoma is a malignant tumor that produces osteoid matrix or mineralized bone. Excluding hematopoietic tumors, osteosarcoma is the most common primary malignant tumor of bone."
- Robbins & Kumar Basic Pathology
| Feature | Details |
|---|---|
| Who gets it? | 75% in people under 20 years (adolescents) - second peak in elderly |
| Where? | Metaphysis of long bones - 50% near the knee (distal femur or proximal tibia) |
| Sex | Males > Females (1.6:1) |
| Presentation | Painful, progressively enlarging mass; sometimes pathological fracture |
| X-ray sign | Codman triangle - periosteum lifted by tumour |
| Spreads to | Lungs (most common), bones, brain - via bloodstream |
| 5-year survival | ~70% without metastasis (with chemotherapy) |
Summary: What the HPE Description Means
| HPE Finding | Simple Meaning | Significance |
|---|---|---|
| Pleomorphic cells | Cells vary wildly in size and shape | Sign of malignancy |
| Hyperchromatic nuclei | Nuclei stain very dark due to excess DNA | Sign of malignancy / rapid division |
| Bizarre tumor giant cells | Abnormally huge cells with multiple nuclei | Highly malignant, aggressive tumour |
| Unmineralized bone (osteoid) production by malignant cells | Cancer cells making defective bone matrix | Diagnostic of OSTEOSARCOMA |
what is displacia and tels it symptoms and also tell how osteoblast controls osteoclast and if type I collagen is present in bone cartilage, Type II collagen in bone then where type III and IV are found
Three Topics Answered from Medical Textbooks
PART 1: What is Dysplasia?
Important Note First:
"It is important to note that as used in bone biology the term dysplasia refers to an abnormal pattern of growth rather than a premalignant lesion."
- Robbins & Kumar Basic Pathology
A. Dysplasia in General Pathology (Cells/Epithelium)
"Dysplasia: Premalignant change in the epithelium displaying proliferation of parabasal cells with disordered polarity, loss of cellular junctions, coarse nuclear chromatin clumping, abnormal nuclear cytoplasmic ratio, and high mitotic index. Reported as mild, moderate, and severe dysplasia."
- Pfenninger and Fowler's Procedures for Primary Care, 3rd Edition
Features / "Symptoms" of Dysplasia (under microscope):
| Feature | What it means simply |
|---|---|
| Disordered polarity | Cells no longer arranged neatly in layers - look jumbled |
| Loss of cellular junctions | Cells losing their connections to each other |
| Coarse nuclear chromatin clumping | The DNA inside the nucleus clumps up, stains dark (hyperchromasia) |
| Abnormal N:C ratio | Nucleus is too large compared to the cytoplasm |
| High mitotic index | Too many cells dividing at once |
| Pleomorphism | Cells vary in size and shape |
| Loss of normal maturation | Cells do not mature from bottom to top of epithelium normally |
Grades of Dysplasia:
NORMAL CELLS
↓ (changes begin)
MILD DYSPLASIA → lower 1/3 of epithelium affected
MODERATE DYSPLASIA → lower 2/3 affected
SEVERE DYSPLASIA → full thickness affected (= Carcinoma in situ)
↓ (if untreated)
INVASIVE CANCER
B. Dysplasia in Bone/Skeletal Biology
"Developmental disorders may be caused by localized abnormalities (dysostosis) or global disorganization of bone and/or cartilage (dysplasia). More than 350 skeletal dysostoses and dysplasias have been described."
- Robbins & Kumar Basic Pathology
- Achondroplasia - most common skeletal dysplasia, cause of dwarfism. Short limbs, large head.
- Thanatophoric dysplasia - most common lethal form of dwarfism
- Fibrous dysplasia - normal bone replaced by fibrous tissue and woven bone
PART 2: How Does Osteoblast Control Osteoclast?
