Can you explain cardiac output
Reading File
Finding Sources
Searching PubMed
"cardiac output" physiology determinants
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Reading File
I now have comprehensive textbook content from multiple authoritative sources. Here is the full explanation:
Cardiac Output
Definition and Formula
Cardiac output (CO) is the total volume of blood ejected by the heart per unit time. It is the product of two variables:
CO = Stroke Volume (SV) × Heart Rate (HR)
- Stroke volume = volume ejected in one beat (mL)
- Heart rate = beats per minute
In a resting 70-kg adult, a typical stroke volume of ~70 mL and HR of ~72 beats/min gives:
CO = 70 mL × 72 beats/min = ~5,000 mL/min (5 L/min)
The normal resting range is roughly 4-8 L/min.
- Costanzo Physiology 7th Edition, p. 155
Cardiac Index
Because cardiac output scales with body size, it is often normalized to body surface area (BSA):
Cardiac Index (CI) = CO / BSA (m²)
Normal CI at rest = ~3.0-3.2 L/min/m². In a 70-kg adult, BSA is approximately 1.7 m², giving a CI of about 3 L/min/m². CI peaks around age 10 (>4 L/min/m²) and declines to ~2.4 L/min/m² by age 80.
- Guyton and Hall Textbook of Medical Physiology, p. 251
Determinants of Cardiac Output
1. Heart Rate
When stroke volume is constant, CO is directly proportional to HR. The SA node's intrinsic rate in young adults is ~90-100 beats/min but is modified by:
- Sympathetic stimulation (via β1-adrenergic receptors): increases HR (positive chronotropy)
- Parasympathetic/vagal stimulation (via M2 cholinergic receptors): decreases HR
Normal intrinsic HR ≈ 118 beats/min - (0.57 × Age)
2. Stroke Volume
Stroke volume is governed by three primary factors:
| Factor | Definition | Effect on SV |
|---|---|---|
| Preload | End-diastolic volume (EDV) - ventricular filling | Higher preload → higher SV (Frank-Starling) |
| Afterload | Resistance the ventricle must overcome to eject blood (SVR) | Higher afterload → lower SV |
| Contractility | Intrinsic force of myocardial contraction | Higher contractility → higher SV |
