Teach me pneumothorax with pics also
Reading File
Finding Sources
Searching the Web
pneumothorax types pathophysiology clinical features chest X-ray treatment 2025
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have all the images and content I need to write a comprehensive, well-illustrated lesson. Let me compile everything:
Pneumothorax - A Complete Guide with Images
Sources: Rosen's Emergency Medicine (9e), Goldman-Cecil Medicine, Roberts & Hedges' Clinical Procedures in Emergency Medicine, Murray & Nadel's Textbook of Respiratory Medicine
1. Definition
A pneumothorax is an abnormal collection of air in the pleural space - the potential space between the parietal pleura (lining the chest wall) and visceral pleura (covering the lung). This disrupts the negative intrapleural pressure that keeps the lung expanded, causing the ipsilateral lung to collapse.
2. Classification
A. Spontaneous Pneumothorax
Primary Spontaneous Pneumothorax (PSP)
- Occurs with no clinically apparent underlying lung disease
- Typical patient: tall, thin young male (3x more common in men)
- Caused by rupture of subpleural blebs - small thin-walled air pockets
- Risk factors: smoking, Marfan syndrome, mitral valve prolapse, changes in atmospheric pressure
- Incidence approximately 7.4/100,000/year in men; 1.2/100,000/year in women
Secondary Spontaneous Pneumothorax (SSP)
- Occurs on a background of existing lung disease
- Most common cause in the US: COPD (emphysematous bullae rupture)
- Other causes include:
- Asthma, cystic fibrosis
- Pneumocystis jirovecii pneumonia (HIV patients)
- Tuberculosis and lung abscess (developing countries)
- Connective tissue diseases (Marfan, Ehlers-Danlos)
- Malignancy, sarcoidosis, lymphangioleiomyomatosis
B. Traumatic Pneumothorax
- 15-50% of patients with significant chest trauma
- Three subtypes based on the relationship with the atmosphere:
1. Simple (Closed) Pneumothorax
- No communication with the atmosphere
- No mediastinal shift
- Usually caused by a rib fracture lacerating the pleura, or a blow at full inspiration with the glottis closed ("paper bag effect")
2. Communicating (Open) Pneumothorax - "Sucking Chest Wound"
- Chest wall defect creates a direct communication with the atmosphere
- Mostly from gunshot wounds or combat injuries
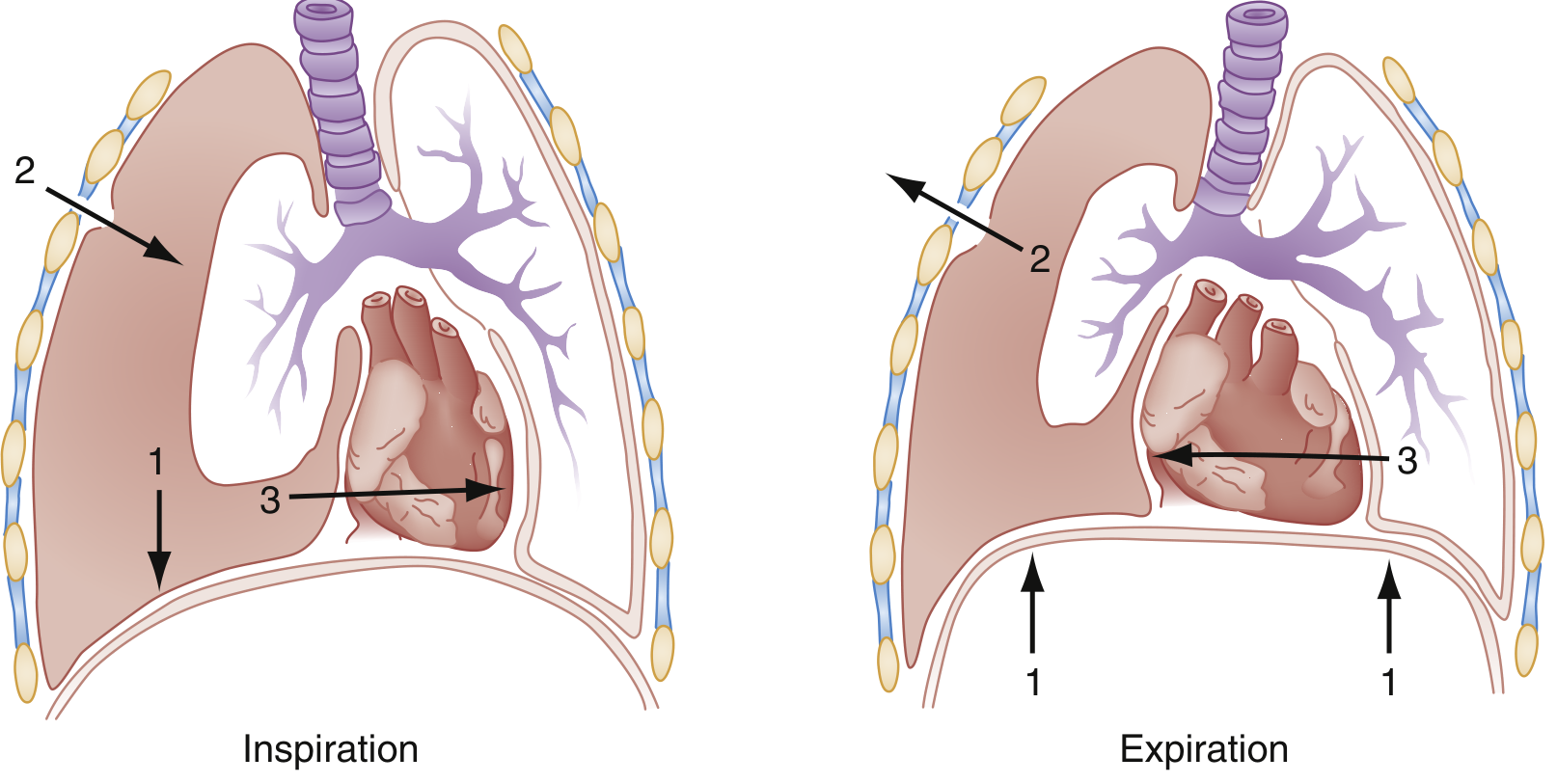
