Tell me about lymph nodes and its examination with anatomy
Reading File
Finding Sources
Finding Sources
Searching Images
lymph node anatomy structure
Finding Sources
Reading File
Searching Images
lymph node histology cortex medulla germinal center
Finding Sources
Reading File
Loading Image
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full answer.
Lymph Nodes — Anatomy & Clinical Examination
1. Overview
There are approximately 600 lymph nodes throughout the body. They are small, bean-shaped, encapsulated organs distributed along lymphatic vessels, acting as biological filters and sites of immune activation. — Harrison's Principles of Internal Medicine 22E
2. Gross Anatomy
| Feature | Description |
|---|---|
| Shape | Bean-shaped, 1–25 mm |
| Capsule | Outer collagenous fibrous capsule |
| Trabeculae | Fibrous extensions from capsule that subdivide the node |
| Hilus | Concave indentation; entry of artery and vein, exit of efferent lymphatic |
| Afferent vessels | Enter through convex surface (multiple) |
| Efferent vessel | Exits at the hilus (single) |
3. Microanatomy (Internal Structure)
The diagram below shows the full internal architecture:
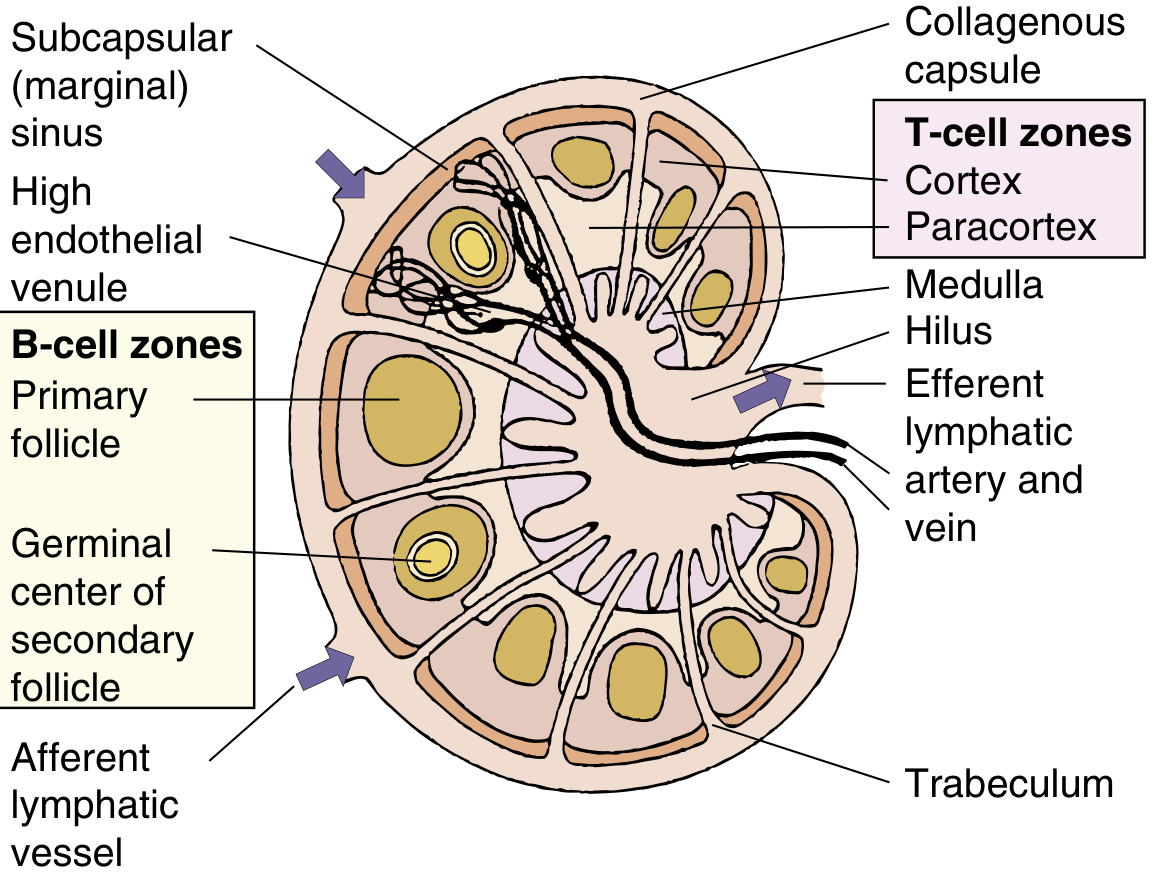
Fig. Organization of the lymph node — Medical Microbiology 9e (Elsevier)
Zones and Their Cellular Composition
| Zone | Location | Cell Type | Function |
|---|---|---|---|
| Subcapsular (marginal) sinus | Just beneath capsule | Phagocytic macrophages | Filters lymph from afferent vessels |
| Cortex | Outer zone | B cells in primary follicles | Humoral immunity; B-cell activation |
| Germinal centers (secondary follicles) | Within cortex | Activated B cells, follicular dendritic cells | Site of B-cell proliferation, somatic hypermutation, affinity maturation; plasma cell and memory B-cell development |
| Paracortex | Between cortex and medulla | T cells, dendritic cells | Cell-mediated immunity; antigen presentation |
| High endothelial venules (HEV) | Paracortex | Specialized endothelium | Entry of naïve lymphocytes from blood into the node |
| Medulla | Central/inner zone | T cells, B cells, plasma cells in medullary cords | Antibody production and final lymph filtration |
| Medullary sinuses | Around medullary cords | Macrophages | Further phagocytic filtration before efferent exit |