- Morgan and Mikhail's Clinical Anesthesiology 7e, p. 657
Preload and the Frank-Starling Law
Preload = ventricular end-diastolic volume (EDV), which reflects venous return. Otto Frank and Ernest Starling independently established that:
The volume ejected in systole is determined by the volume present at end-diastole.
This is the Frank-Starling law: as EDV increases, myocardial fibers are stretched, producing a stronger contraction (length-tension relationship), and therefore a larger stroke volume and higher CO. This mechanism ensures that the heart automatically pumps what it receives - in steady state, CO equals venous return.
The Frank-Starling curve shifts with contractility:
- Positive inotropes (e.g., digoxin, catecholamines): shift curve upward - higher CO for the same EDV
- Negative inotropes (e.g., beta-blockers, acidosis, hypoxia): shift curve downward
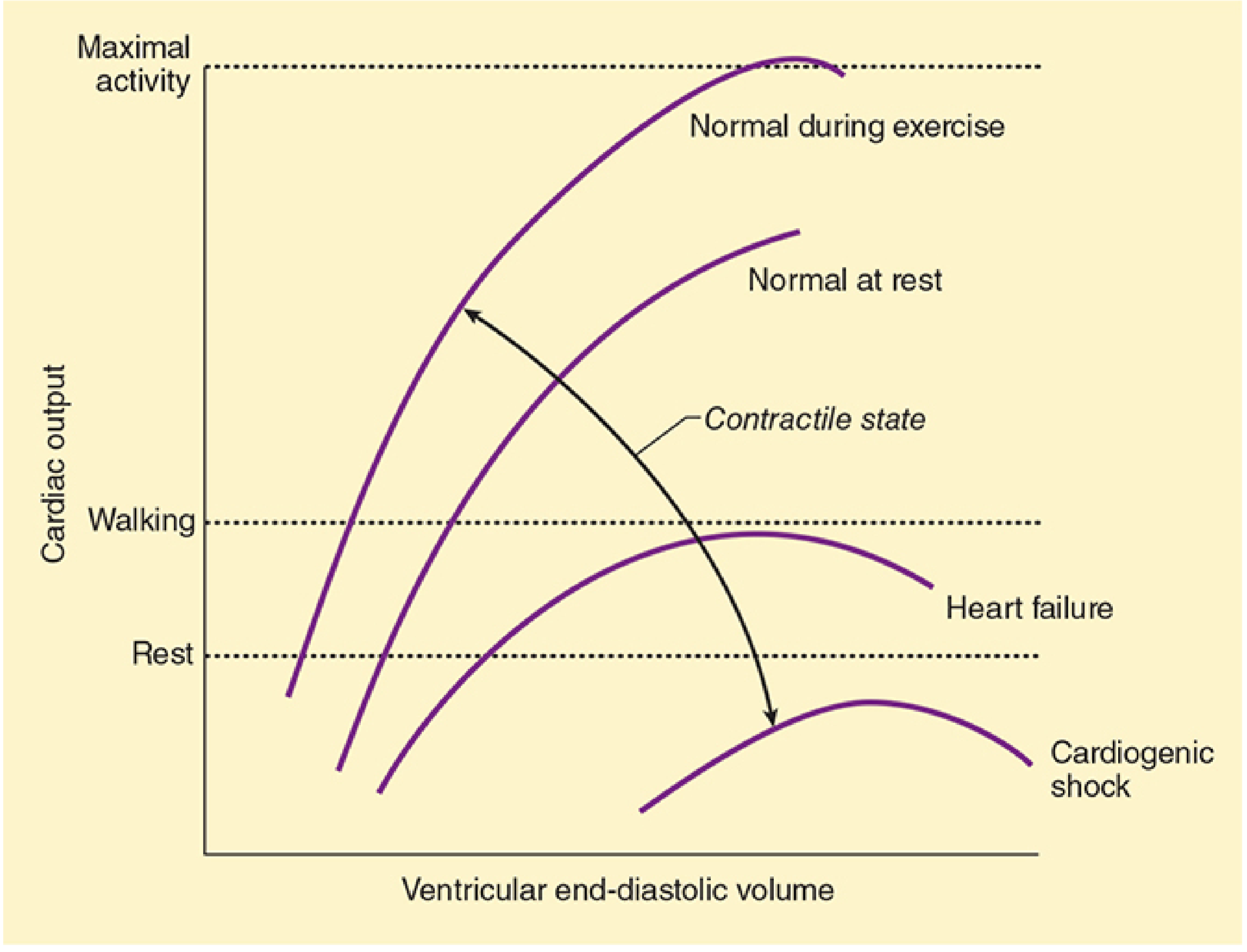
Starling's law illustrated. During exercise, contractility increases and the curve shifts up. In heart failure and cardiogenic shock, depressed contractility causes the curve to drop. - Morgan and Mikhail's Clinical Anesthesiology 7e
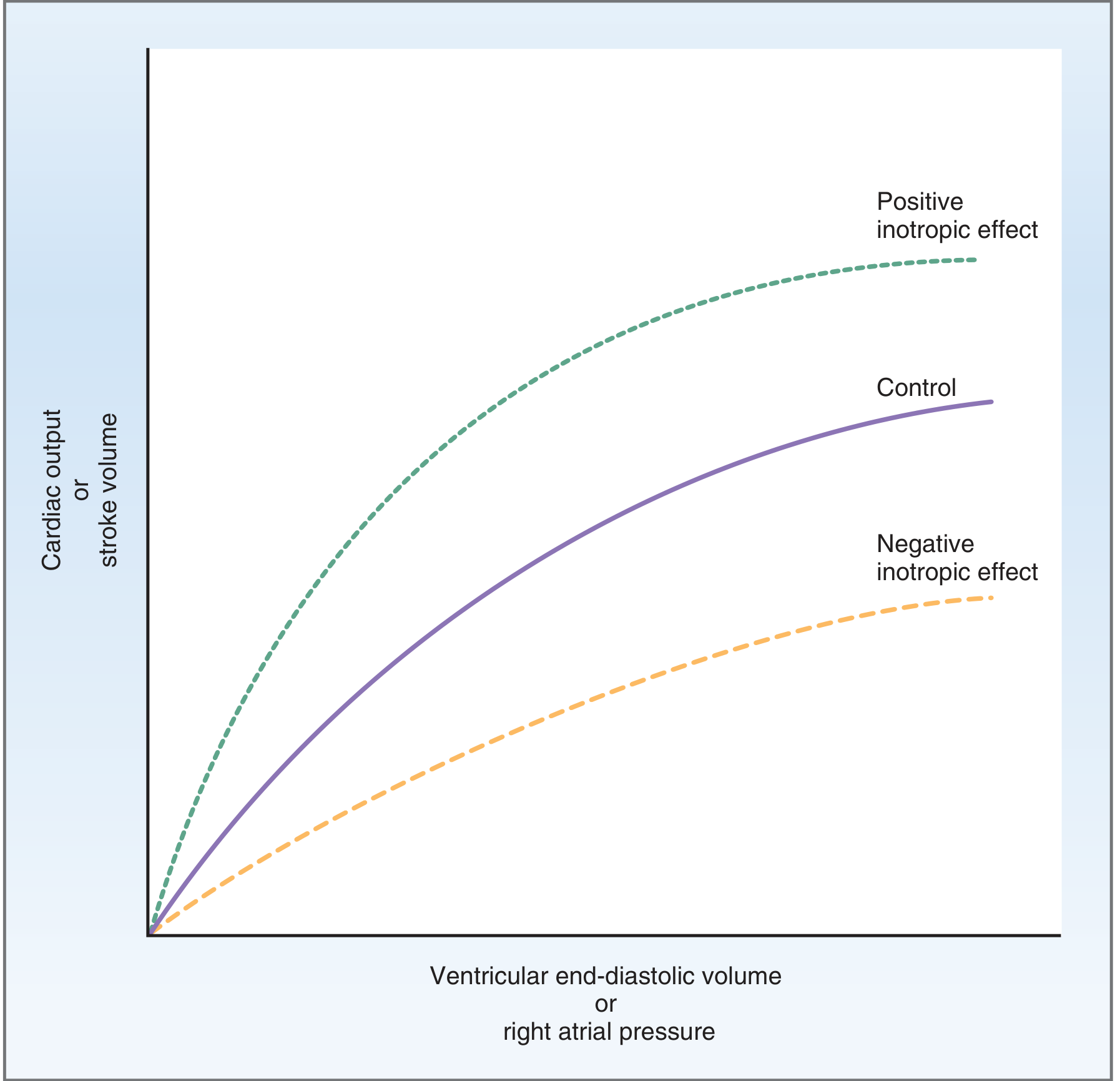
Frank-Starling curves: the positive inotropic effect (green, top) shifts the relationship upward; negative inotropic effect (orange, bottom) shifts it downward relative to control (purple). - Costanzo Physiology 7th Edition
Afterload
Afterload is the tension/resistance the ventricle must overcome during ejection. For the left ventricle, this is approximated clinically by systemic vascular resistance (SVR):
SVR = 80 × (MAP - CVP) / CO (normal: 900-1,500 dyn·s·cm⁻⁵)
- Larger ventricular radius increases wall tension required (LaPlace's law: T = P × R / 2H)
- CO falls in response to large increases in afterload
- The right ventricle is more sensitive to afterload changes than the left, due to its thinner wall
- Morgan and Mikhail's Clinical Anesthesiology 7e, p. 661
Contractility (Inotropy)