Inspiration (left): Diaphragm contracts (arrow 1) drawing air through the chest wound into the pleural cavity (arrow 2), shifting mediastinal structures to the opposite side (arrow 3). Expiration (right): Air exits the wound; the collapsed lung paradoxically expands slightly. This creates massive dead space and severe ventilatory disturbance.
3. Tension Pneumothorax
- A one-way valve effect - air enters on inspiration but cannot exit on expiration
- Air accumulates progressively under pressure, pushing the mediastinum to the opposite side
- Compresses the vena cava and distorts the cavoatrial junction - dramatically reduces venous return and cardiac output
- Life-threatening emergency
C. Iatrogenic Pneumothorax
- Complication of central line placement, thoracentesis, lung biopsy, mechanical ventilation (barotrauma), post-procedure
3. Pathophysiology
Normally, intrapleural pressure is slightly negative relative to atmospheric pressure (-3 to -5 cmH2O at rest), maintained by the elastic recoil of the lung pulling inward against the chest wall pulling outward.
When air enters the pleural space:
- Negative intrapleural pressure is lost
- The ipsilateral lung collapses (elastic recoil)
- Vital capacity and functional residual capacity drop
- Ventilation-perfusion mismatch causes hypoxemia
In tension pneumothorax, progressive air accumulation causes:
- Ipsilateral lung total collapse
- Mediastinal shift contralaterally
- Compression of contralateral lung
- Kinking and compression of the vena cava → decreased preload → shock
- Rapid onset of hypoxia, acidosis, cardiovascular collapse, and death if untreated
4. Clinical Features
Symptoms
| Feature | Detail |
|---|---|
| Chest pain | Sudden onset, pleuritic (sharp, worse with breathing) |
| Dyspnea | Can range from mild to severe |
| Cough | Dry, non-productive |
Signs on Examination
| Finding | Explanation |
|---|---|
| Decreased/absent breath sounds (ipsilateral) | Air in pleural space blocks transmission |
| Hyper-resonance on percussion (ipsilateral) | Air is more resonant than lung tissue |
| Reduced chest expansion (ipsilateral) | Lung collapsed |
| Tracheal deviation (away from side) | Only in tension - mediastinal shift |
| JVD (jugular venous distension) | Only in tension - obstructed venous return |
| Hypotension + tachycardia | Only in tension - cardiogenic shock |
| Subcutaneous emphysema | Air tracking into soft tissues |
Tension Pneumothorax - The Classic Triad
Tracheal deviation + absent breath sounds (ipsilateral) + hypotension = Tension pneumothorax until proven otherwise. Treat first, confirm later.
