penetration of Meropenem in urine
Reading File
Finding Sources
Searching PubMed
meropenem urinary pharmacokinetics penetration
Searching the Web
meropenem urine penetration concentration pharmacokinetics renal excretion
Finding Sources
Finding Sources
Reading File
I now have comprehensive data from the FDA label, drug references, and textbooks. Here is a full, detailed answer:
Meropenem Urinary Penetration - Detailed Pharmacokinetics
Route of Elimination
Meropenem is primarily eliminated by the kidneys. Two mechanisms are involved:
- Glomerular filtration - passive filtration of unbound drug (protein binding is only ~2%, so virtually all circulating meropenem is free and filterable)
- Active tubular secretion - via OAT1 and OAT3 transporters in the proximal tubule (demonstrated by the fact that probenecid, an OAT inhibitor, increases meropenem AUC by ~56% and half-life by ~38%)
Urinary Recovery
| Fraction | Amount |
|---|---|
| Unchanged meropenem in urine (12 h) | ~70% (range 50-75%) |
| Microbiologically inactive ring-opened metabolite | ~28% |
| Fecal elimination | ~2% |
Total renal excretion accounts for ~98% of the administered dose.
Urinary Concentrations
After a 500 mg IV dose, peak urinary meropenem concentrations reach approximately 23 mcg/mL (range 14-26 mcg/mL). Critically, urine concentrations >10 mcg/mL are maintained for up to 5 hours after this dose. After a 1 g IV dose, peak urine concentrations rise to approximately 49 mcg/mL (range 39-58 mcg/mL).
These concentrations vastly exceed the MIC90 for most common uropathogens (e.g., E. coli, Klebsiella, Proteus - typically 0.016-0.5 mcg/mL for carbapenem-susceptible strains), making urine penetration clinically more than adequate.
Contrast with Imipenem
An important distinction: imipenem is rapidly hydrolyzed by renal tubular dehydropeptidase-1 (DHP-1), which degrades it in the renal tubule and significantly reduces its active urine concentrations. This is why imipenem must be co-administered with cilastatin (a DHP-1 inhibitor) to restore adequate urine levels. Meropenem, doripenem, and ertapenem are not significantly degraded by DHP-1 and therefore achieve high urinary concentrations without any inhibitor - an inherent pharmacokinetic advantage.
- Sherris & Ryan's Medical Microbiology, 8th Ed., p. 915
Renal Impairment
Because meropenem is so dependent on renal clearance, dose adjustment is required in renal impairment:
| CrCl (mL/min) | Half-life | Adjustment |
|---|---|---|
| >50 (normal) | ~1 hour | Standard dosing |
| 26-50 | ~1.9-3.3 h | Reduce dose or extend interval |
| 10-25 | ~3.8-5.7 h | Significant reduction required |
| <10 (or dialysis) | Markedly prolonged | Major dose reduction; supplement after HD |
In patients with reduced GFR, urinary concentrations will also be lower due to decreased filtration, but systemic concentrations rise - dosing is adjusted to avoid toxicity, not to compensate for reduced urinary penetration.
Drug Interaction Note
Co-administration with probenecid blocks tubular secretion, increasing systemic exposure by 56%. This combination is not recommended; it does not improve urinary concentrations (in fact, it reduces renal clearance and thus urinary delivery).
Clinical Implications
Meropenem's excellent urinary penetration makes it highly effective for:
- Complicated UTIs caused by ESBL-producing organisms
- Carbapenem-susceptible Pseudomonas aeruginosa UTIs
- Multidrug-resistant Enterobacterales urinary infections
The standard IV dose of 1 g q8h (or 500 mg q6h for uncomplicated UTI in some protocols) provides urine concentrations many times above the MIC for susceptible organisms throughout the dosing interval.
Sources: FDA MERREM IV Prescribing Information; Pfizer Meropenem Labeling; Sherris & Ryan's Medical Microbiology, 8th Ed.
blood supply of the heart
Reading File
Finding Sources
Searching the Web
blood supply of the heart coronary arteries anatomy branches territories
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have excellent textbook content and diagrams. Let me compile the full answer.