"The cortex contains B cells grouped in primary follicles and stimulated B cells in secondary follicles (germinal centers). The paracortex contains mainly T cells and dendritic cells. Lymphocytes enter the node from the circulation through the specialized high endothelial venules in the paracortex. Lymphocytes can leave the node only through the efferent lymphatic vessel." — Medical Microbiology 9e
Histology (H&E)
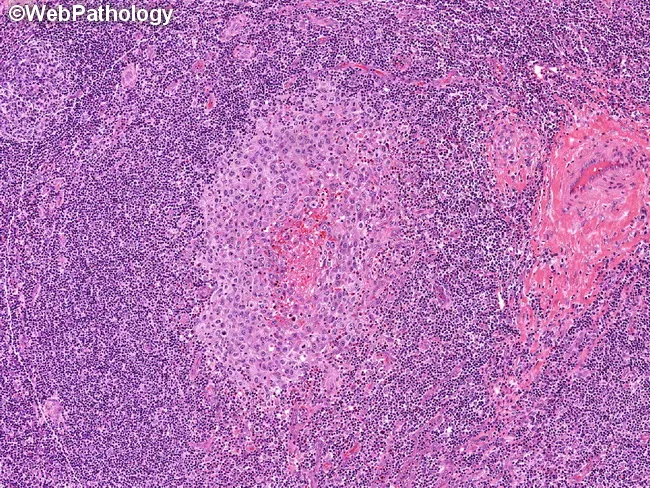
Normal lymph node histology: pale germinal centers (B-cell zones) surrounded by dark mantle zones of small lymphocytes, with T-cell-rich interfollicular paracortex
4. Lymph Node Groups — Regional Anatomy
Head & Neck Nodes (Most Clinically Important)
The American Head and Neck Society classification uses 6 levels + additional regions:
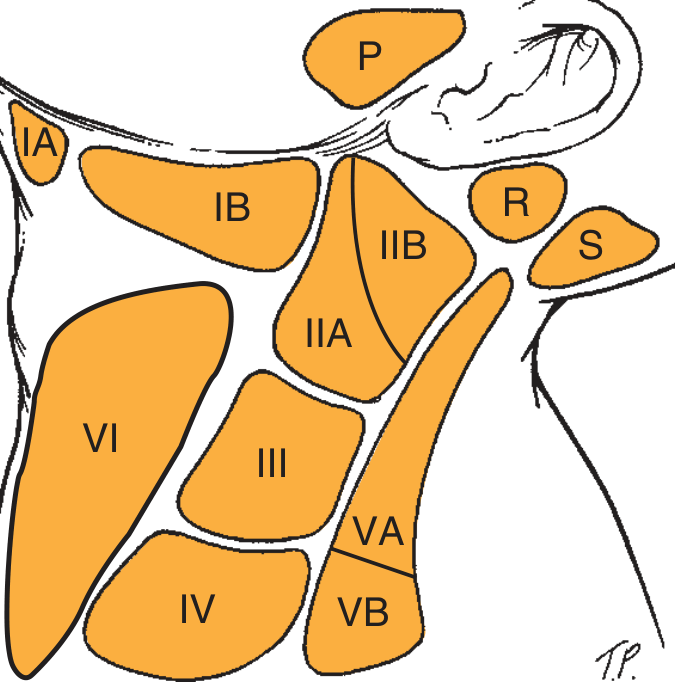
Fig. Lymph node levels of the neck — Cummings Otolaryngology
| Level | Location | Key Nodes | Drains |
|---|---|---|---|
| IA | Submental triangle | Submental nodes | Floor of mouth, tip of tongue, lower lip |
| IB | Submandibular triangle | Submandibular nodes | Oral cavity, anterior face |
| IIA | Upper jugular (medial to CN XI) | Jugulodigastric nodes | Tonsil, pharynx, oral cavity |
| IIB | Upper jugular (lateral to CN XI) | Upper spinal accessory chain | Posterior scalp |
| III | Middle jugular (hyoid → cricoid) | Mid-jugular nodes | Larynx, hypopharynx |
| IV | Lower jugular (cricoid → clavicle) | Lower jugular nodes | Thyroid, cervical esophagus |
| VA | Posterior triangle superior | Spinal accessory nodes | Posterior scalp, skin |
| VB | Posterior triangle inferior | Supraclavicular, transverse cervical nodes | Thorax, abdomen (Virchow's node is in level IV) |
| VI | Central compartment | Pretracheal, paratracheal, Delphian node | Thyroid, larynx, cervical trachea |
| P | Parotid/preauricular | — | Anterior scalp, face, ear |
| R | Retroauricular | — | Posterior scalp, pinna |
| S | Suboccipital | — | Posterior scalp |
"The Virchow node is not in the VB region but is located in level IV." — Cummings Otolaryngology
Other Major Node Groups
| Region | Key Node Groups | Drains |
|---|---|---|
| Axillary | Anterior (pectoral), posterior (subscapular), lateral, central, apical | Arm, breast, chest wall |
| Inguinal (superficial) | Along inguinal ligament and great saphenous vein | Lower limb, perineum, external genitalia, anal canal below dentate line |
| Inguinal (deep) | Along femoral vessels, Cloquet's node | Deep structures of lower limb |