5. Imaging
Chest X-Ray
The first-line investigation. Request upright, full-inspiratory PA film when possible.
CXR findings:
- Visible visceral pleural line (thin white line parallel to chest wall) with no lung markings beyond it
- Collapsed lung toward the hilum
- If tension: tracheal deviation, depressed ipsilateral hemidiaphragm, contralateral mediastinal shift
CXR 1: Right-sided simple pneumothorax from penetrating trauma (bullet visible near right mediastinum)
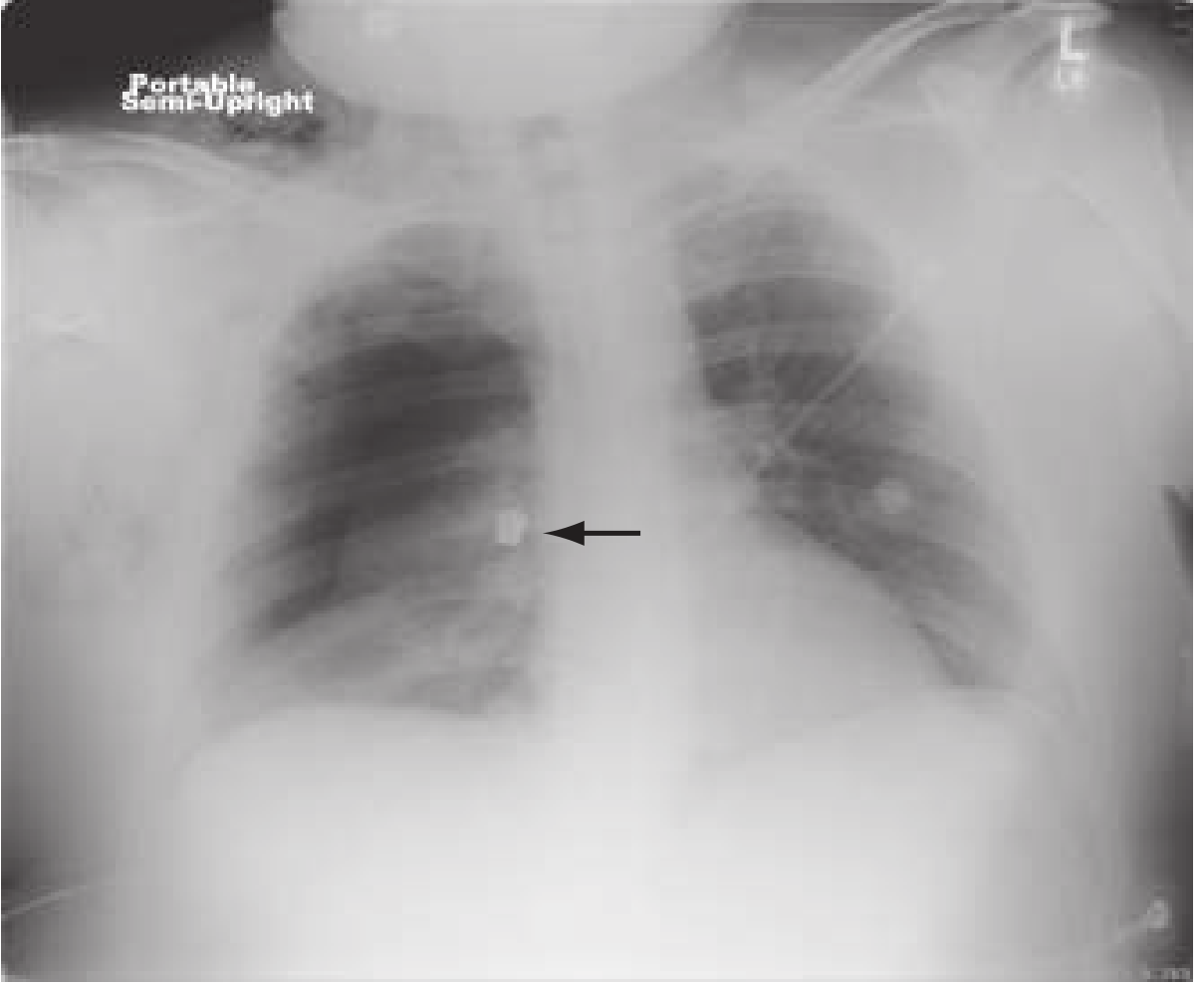
Note the right lung is hyperlucent and partially collapsed. A bullet fragment is visible near the right mediastinum (arrow).
