Explain me menstrual cycle
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
I now have more than enough comprehensive content from authoritative textbooks. Let me compile the full, detailed answer.
The Menstrual Cycle
The menstrual cycle is the monthly series of hormonal and structural changes that prepares a woman's body for potential pregnancy. In humans and other primates, its most visible feature is periodic vaginal bleeding (menstruation) from shedding of the uterine lining. The average cycle length is 28 days, counted from the first day of one period to the first day of the next, though this is notoriously variable between individuals.
The cycle is orchestrated by a four-level axis: Hypothalamus → Anterior Pituitary → Ovaries → Uterus (endometrium).
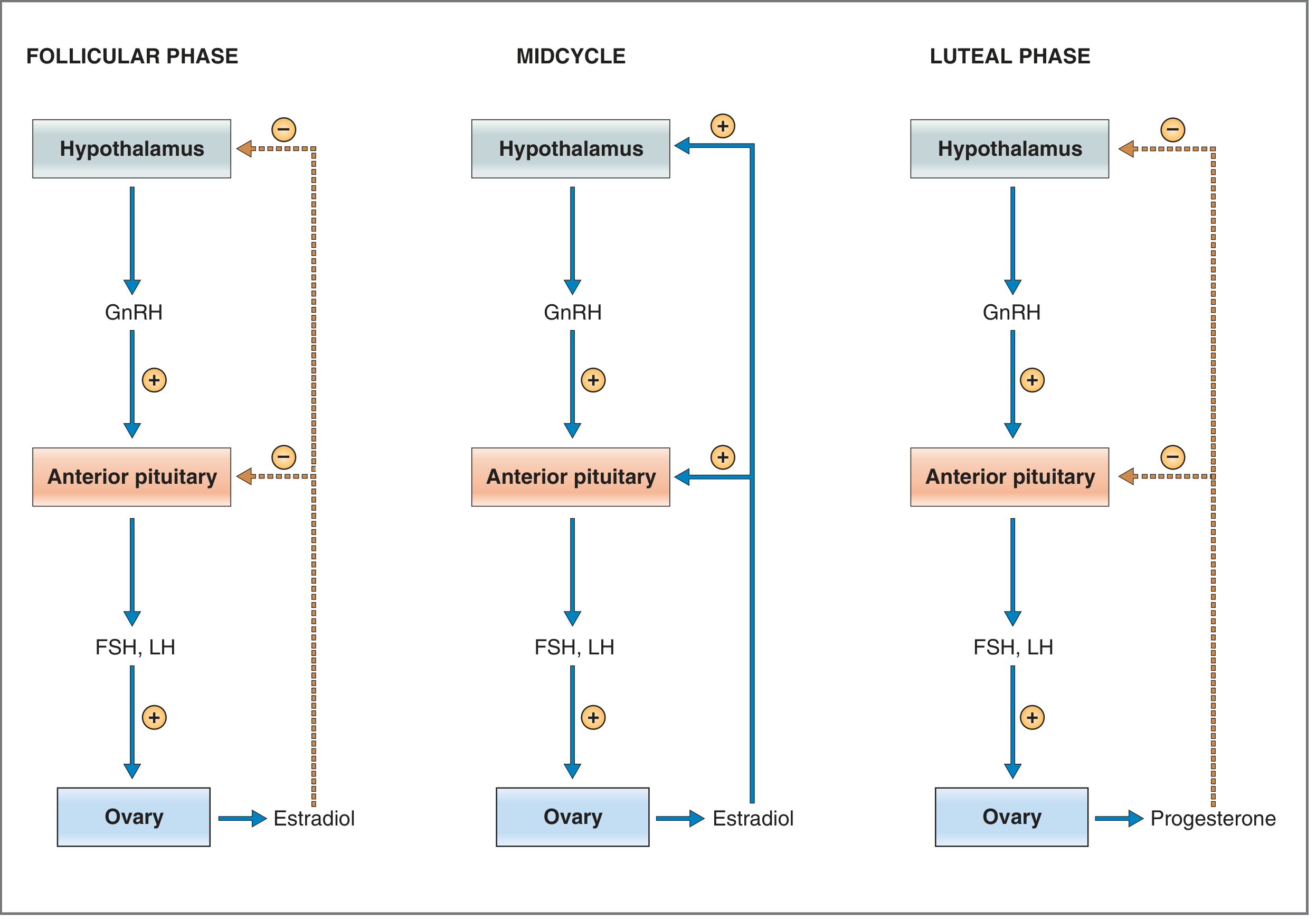
Hormonal Control Axis
Hypothalamus releases GnRH (Gonadotropin-Releasing Hormone) in pulses into the portal circulation. GnRH pulse frequency determines the relative ratio of FSH to LH secreted by the pituitary - higher frequency favors LH, lower frequency favors FSH.