| Epitrochlear | Medial arm above elbow | Ulnar forearm, hand (4th and 5th fingers) |
| Popliteal | Behind knee | Foot, posterior lower leg |
| Mesenteric | Along superior/inferior mesenteric vessels | GI tract |
| Mediastinal | Paratracheal, subcarinal, hilar | Lungs, trachea, esophagus |
| Para-aortic (lumbar) | Alongside aorta | Testes/ovaries, kidneys, uterus |
5. Clinical Examination of Lymph Nodes
General Principles
A physical examination should assess lymph nodes in multiple regions — popliteal, inguinal, epitrochlear, axillary, and multiple cervical regions. For each palpable node, document: — Harrison's Principles of Internal Medicine 22E
| Parameter | What to Note |
|---|---|
| Location | Which anatomical region |
| Size | Normal <1 cm in adults; <1.5 cm in children |
| Tenderness | Present (suggests infection/inflammation) or absent |
| Consistency | Soft (reactive/infection), firm/rubbery (lymphoma), hard (metastatic carcinoma) |
| Mobility | Mobile (benign reactive) vs. fixed/matted (malignancy, TB, extranodal extension) |
| Overlying skin | Erythema, warmth, sinus tracts |
| Number | Single vs. multiple |
| Borders | Discrete vs. matted (nodes connected and moving together) |
"Nodes that are small and firm can also be described as 'shotty', referring to the size and consistency of buckshot pellets. Palpable epitrochlear nodes are always pathologic." — Harrison's 22E
Technique
- Use pads of 2–3 fingers, applying gentle circular pressure
- In the neck: examine systematically from Level I → VI, comparing both sides
- Submandibular area: bimanual palpation (gloved finger in floor of mouth) distinguishes nodes from the submandibular gland
- Carotid artery can be mistaken for a pulsatile node — auscultate for a bruit; pulsatility distinguishes it
"In the superior cervical chain, it is very common to have multiple, borderline, enlarged, indistinct, or slightly firm nodes that are often termed 'shoddy'." — Cummings Otolaryngology
Size Thresholds for Pathology
| Population | Pathologic Threshold |
|---|---|
| Adults | >1 cm in most regions |
| Children | >1.5 cm in greatest diameter |
| All patients | Any palpable epitrochlear node |
| All patients | Any palpable supraclavicular node (always pathologic) |
Characteristics That Suggest Malignancy vs. Benign
| Feature | Benign/Reactive | Malignant |
|---|---|---|
| Consistency | Soft, rubbery | Hard, stony |
| Mobility | Mobile | Fixed to skin or deep structures |