Blood Supply of the Heart
Arterial Supply - Overview
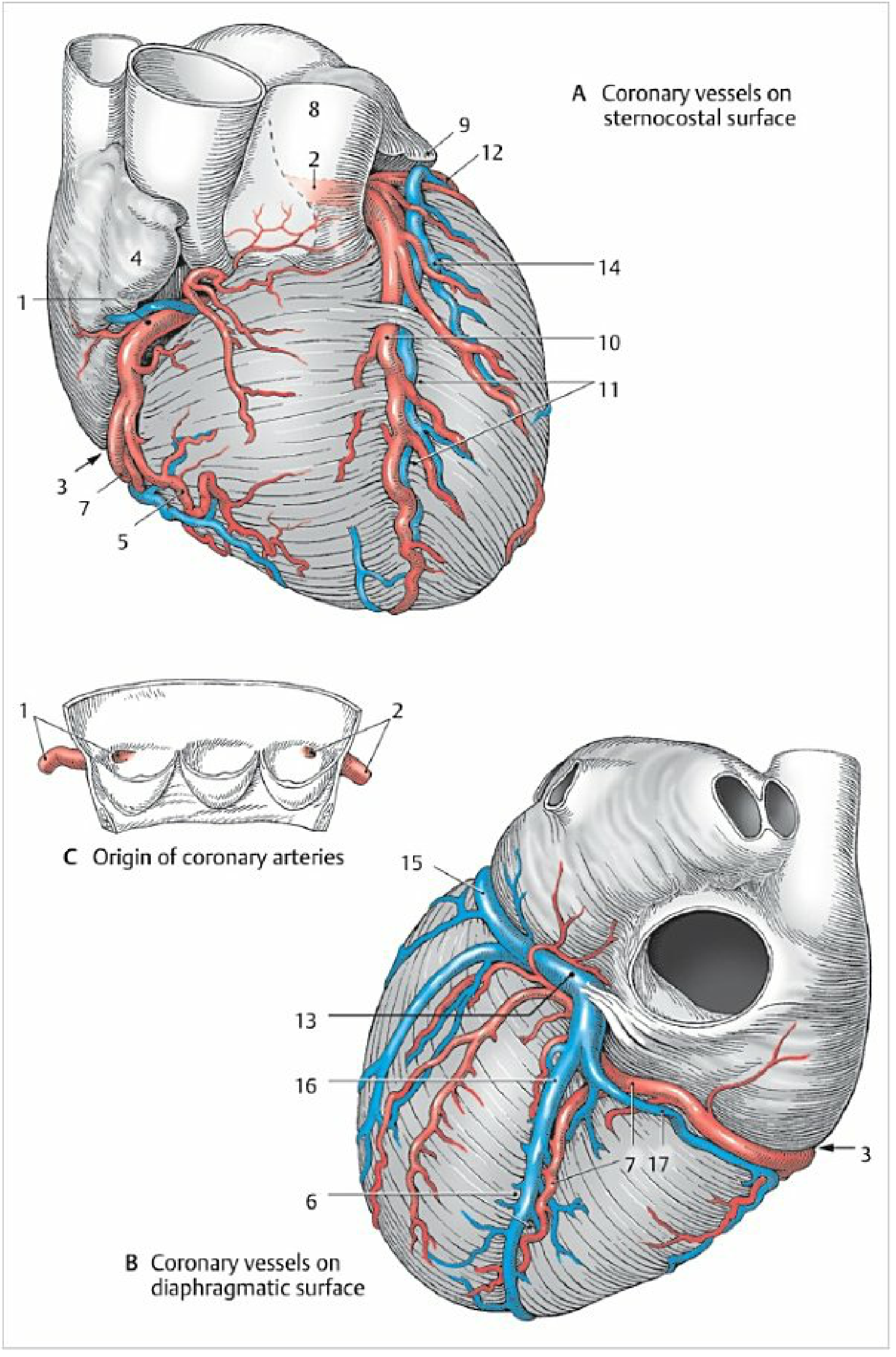
The heart is supplied by two coronary arteries - the right coronary artery (RCA) and the left coronary artery (LCA) - which arise from the aortic sinuses (behind the right and left cusps of the aortic valve) at the root of the ascending aorta. They run in the subepicardial fat within the coronary sulci and are the first branches off the aorta.