Contractility is the intrinsic ability of the myocardium to generate force, independent of preload and afterload. It is governed by intracellular Ca²⁺ concentration during systole.
Increases contractility (positive inotropy):
- Sympathetic stimulation (norepinephrine, epinephrine via β1 receptors)
- Digoxin
- Calcium, catecholamines
Decreases contractility (negative inotropy):
- Hypoxia, acidosis
- Loss of functioning myocardium (ischemia, infarction)
- Most anesthetics and antiarrhythmics at high doses
- Catecholamine depletion
- Morgan and Mikhail's Clinical Anesthesiology 7e, p. 662
Ejection Fraction
Ejection fraction (EF) is a measure of ventricular efficiency:
EF = Stroke Volume / End-Diastolic Volume
A normal EF is ~50-70%. For example, SV of 70 mL from an EDV of 140 mL gives EF = 0.50 (50%). EF increases with positive inotropy and decreases in heart failure.
Regulation by Venous Return
Under most resting conditions, venous return - not the heart itself - is the primary controller of CO. Peripheral factors (metabolic activity, vascular tone, blood volume) determine how much blood returns to the right atrium. The Frank-Starling mechanism then ensures the heart pumps exactly what it receives. When metabolic activity increases (exercise, fever), vascular capacity decreases, venous return increases, and CO rises automatically.
- Guyton and Hall Textbook of Medical Physiology, p. 251
CO in Different Conditions
| Condition | CO |
|---|---|
| Resting adult | ~5 L/min |
| Exercise (trained athlete) | Up to 20-25 L/min |
| Heart failure | Reduced (depressed contractility curve) |
| Cardiogenic shock | Severely reduced |
| Pregnancy (third trimester) | Increased (~30-50% above baseline) |
| Anemia, AV fistula, hyperthyroidism | Elevated (high-output states) |
- Ganong's Review of Medical Physiology 26th Edition
Summary mnemonic: CO depends on HR and SV; SV depends on Preload, Afterload, and Contractility (PAC).
This is a shared conversation. Sign in to Orris to start your own chat.