Management of IgG4 disease
Reading File
Finding Sources
Searching PubMed
"IgG4-related disease" AND management
Searching the Web
IgG4-related disease management treatment guidelines 2024 2025
Reading File
Reading File
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC12525221
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from Harrison's 22E (2025), Yamada's Gastroenterology, Robbins Pathology, and recent PMC 2025 literature. Let me compile the full answer.
Management of IgG4-Related Disease (IgG4-RD)
Background
IgG4-RD is a systemic fibro-inflammatory disorder characterized by tissue infiltrates dominated by IgG4-positive plasma cells, storiform fibrosis, obliterative phlebitis, and usually elevated serum IgG4. It can affect virtually any organ - pancreas, bile ducts, salivary glands, lacrimal glands, kidneys, lungs, retroperitoneum, meninges, aorta, thyroid, and more. It most often affects middle-aged to older males, though salivary/lacrimal gland disease shows a more equal sex distribution.
The hallmark histology (shown below from Harrison's 22E) demonstrates dense lymphoplasmacytic infiltrate, storiform fibrosis, and obliterative phlebitis:
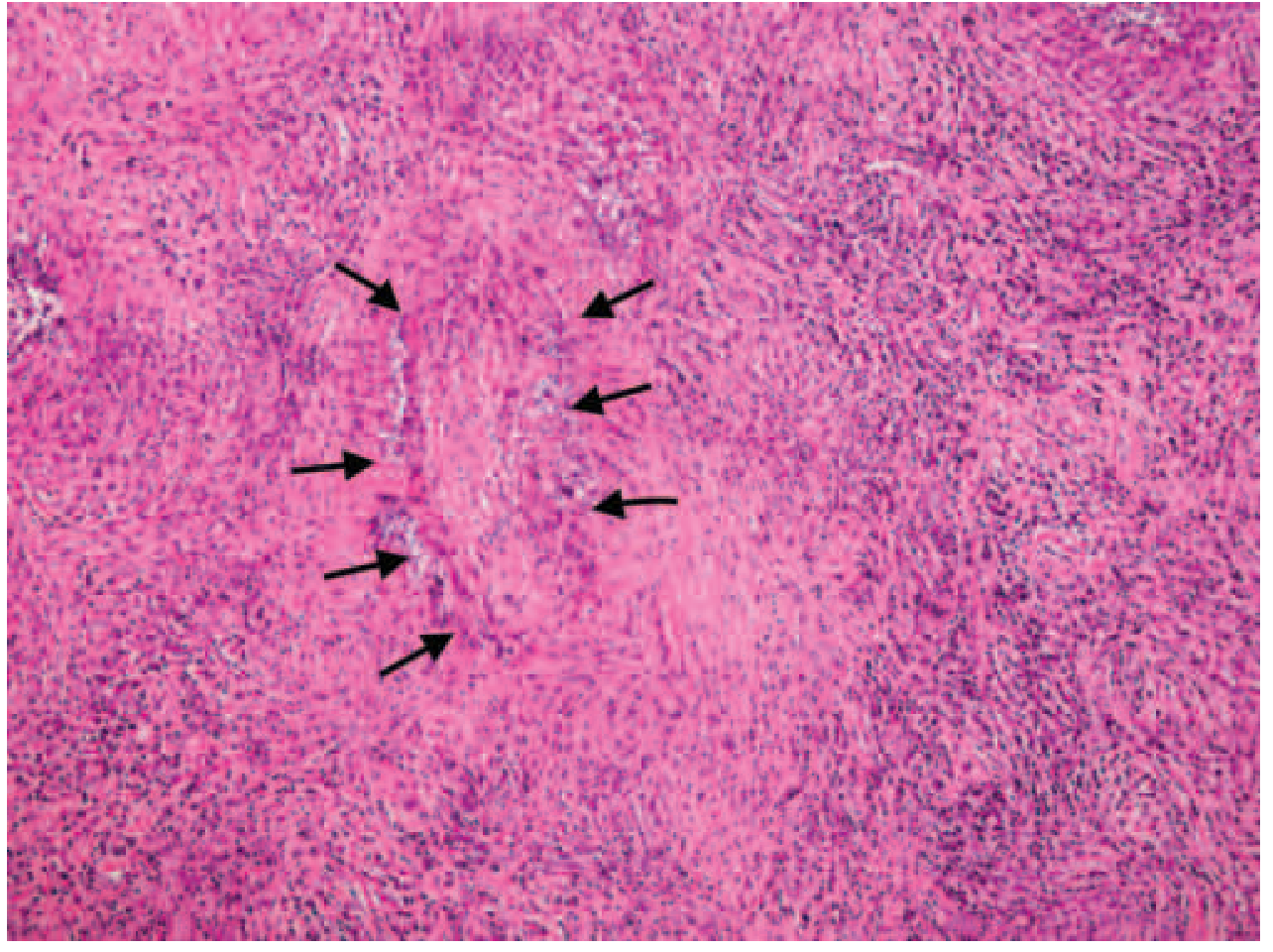
Harrison's 22E (2025): Storiform fibrosis and obliterative phlebitis in IgG4-RD from a patient with hypertrophic pachymeningitis - identical findings occur in pancreas, kidneys, salivary glands, and other organs.