Anterior Pituitary releases two gonadotropins in response:
- FSH (Follicle-Stimulating Hormone) - acts on granulosa cells of ovarian follicles; stimulates their growth and estradiol synthesis
- LH (Luteinizing Hormone) - triggers ovulation and drives corpus luteum formation and function
Ovaries respond by producing estradiol (follicular phase) and progesterone + estradiol (luteal phase), which then feed back on the hypothalamus and pituitary.
Phases of the Menstrual Cycle
The 28-day cycle has four overlapping phases:
1. Menstrual Phase (Days 1-5)
This is day 1 of the new cycle. In the absence of fertilization, the corpus luteum regresses at the end of the previous cycle, causing an abrupt fall in estrogen and progesterone. This withdrawal causes the decidua functionalis (functional layer of the endometrium) to shed, producing menstrual bleeding lasting 4-5 days. Meanwhile, new primordial follicles begin to be recruited for the next cycle.
2. Follicular Phase / Proliferative Phase (Days 1-14)
This phase runs concurrently with and following menstruation, lasting until ovulation.
Ovarian events:
- At the start of the cycle, several primordial follicles are recruited and begin to enlarge, forming an antrum (fluid-filled cavity) around the oocyte
- Around day 6, one follicle emerges as the dominant (Graafian) follicle, while the rest undergo apoptotic atresia
- The dominant follicle is selected based on its superior ability to produce intrafollicular estrogen needed for final maturation
- Granulosa cells (driven by FSH) and theca interna cells work together: theca cells secrete androgens, which granulosa cells aromatize into estradiol - this is the two-cell, two-gonadotropin model
- As estradiol rises, it initially exerts negative feedback on the hypothalamus and pituitary, suppressing FSH and LH
Endometrial events (Proliferative Phase):
- After menstruation, the endometrium is thin (1-2 mm), composed of the basalis layer
- Rising estradiol drives mitotic growth of the decidua functionalis
- Initially straight, narrow glands elongate and become tortuous; histologically, cells go from low columnar to pseudostratified pattern
- Stroma is dense and compact, with increased vascular development
- Cervical mucus becomes copious, watery, elastic, and forms a "ferning" pattern on a slide - creating channels that allow sperm penetration