CXR 2: Left-sided tension pneumothorax in an intubated patient
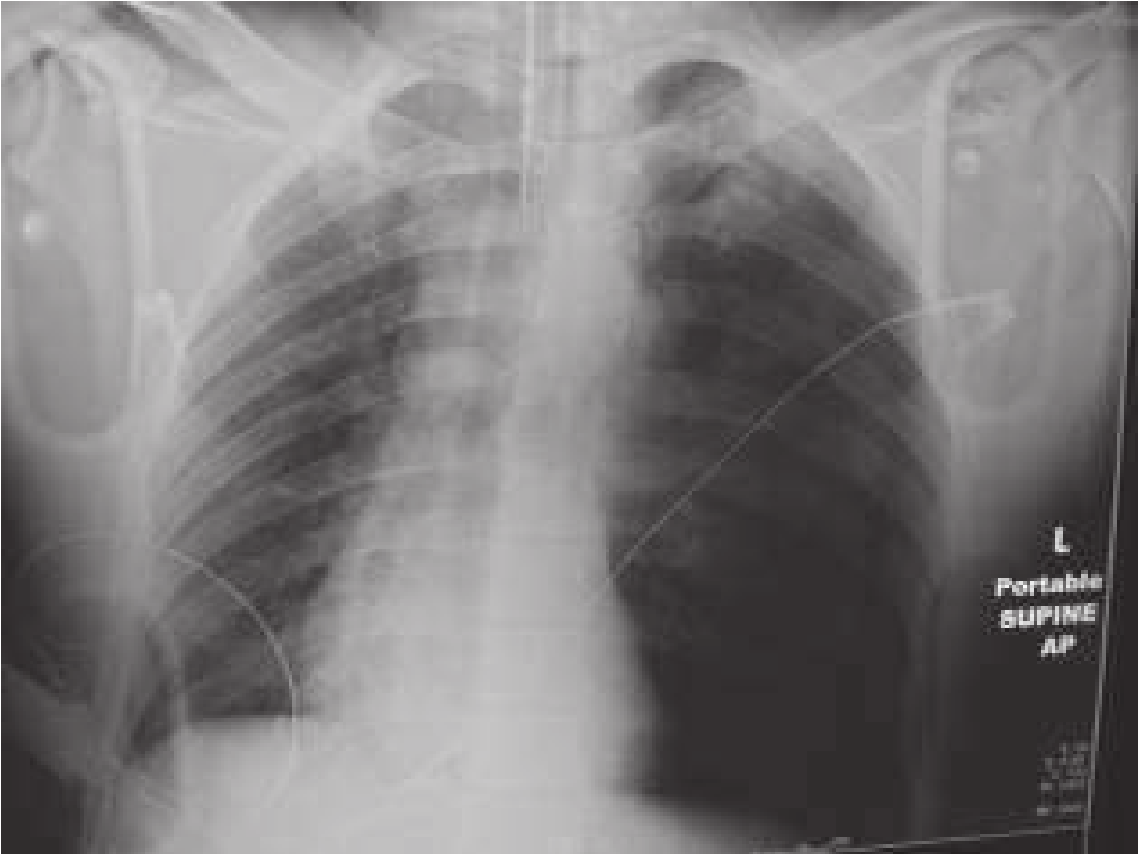
Classic tension pneumothorax in an intubated patient. Note the completely collapsed left lung, leftward shift of air with the right lung overstretched, and mediastinal displacement.