Before Treating: Pre-requisites
1. Confirm the diagnosis
Biopsy from an affected organ is strongly recommended whenever feasible - not just to confirm IgG4-RD but to exclude malignancy (adenocarcinoma, lymphoma), infection, vasculitis (GPA, MPA), sarcoidosis, Castleman disease, and primary sclerosing cholangitis, all of which are important mimics. Histopathology must always be interpreted in the clinical, serological, and radiological context - pathology alone is never sufficient.
2. Do not rely on serum IgG4 alone
Serum IgG4 is supportive but not diagnostic - it can be elevated in many conditions and is normal in ~30-40% of biopsy-confirmed cases. Normalization of serum IgG4 is not required to declare remission.
3. Assess for organ-threatening involvement
Some manifestations require urgent treatment: IgG4-RD can lead quickly to end-stage liver disease, permanent pancreatic insufficiency, renal atrophy, aortic dissection/aneurysm, and destructive sinonasal lesions.
Treatment Indications
- Active, symptomatic disease (obstructive jaundice, abdominal pain, organ swelling, visual change, renal dysfunction) should be treated promptly.
- Asymptomatic patients may be observed ("watchful waiting") with monitoring, particularly for IgG4-related lymphadenopathy.
- Watchful waiting requires active surveillance, because serious organ involvement can evolve over time, especially with rising serum IgG4.
Induction of Remission
First-line: Glucocorticoids
Glucocorticoids are the standard first-line treatment for induction of remission. The clinical response is typically swift and striking.
| Regimen | Detail |
|---|---|
| Starting dose | Prednisone 30-40 mg/day (or 0.6-1 mg/kg/day) |
| Duration of high-dose | 2-4 weeks |
| Taper | To 5 mg/day (or discontinuation) over 2-3 months |
| Minimum effective dose | At least 20 mg/day needed to induce remission |
Most patients respond dramatically within 2-4 weeks. Non-response should raise suspicion of an alternative diagnosis, most importantly malignancy.
Important caveat: Prolonged steroid-free remissions are uncommon. The risk of glucocorticoid-induced morbidity is high in this predominantly middle-aged to elderly population, particularly those with pre-existing comorbidities and pancreatic involvement.
Maintenance of Remission
Maintenance therapy is not required for every patient but should be considered for:
- Remarkably high serum IgG4 before treatment
- Still elevated serum IgG4 after steroid induction
- Diffuse pancreatic enlargement
- Proximal IgG4-sclerosing cholangitis (high risk of cirrhosis)
- More than two organs involved
- Prior disease relapse
Maintenance options:
- Low-dose steroids (2.5-5 mg/day) for up to 3 years - supported by Japanese guidelines and an RCT by Masamune et al. showing 76.7% long-term remission rate.
- Conventional steroid-sparing immunomodulators (azathioprine, mycophenolate mofetil) - experience is limited and evidence of superiority over steroids alone is lacking; one study showed relapse-free survival was similar to steroids alone, and 22% had treatment-related side effects requiring discontinuation.
- Rituximab (see below) as maintenance every 2-3 months.
Second-line and Steroid-Sparing Therapy
Rituximab (Anti-CD20 B-cell Depletion)
Rituximab is the established second-line agent for:
- Relapsing disease
- Glucocorticoid-resistant disease
- Patients at high risk for glucocorticoid toxicity
Regimen: Two doses of 1 g IV, separated by ~15 days (rheumatology protocol); alternatively 375 mg/m² x4 weekly.
Evidence:
- Leads to swift decline in serum IgG4 concentrations by preventing repletion of short-lived IgG4-producing plasma cells.
- Also depletes CD4+ cytotoxic T cells that mediate profibrotic injury.
- In pancreaticobiliary IgG4-RD: 86% complete/partial remission at 6 months; 89% in remission at 3 years with induction + maintenance rituximab (Majumder et al.).
- Rituximab maintenance (every 2-3 months infusion) reduces relapse rates.