| Tenderness | Often tender | Usually non-tender |
| Growth | Fluctuating | Progressive |
| Duration | Acute (<4–6 weeks) | Subacute/chronic (>4–6 weeks) |
| Skin | Normal | Dimpling, attachment, ulceration |
6. Differential Diagnosis of Lymphadenopathy
Localised vs. Generalised
- Localized lymphadenopathy: found in the head/neck (55% of cases), inguinal (14%), axillary (5%) — suggests regional infection, trauma, or local malignancy
- Generalised (≥2 non-contiguous regions): suggests systemic disease — viral infection, lymphoma, HIV, autoimmune disorders, drugs
Key Clinical Framework (Cervical)
| Presentation | Most Likely Cause |
|---|---|
| Acute bilateral cervical nodes | Viral URTI |
| Acute unilateral cervical nodes | Bacterial (Staph, Strep) |
| Subacute/chronic (>4–6 weeks) | Granulomatous infection (TB, atypical mycobacteria), malignancy |
| Progressive enlargement | Malignancy |
| Fluctuating size | Inflammatory/infectious |
— Tintinalli's Emergency Medicine
Causes by Category
| Category | Examples |
|---|---|
| Infectious | EBV (infectious mononucleosis), CMV, HIV, Toxoplasmosis, TB, cat-scratch disease (Bartonella), tularemia |
| Autoimmune/inflammatory | SLE, rheumatoid arthritis, sarcoidosis |
| Malignant — primary | Hodgkin lymphoma, non-Hodgkin lymphoma |
| Malignant — metastatic | Carcinoma (squamous cell, thyroid, breast, lung, GI) |
| Drug-induced | Phenytoin, allopurinol, hydralazine |
| Miscellaneous | Kawasaki disease, Castleman disease |
7. Special Clinical Notes
- Virchow's node (left supraclavicular/level IV node): enlargement suggests metastatic intra-abdominal or thoracic malignancy (sentinel node of Troisier's sign)
- Sister Mary Joseph node (periumbilical): intra-abdominal malignancy
- Delphian node (precricoid, level VI): enlargement in thyroid carcinoma or subacute thyroiditis
- Extranodal extension: nodes feel fixed and immobile on examination; diagnosed pathologically or when fixation is evident on palpation/imaging — Sabiston Textbook of Surgery
- Adults >40 years with unexplained lymphadenopathy lasting >4 weeks should have biopsy considered to exclude lymphoma or metastatic disease
Sources: Medical Microbiology 9e, Harrison's Principles of Internal Medicine 22E, Cummings Otolaryngology: Head and Neck Surgery, Tintinalli's Emergency Medicine, Sabiston Textbook of Surgery
This is a shared conversation. Sign in to Orris to start your own chat.