CXR 3: After left-sided chest tube insertion - tension resolved

Left-sided tube thoracostomy placed. The tension is relieved - both lungs are now visible, and the mediastinum has returned toward midline.
CT Chest
More sensitive than CXR - detects at least twice as many pneumothoraces.
CT: Occult left-sided pneumothorax (missed on CXR)
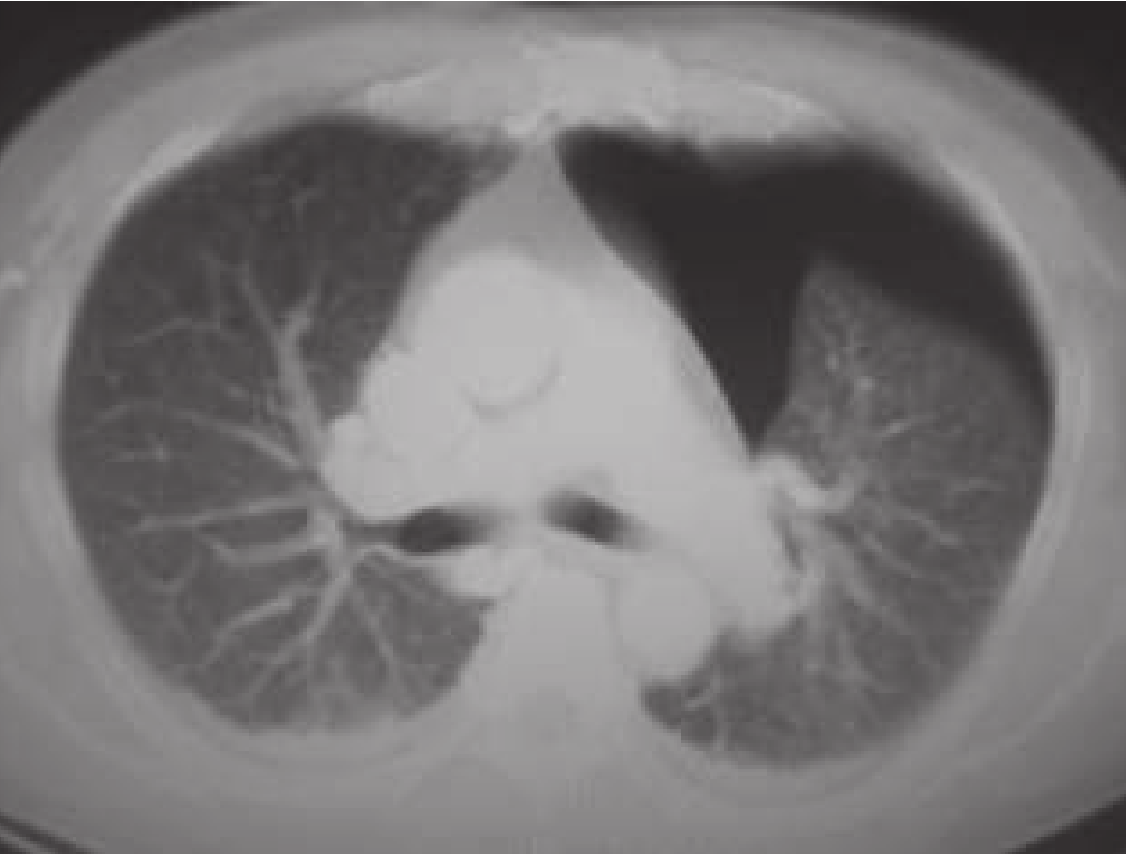
CT cross-section showing a large left-sided pneumothorax (black area around the collapsed left lung). This was invisible on the plain chest X-ray.
CT is used when:
- Occult pneumothorax suspected
- Need to distinguish pneumothorax from bullous emphysema
- Loculated collections requiring image-guided drainage
- Pre-surgical planning
Ultrasound (POCUS)
Increasingly used at the bedside - higher sensitivity (79-98%) than CXR (28-52%), though similar specificity (~98-99%).