(Harrison's Principles of Internal Medicine 22E, 2025)
Novel Targeted Therapy (2025 Update)
Inebilizumab (Uplizna) - FDA Approved April 2025
Inebilizumab is the first FDA-approved treatment specifically for IgG4-RD (April 2025). It is an anti-CD19 monoclonal antibody that depletes B cells via antibody-dependent cellular cytotoxicity - with a broader effect than rituximab (targeting CD19 extends to B-cell precursors).
MITIGATE Trial (Phase 3):
- 135 patients with active IgG4-RD randomized 1:1 to inebilizumab 300 mg IV (Days 1, 15, and Week 26) vs. placebo over 52 weeks.
- All patients had to taper off glucocorticoids by Week 8.
- Cumulative glucocorticoid dose: 188 mg (inebilizumab arm) vs. 1,385 mg (placebo arm).
- Glucocorticoid withdrawal achieved: 90% (inebilizumab) vs. 37% (placebo).
- Significantly fewer relapses in the inebilizumab group.
- Adverse events: 18% (inebilizumab) vs. 9% (placebo) - warrants careful long-term safety monitoring.
Note: No head-to-head trial with rituximab exists yet, and long-term real-world data are lacking.
Management of Relapse
Relapse rates in IgG4-RD range from 15-60%, with proximal biliary tract disease being the strongest risk factor. Relapses can occur in the same or different organs from the initial presentation.
Options for relapse management:
- Tapering course of high-dose steroids alone (without maintenance) - for low-relapse-risk patients.
- Tapering course of high-dose steroids + maintenance therapy (low-dose steroid or immunomodulator).
- Rituximab induction alone, then clinical follow-up.
- Rituximab induction + rituximab maintenance (infusion every 2-3 months).
After relapse, escalation to steroid-sparing therapy (rituximab or inebilizumab) should be strongly considered, especially for patients whose disease is steroid-responsive but not steroid-sustainable.
Organ-Specific Considerations
| Organ/Manifestation | Specific Management Notes |
|---|---|
| Obstructive jaundice | Biliary stenting + antibiotics first if cholangitis present, then initiate steroids once stabilized |
| IgG4-related sclerosing cholangitis (proximal) | High relapse/cirrhosis risk - favor maintenance therapy |
| Retroperitoneal fibrosis | May have incomplete radiographic response (fibrosis may persist despite clinical remission) |
| Intrahepatic bile ducts | Less complete response to steroids; fibrotic damage may persist |
| Pancreatic exocrine insufficiency | Pancreatic enzyme replacement for persistent steatorrhea; up to 50% need insulin/oral agents for DM |
| Aortic involvement | Treat aggressively - risk of dissection/aneurysm |
| Renal involvement | Steroid-responsive; risk of renal atrophy with delayed treatment |
| Lymphadenopathy | Often responds to steroids; watchful waiting acceptable if asymptomatic |
Monitoring During and After Treatment
Monitoring should never rely on a single measure. Use a combination of:
- Symptoms and clinical examination
- Laboratory trends (serum IgG4, organ-specific enzymes - liver, renal function)
- Imaging (CT/MRI/PET)
- Organ-specific assessment (spirometry for lung, creatinine for kidney, etc.)
Serum IgG4 may remain elevated even in clinical remission - normalization is not required as a treatment endpoint. However, persistently rising IgG4 during observation warrants closer vigilance.
Management Algorithm Summary
Active, symptomatic IgG4-RD
│
▼
Glucocorticoids (prednisone 30-40 mg/day → taper over 2-3 months)
│
┌────┴─────┐
Remission No response → reconsider diagnosis (malignancy?)
│
Assess relapse risk
│
Low risk: Observe / discontinue
High risk: Maintenance (low-dose steroids OR rituximab)
│
Relapse → Re-induce (steroids) + escalate to rituximab / inebilizumab
Key References
- Harrison's Principles of Internal Medicine, 22nd Edition (2025), Chapter 380 - IgG4-Related Disease Treatment
- Yamada's Textbook of Gastroenterology, 7th Edition - AIP/IgG4-RD Management
- Robbins & Kumar Pathologic Basis of Disease - IgG4-RD Pathology
- PMC 2025: "New Developments in the Treatment of IgG4-Related Disease" (full article)
- IgG4Ward Official Management Guidelines (igg4ward.org)
2025 Update Notice: Inebilizumab (Uplizna) received FDA approval in April 2025 as the first targeted therapy for IgG4-RD. Rituximab remains well-established off-label. BTK inhibitors (e.g., rilzabrutinib) are in early-phase trials as future options. (PMID: 38769126)
Skyrizi dosing in psa
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.