The RANKL - RANK - OPG System
Diagram (from Robbins & Kumar Basic Pathology, Fig. 19.4):
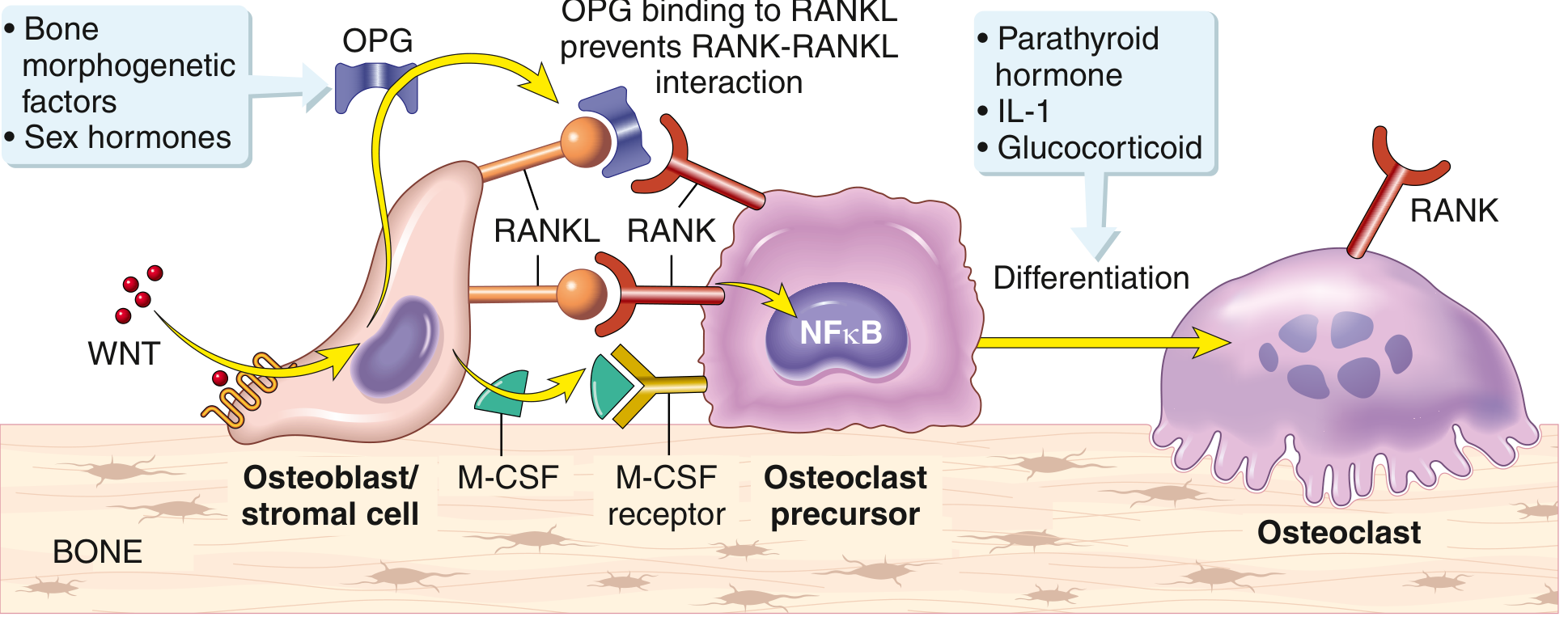
How It Works - Step by Step:
"Osteoblast/stromal cell membrane-associated RANKL binds to its receptor RANK located on the cell surface of osteoclast precursors. Signals transduced by RANK and macrophage colony-stimulating factor (M-CSF) receptor cause the precursor cells to differentiate into functional osteoclasts. By contrast, WNT protein binding triggers stromal cells/osteoblasts to secrete osteoprotegerin (OPG), a 'decoy' receptor that prevents RANKL from binding the RANK receptor. Consequently, OPG prevents bone resorption by inhibiting osteoclast differentiation."
- Robbins & Kumar Basic Pathology, p. 772
Simple Explanation:
OSTEOBLAST
↓ produces
RANKL (signal molecule)
↓ binds to
RANK receptor on Osteoclast Precursor
↓ activates
NFκB signaling pathway
↓ causes
Osteoclast Precursor → MATURE OSTEOCLAST
↓
BONE RESORPTION (bone is broken down)
OSTEOBLAST receives WNT signal
↓ produces
OPG (Osteoprotegerin) = the "decoy receptor"
↓ OPG grabs onto RANKL before it reaches RANK
RANKL is blocked - cannot reach RANK
↓
No osteoclast activation
↓
BONE RESORPTION STOPS
Other factors that increase osteoclast activity (increase RANKL or suppress OPG):
| Factor | Effect |
|---|---|
| Parathyroid hormone (PTH) | ↑ RANKL → more osteoclasts → bone resorption |
| IL-1 (Interleukin-1) | ↑ osteoclast activity |
| Glucocorticoids (steroids) | ↑ osteoclast activity → osteoporosis |
| Sex hormones (oestrogen) | ↑ OPG → protect bone (why post-menopausal women get osteoporosis) |
| Bone morphogenetic factors | ↑ OPG → protect bone |
PART 3: Where Are Type III and Type IV Collagen Found?