Key ultrasound signs:
| Sign | Meaning |
|---|---|
| Lung sliding present | Pleural layers moving together - pneumothorax EXCLUDED at that site |
| Lung sliding absent | Suggestive of pneumothorax (but not specific alone) |
| B-lines present | Pleural contact maintained - pneumothorax EXCLUDED |
| Barcode/stratosphere sign (M-mode) | Absent sliding - pneumothorax |
| Seashore sign (M-mode) | Normal - no pneumothorax |
| Lung point | Boundary between sliding/no-sliding - highly specific for pneumothorax; can estimate size |
6. Sizing
| Size Classification | Definition | Implication |
|---|---|---|
| Small | <2 cm rim of air (BTS) or <15-20% volume | Conservative management |
| Large | ≥2 cm rim (BTS) or ≥15-20% volume | Intervention usually needed |
7. Management
Algorithm Overview
Pneumothorax confirmed
├── Tension pneumothorax? → IMMEDIATE DECOMPRESSION (don't wait for CXR!)
│
├── Traumatic? → Tube thoracostomy (24 Fr or pigtail via Seldinger)
│
└── Spontaneous?
├── Small + asymptomatic + PSP → Observation, repeat CXR in 4-6h
│
├── Large or symptomatic PSP → Aspiration or chest tube
│
└── Any SSP → Chest tube (higher risk of tension with PPV)
Tension Pneumothorax - Emergency Treatment
Treat clinically - do NOT wait for imaging!
-
Needle decompression (temporizing):
- 14-16G IV catheter (minimum 5 cm length)
- 2nd intercostal space, midclavicular line OR 4th/5th ICS, midaxillary line
- Air escaping under pressure = confirms diagnosis
- Follow immediately with chest tube
-
Finger/tube thoracostomy (definitive):
- May be done directly in the ED - often faster than needle decompression
Chest Tube (Tube Thoracostomy)
Indications (Box 37.2):
- Traumatic pneumothorax (except small asymptomatic apical)
- Moderate-to-large pneumothorax
- Respiratory symptoms, any size
- Pneumothorax on positive pressure ventilation
- Increasing size after initial observation
- Recurrence after previous chest tube
Technique:
- Small-bore tube (24 Fr) or pigtail catheter (Seldinger technique) for simple pneumothorax
- Connected to water-seal drainage unit with suction at -20 cmH2O
- Reduce to water seal only once air leak stops
- Clamp test for 4 hours; remove if CXR clear
- Air leak persisting >4-7 days = tube failure → surgical intervention
Recurrence Prevention
- Recurrence rate ~30% after first episode
- Options: pleurodesis (sclerosing agent instilled or mechanical abrasion), surgical resection of apical blebs/bullae (via VATS)
- Pleurodesis recommended after second episode or first episode in high-risk patients (pilots, divers)
Disposition
| Scenario | Disposition |
|---|---|
| Young, healthy, small PSP, no hypoxemia | Observe 4-6h, discharge with follow-up in 24-48h |
| Large PSP or SSP | Admission |
| Tension or traumatic | ICU/admission |
| Any pneumothorax | Avoid air travel and scuba diving until fully resolved |
8. Complications
- Tension pneumothorax - if simple pneumothorax not managed on PPV
- Reexpansion pulmonary edema - rare, after rapid evacuation of large chronic pneumothorax
- Hemopneumothorax - blood + air in pleural space (from torn adhesions in recurrent PSP)
- Bronchopleural fistula - persistent air leak
- Recurrence (~30%)
9. Quick Comparison Table
| Feature | PSP | SSP | Tension |
|---|---|---|---|
| Patient | Young, thin, male | COPD, lung disease | Any |
| Cause | Bleb rupture | Bullae/disease | Valve mechanism |
| Mediastinal shift | No | No | Yes |
| Hemodynamics | Stable | Stable/compromised | Shock |
| JVD | No | No | Yes |
| Urgency | Semi-urgent | Urgent | Immediate |
| Treatment | Observe/aspiration | Chest tube | Needle decompression NOW |
Sources:
- Rosen's Emergency Medicine, 9e, Chs. 37 & 63
- Murray & Nadel's Textbook of Respiratory Medicine (POCUS section)
- Roberts & Hedges' Clinical Procedures in Emergency Medicine
- Goldman-Cecil Medicine, International Edition
What is darier sign
Reading File
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
Analyze this file and teach me the content of it that is most important and give me all important points
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
This is a shared conversation. Sign in to Orris to start your own chat.