3. Ovulation (Day ~14)
This is the pivotal event of the cycle triggered by a critical rise in estradiol:
- When estradiol reaches a threshold of ≥200 pg/mL for a sustained period, feedback switches from negative to positive - estradiol now up-regulates GnRH receptors in the anterior pituitary
- This triggers the dramatic LH surge (and a smaller FSH surge), called the ovulatory surge
- The LH surge causes rupture of the dominant follicle approximately 36 hours after its onset, releasing the mature oocyte into the peritoneal cavity
- The oocyte is picked up by the fimbriated ends of the fallopian tube
- Minor bleeding from the ruptured follicle into the peritoneal cavity can cause transient lower abdominal pain known as Mittelschmerz
Below is the feedback control diagram across the three phases:
4. Luteal Phase / Secretory Phase (Days 14-28)
Ovarian events:
- After rupture, the follicle fills with blood (corpus hemorrhagicum), then granulosa and theca cells rapidly proliferate and become lipid-rich luteal cells, forming the corpus luteum (yellow body)
- The corpus luteum secretes both progesterone (dominant) and estradiol
- Its development and maintenance depend on adequate vascular supply (VEGF plays a role)
- Progesterone and estradiol from the corpus luteum exert negative feedback on the hypothalamus and pituitary, suppressing further gonadotropin release and preventing development of new follicles
- If fertilization does NOT occur, the corpus luteum regresses around days 24-26, causing progesterone and estradiol levels to plummet - triggering the next menstruation
- If fertilization DOES occur, trophoblastic cells of the early embryo secrete hCG (human chorionic gonadotropin), which "rescues" the corpus luteum and maintains steroid production until the placenta takes over (~weeks 8-10)
Endometrial events (Secretory Phase):
- Within 48-72 hours of ovulation, progesterone transforms the endometrium into a secretory state
- Glands form characteristic PAS-positive, glycogen-filled subnuclear vacuoles that progressively migrate to the glandular lumen, with maximal secretory activity at postovulatory day 6-7 - precisely when a blastocyst would be arriving for implantation
- The stroma becomes edematous; spiral arteries elongate and coil
- By day 24, a perivascular eosinophilic pattern ("cuffing") appears, marking the beginning of decidualization