- Type I collagen → Bone, tendon, skin ✅
- Type II collagen → Cartilage, vitreous body of eye ✅ (NOT in bone)
Master Collagen Table:
| Type | Found In | Function |
|---|---|---|
| Type I | Bone, tendon, skin, dentin | Resistance to TENSION (pulling force) |
| Type II | Cartilage, vitreous body of eye | Resistance to PRESSURE |
| Type III | Skin, muscle, blood vessels, intestines, fetal tissues | Structural maintenance in EXPANSIBLE (stretchy) organs |
| Type IV | ALL basement membranes (under every epithelium) | Support of epithelial cells; FILTRATION |
Type III Collagen - Where and Why?
"Type III collagen: found in skin, muscle, blood vessels, frequently together with type I. Function: structural maintenance in expansible organs."
- Junqueira's Basic Histology, 17th Edition
- Blood vessel walls (arteries stretch with each heartbeat)
- Uterus (expands during pregnancy)
- Liver, spleen (soft organs with lots of cells)
- Fetal skin
- Intestinal walls
- Lymph nodes (reticular framework)
"Type III collagen distribution: Fetal skin; blood vessels, intestines."
- Andrews' Diseases of the Skin
Type IV Collagen - Where and Why?
"The basal lamina is a thin meshwork of type IV collagen and laminin produced by the epithelial cells."
- Junqueira's Basic Histology, 17th Edition
"Type IV collagen: found in all basal and external laminae. Function: support of epithelial cells; filtration."
- Junqueira's Basic Histology, 17th Edition
- Under all skin epithelium
- Under gut epithelium
- Under lung epithelium
- Kidney glomerular basement membrane (filtration!)
- Blood vessel basement membrane
- Muscle basement membrane
- Nerve sheaths
Simple Memory Table for Exams:
| Collagen Type | Memory Trick | Location |
|---|---|---|
| Type I | "I am strong" = 1st and strongest | Bone, Tendon, Skin - "BTS" |
| Type II | "II withstand pressure" | Cartilage, Vitreous - "CV" |
| Type III | "III elastic/stretchy" = reticular fibres | Blood vessels, Skin, Muscle - stretchy organs |
| Type IV | "IV is like a floor/net" = basement membrane | Basement membrane everywhere - filtration |
Sources:
- Robbins & Kumar Basic Pathology - Dysplasia definition, RANKL/OPG diagram (Fig. 19.4)
- Junqueira's Basic Histology, Text and Atlas, 17th Edition - Collagen types table
- Andrews' Diseases of the Skin - Collagen types table (Table 25.1)
- Pfenninger and Fowler's Procedures for Primary Care, 3rd Edition - Dysplasia definition
- Histology: A Text and Atlas with Correlated Cell and Molecular Biology - Type III & IV collagen in basement membrane
i didnt understand the defn
tumor of distal end of femur and classification of bone tumor
Tumours of the Distal Femur & Classification of Bone Tumours
PART 1: Classification of Bone Tumours
Source: Robbins & Kumar Basic Pathology - Table 19.1
Master Classification Table (Table 19.1 from Robbins):
| Category | Behaviour | Tumour Type | Location | Age (yrs) |
|---|---|---|---|---|
| Cartilage-forming | Benign | Osteochondroma | Metaphysis of long bones | 10-30 |
| Benign | Chondroma (Enchondroma) | Small bones of hands/feet | 30-50 | |
| Malignant | Chondrosarcoma | Pelvis, shoulder | 40-60 | |
| Bone-forming | Benign | Osteoid osteoma | Metaphysis of long bones | 10-20 |
| Benign | Osteoblastoma | Vertebral column | 10-20 | |
| Malignant | Osteosarcoma | Metaphysis of distal femur, proximal tibia | 10-20 | |
| Unknown origin | Benign | Giant Cell Tumour | Epiphysis of long bones | 20-40 |
| Benign | Aneurysmal Bone Cyst | Proximal tibia, distal femur, vertebra | 10-20 | |
| Malignant | Ewing Sarcoma | Diaphysis of long bones | 10-20 |
Simple Visual Summary - Bone Parts and Which Tumour Goes Where:
EPIPHYSIS ← Giant Cell Tumour (GCT)
─────────
METAPHYSIS ← Osteosarcoma, Osteoid Osteoma
─────────
DIAPHYSIS ← Ewing Sarcoma
─────────
METAPHYSIS ← Osteosarcoma
─────────
EPIPHYSIS ← Giant Cell Tumour
- Epiphysis = Every Giant Cell Tumour lives here
- Metaphysis = Most Osteosarcomas live here
- Diaphysis = Diaphysis = Ewing's
PART 2: Tumours of the Distal End of Femur
TUMOUR 1: OSTEOSARCOMA (at the METAPHYSIS of distal femur)
"Osteosarcoma is the most common primary malignant tumour of bone... In adolescents, tumours usually arise in the metaphyseal region of the long bones; almost 50% are near the knee in the distal femur or proximal tibia."