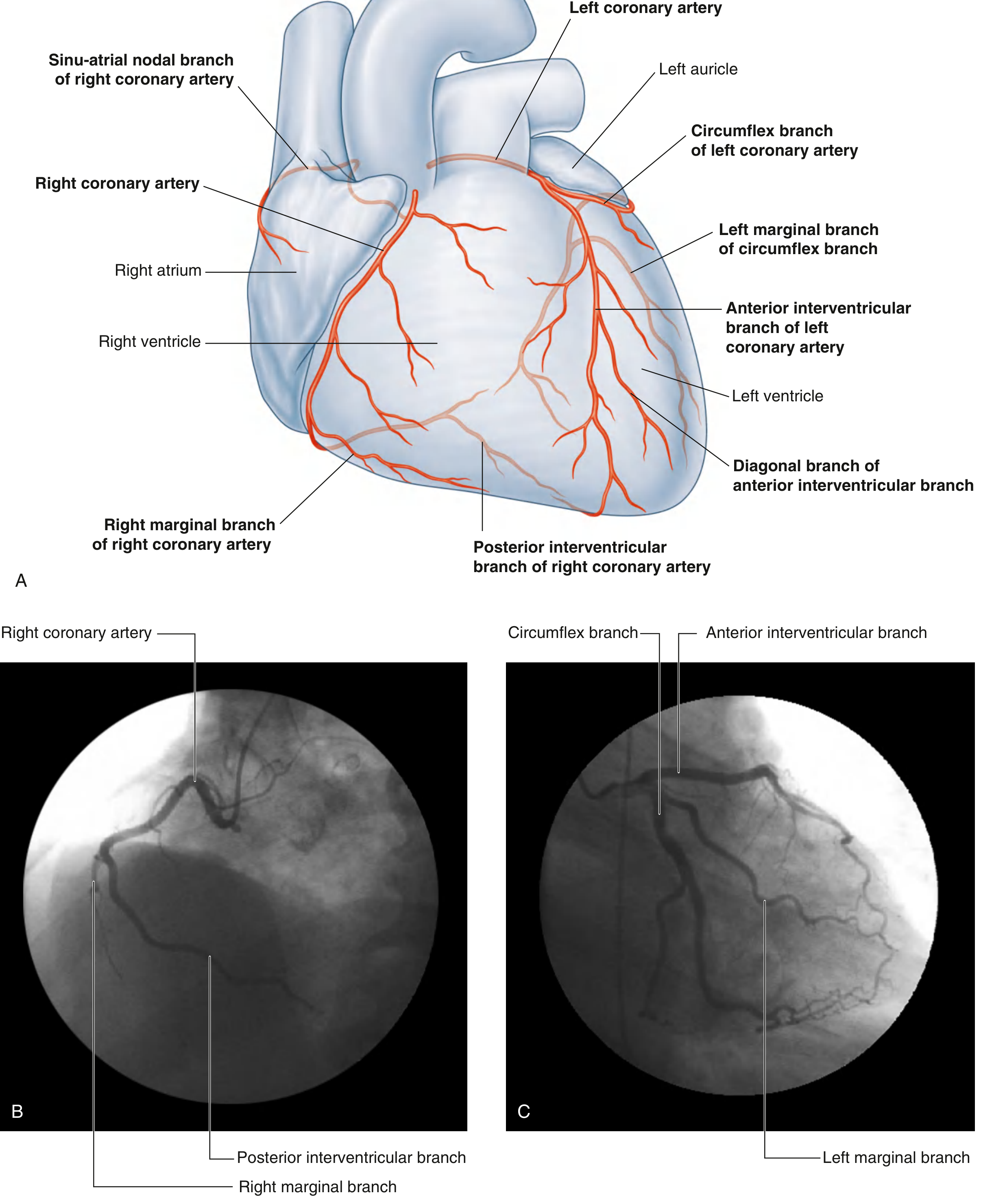
Right Coronary Artery (RCA)
- Arises from the right aortic sinus
- Initially covered by the right auricle as it enters the coronary sulcus on the right side
- Travels posteriorly in the coronary sulcus toward the posterior interventricular sulcus
Major branches:
| Branch | Course & Territory |
|---|---|
| Right marginal artery | Runs along the acute (right) margin toward the apex |
| Sinu-atrial (SA) nodal branch | Supplies the SA node (in ~60% of people) |
| AV nodal branch | Supplies the AV node before giving off the posterior interventricular artery |
| Posterior interventricular artery (PDA) | Descends in the posterior interventricular sulcus toward the apex |
Territory supplied:
- Right atrium and right ventricle
- SA node and AV node (in most people)
- Interatrial septum and a portion of the left atrium
- Posteroinferior one-third of the interventricular septum
- A portion of the posterior wall of the left ventricle
Left Coronary Artery (LCA)
- Arises from the left aortic sinus
- A short trunk (the "left main stem") passes between the pulmonary trunk and the left auricle before dividing into its two terminal branches
Two terminal branches:
1. Anterior Interventricular Artery (LAD - Left Anterior Descending)
- Descends in the anterior interventricular sulcus toward the apex
- Gives off diagonal branches that cross the anterior surface of the left ventricle
- Gives off septal perforators that penetrate the interventricular septum
- Supplies the anterior wall of the left ventricle, the anterior two-thirds of the interventricular septum, and the apex
2. Circumflex Artery (Cx)
- Courses posteriorly in the coronary sulcus along the left border
- Gives off the left marginal artery (obtuse marginal), which runs along the left/obtuse border
- Usually ends before reaching the posterior interventricular sulcus (in right-dominant hearts)
- Supplies the left atrium and the lateral/posterior wall of the left ventricle
Overall LCA territory: Most of the left atrium, most of the left ventricle, the anterior two-thirds of the interventricular septum including the bundle of His and bundle branches.
Coronary Dominance
"Dominance" refers to which artery gives rise to the posterior descending artery (PDA) and therefore supplies the posteroinferior left ventricle:
| Dominance | Frequency | PDA Origin |
|---|---|---|
| Right dominant | ~80-85% | RCA |
| Left dominant | ~10-15% | Circumflex branch of LCA |
| Balanced/co-dominant | ~5% | Both contribute |
In right-dominant hearts, the RCA is the larger posterior vessel. In left-dominant hearts, the circumflex is enlarged and provides the PDA. This is also important for SA/AV node supply - occasionally the circumflex provides the nodal arteries instead of the RCA.
Venous Drainage
About two-thirds of venous return from the heart drains into the coronary sinus, which lies in the posterior part of the coronary sulcus and opens into the right atrium:
| Vein | Drainage area |
|---|---|
| Great cardiac vein (becomes the anterior interventricular vein) | Anterior interventricular sulcus → left coronary sulcus → coronary sinus |
| Middle cardiac vein | Posterior interventricular sulcus → coronary sinus |
| Small cardiac vein | Right side of heart → coronary sinus |
The remaining one-third drains via:
- Anterior cardiac veins - drain the right ventricle directly into the right atrium
- Thebesian veins (smallest cardiac veins) - tiny veins that empty directly into the cardiac chambers
Lymphatic Drainage
The heart has a deep endocardial, middle myocardial, and superficial epicardial lymphatic network. Collecting vessels travel with the great vessels toward the tracheobronchial and anterior mediastinal lymph nodes.
Clinical Correlates
| Vessel occluded | Area of infarction | ECG changes |
|---|---|---|
| LAD | Anterior LV wall + anterior septum | Anterior leads (V1-V4) |
| RCA | Inferior LV wall + RV | Inferior leads (II, III, aVF) |
| Circumflex | Lateral LV wall | Lateral leads (I, aVL, V5-V6) |
Coronary arteries are functional end arteries - their small anastomoses are insufficient to develop adequate collateral circulation if acute occlusion occurs, explaining why myocardial infarction results from coronary thrombosis (>90% of cases on a ruptured atherosclerotic plaque).
- Gray's Anatomy for Students, p. 239-242
- Color Atlas of Human Anatomy Vol. 2, p. 58-59
- Netter's Atlas of Human Anatomy, p. 354-360
This is a shared conversation. Sign in to Orris to start your own chat.