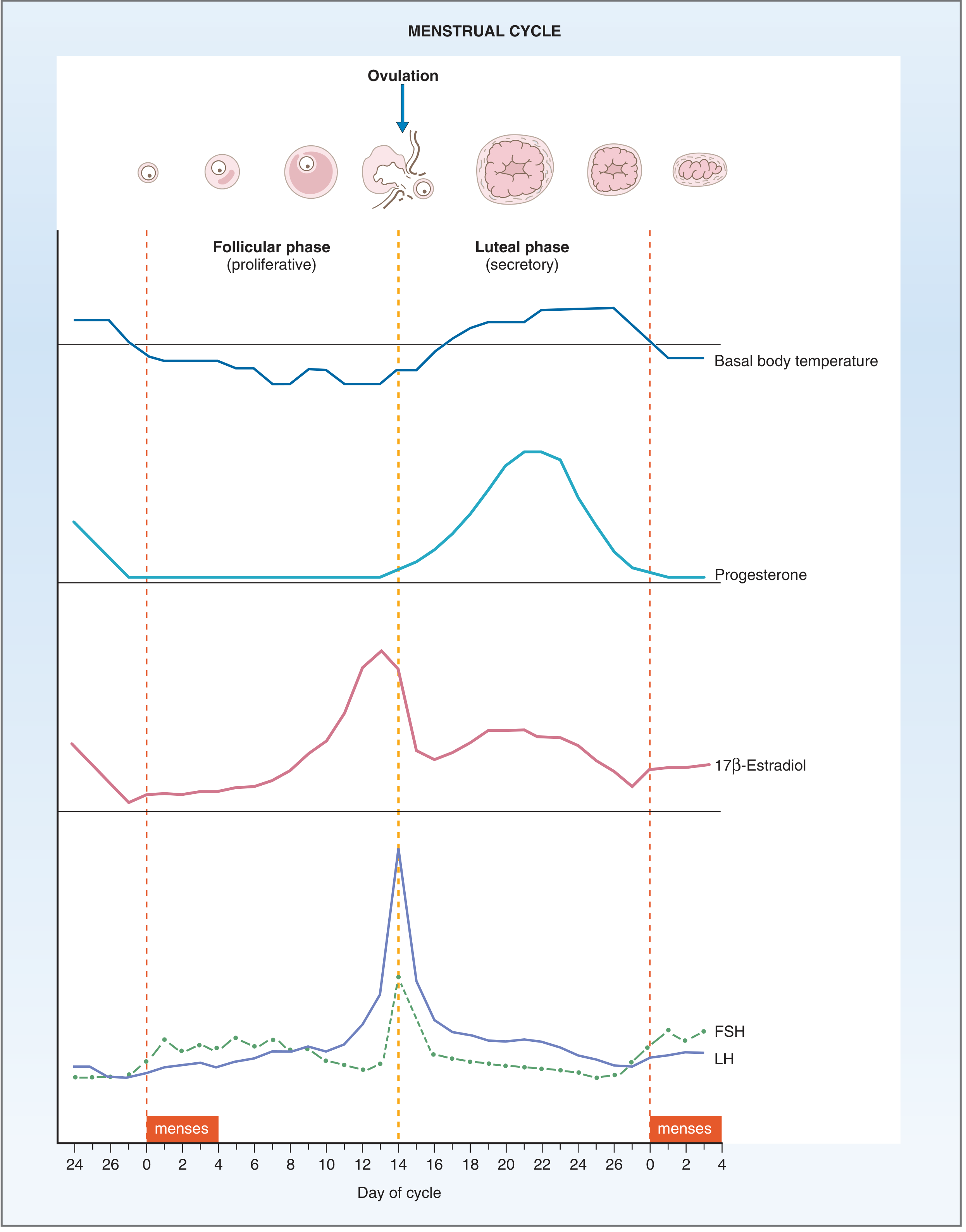
- Basal body temperature rises ~0.3-0.5°C during the luteal phase due to progesterone's effect on the hypothalamic temperature set point
- Cervical mucus becomes thick, scant, and non-elastic - no longer ferning - because sperm penetration is no longer needed
Here is the full hormone curve diagram showing all changes over a 28-day cycle:
Summary Table
| Feature | Follicular/Proliferative Phase (Days 1-14) | Luteal/Secretory Phase (Days 14-28) |
|---|---|---|
| Dominant hormone | Estradiol | Progesterone |
| Ovary | Follicle development, estradiol rises | Corpus luteum, progesterone + estradiol |
| Feedback | Negative (early) → Positive (midcycle LH surge) | Negative |
| Endometrium | Proliferation, gland elongation | Secretory, glycogen vacuoles, edema |
| Cervical mucus | Watery, elastic, ferning, sperm-permeable | Thick, scant, non-ferning |
| Basal body temp | Slightly lower | Rises (~0.3-0.5°C) after ovulation |
| Key event | Follicle selection and growth | Corpus luteum formation and regression |
Key Hormonal Events at a Glance
- Day 1: Menses begins; estrogen and progesterone are at their lowest
- Days 1-13: FSH drives follicle growth → rising estradiol
- Day ~12-13: Estradiol exceeds ~200 pg/mL → switches to positive feedback → LH surge
- Day 14: Ovulation (LH surge peaks ~36 hours before)
- Days 14-28: Corpus luteum produces progesterone → secretory endometrium
- Day ~24-26: Corpus luteum regresses if no pregnancy → estrogen + progesterone drop → menses
What Happens If Pregnancy Occurs?
The fertilized egg travels down the fallopian tube and reaches the uterine cavity as a blastocyst approximately 4 days after ovulation. Implantation occurs around postovulatory day 6-7. The trophoblastic cells of the implanting embryo begin secreting hCG, which mimics LH and prevents corpus luteum regression. This maintains progesterone and estrogen levels, preventing menstruation and sustaining the endometrium for the developing embryo. By the second trimester, the placenta takes over steroid hormone production entirely.
Sources: Costanzo Physiology 7th Edition, pp. 477-481; Berek & Novak's Gynecology, pp. 264-285; Ganong's Review of Medical Physiology 26th Edition, pp. 403-404
This is a shared conversation. Sign in to Orris to start your own chat.