- Robbins & Kumar Basic Pathology, p. 782
| Feature | Details |
|---|---|
| Location in bone | METAPHYSIS (growing zone) of distal femur |
| Age | 10-20 years (adolescents) - peak in growth spurt |
| Sex | Males > Females |
| Presentation | Painful, progressively enlarging mass; pathological fracture |
| X-ray sign | Codman triangle - periosteum lifted up; "sunburst pattern" |
| HPE | Pleomorphic cells, hyperchromatic nuclei, bizarre giant cells, malignant cells producing OSTEOID (unmineralized bone) |
| Treatment | Chemotherapy (neoadjuvant) + Surgery + Adjuvant chemotherapy |
| 5-year survival | ~70% without metastasis |
| Spreads to | Lungs (haematogenous spread) |
TUMOUR 2: GIANT CELL TUMOUR (GCT) (at the EPIPHYSIS of distal femur)
"Giant cell tumors arise in the epiphyses of long bones, most commonly the distal femur and proximal tibia. This location is distinctive, setting it apart from most other bone tumours."
- Robbins & Kumar Basic Pathology, p. 787
| Feature | Details |
|---|---|
| Location in bone | EPIPHYSIS of distal femur |
| Age | 20-40 years |
| Behaviour | Benign BUT locally aggressive |
| Presentation | Arthritis-like symptoms (near the joint!); pathological fracture |
| X-ray sign | Purely LYTIC lesion; "soap bubble" appearance; cortex destruction |
| HPE | Multinucleate osteoclast-type giant cells with 100 or more nuclei + mononuclear stromal cells |
| Treatment | Curettage; RANKL inhibitor (Denosumab) if surgery too risky |
| Recurrence | 40-60% recur locally |
| Metastasis | ~4% go to lungs (but most can be cured by excision) |
X-ray of Giant Cell Tumour (distal area of long bone):

Microscopic (HPE) Image of Giant Cell Tumour:
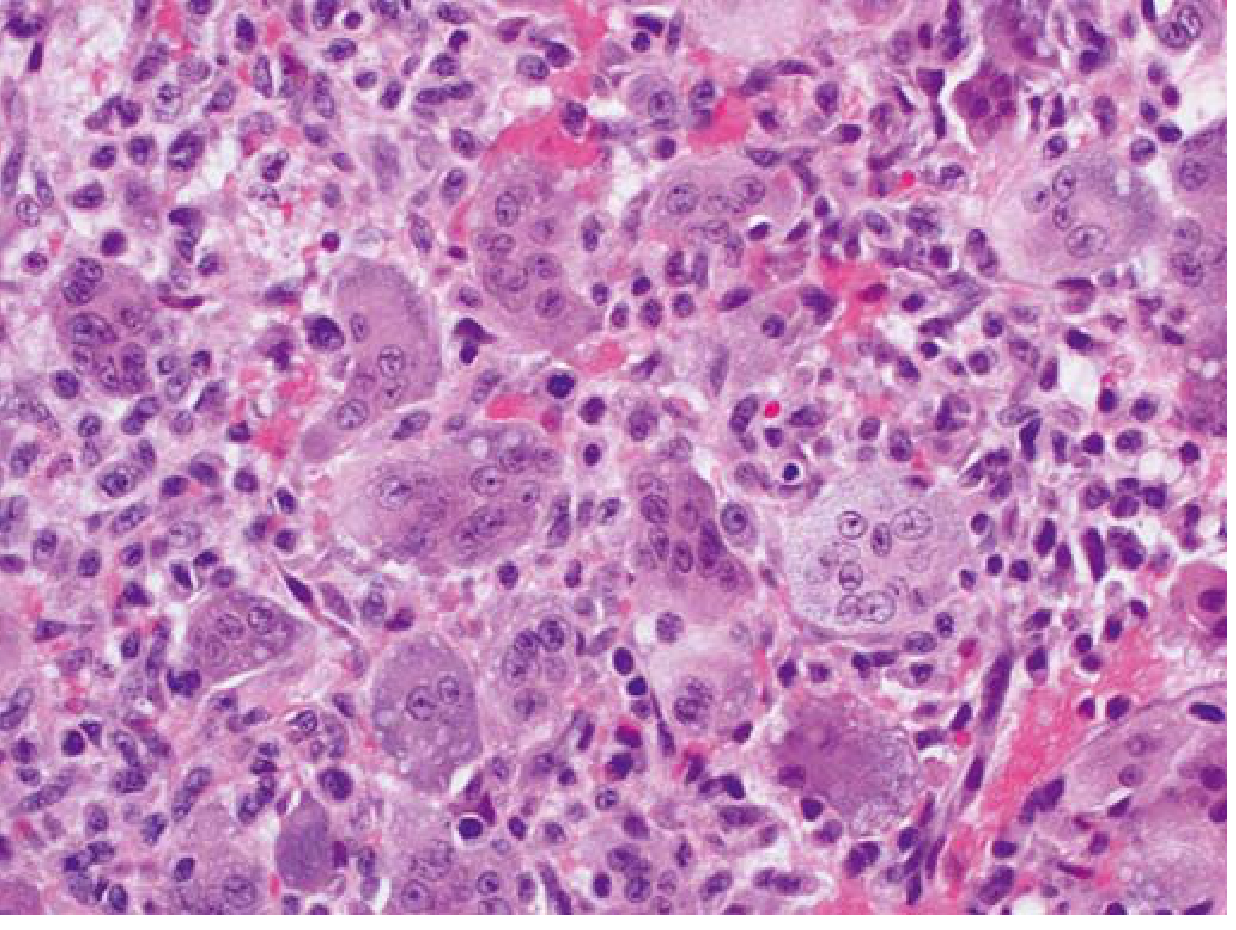
Why Does GCT Destroy Bone? (Pathogenesis)
"The neoplastic cells are primitive osteoblast precursors that express high levels of RANKL, which promotes the proliferation of osteoclast precursors and their differentiation into mature osteoclasts. The absence of normal feedback between osteoblasts and osteoclasts results in localized, but highly destructive, bone resorption."
- Robbins, Cotran & Kumar Pathologic Basis of Disease
Comparing the Two Main Distal Femur Tumours:
| Feature | Osteosarcoma | Giant Cell Tumour |
|---|---|---|
| Location in bone | METAPHYSIS | EPIPHYSIS |
| Age | 10-20 years | 20-40 years |
| Behaviour | Malignant | Benign (locally aggressive) |
| X-ray | Mixed lytic/sclerotic + Codman triangle | Purely lytic, "soap bubble" |
| HPE hallmark | Malignant cells making osteoid | Giant cells with 100+ nuclei |
| Spread | Lungs (haematogenous) | Rarely to lungs (4%) |
| Treatment | Chemo + Surgery | Curettage / Denosumab |
Other Tumours That Can Occur at the Distal Femur:
| Tumour | Type | Notes |
|---|---|---|
| Aneurysmal Bone Cyst | Benign | Blood-filled cystic spaces; age 10-20 |
| Osteochondroma | Benign | Bony projection with cartilage cap; at metaphysis |
| Ewing Sarcoma | Malignant | More in diaphysis; "onion-skin" periosteal reaction on X-ray |
| Chondrosarcoma | Malignant | Produces cartilage; usually in older adults |
Sources:
- Robbins & Kumar Basic Pathology - Table 19.1, FIG. 19.24, FIG. 19.25, p. 782-787
- Robbins, Cotran & Kumar Pathologic Basis of Disease - Giant Cell Tumour pathogenesis
- Miller's Review of Orthopaedics, 9th Edition - Classification of primary bone tumours
Now tell me about osteosarcoma