Give me a comprehensive and detailed analysis on "Conjunctivitis"
Reading File
Finding Sources
Searching PubMed
"conjunctivitis" AND "diagnosis AND treatment"
Searching the Web
conjunctivitis comprehensive clinical overview 2025 etiology diagnosis treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
I now have comprehensive material from 6+ authoritative sources. Let me compile the full detailed analysis.
Conjunctivitis: A Comprehensive Clinical Analysis
1. Definition and Anatomy
Conjunctivitis is inflammation of the conjunctiva - the mucous membrane lining the inner surface of the eyelids (palpebral conjunctiva) and covering the globe of the eye up to the corneoscleral junction (bulbar conjunctiva). It is the most common ocular infection worldwide and a frequent cause of the "red eye."
The conjunctiva serves as a protective mucosal barrier; when inflamed, it produces increased vascular permeability, cellular infiltration, and secretion - the hallmarks of the clinical presentation.
2. Classification and Etiology
Conjunctivitis is broadly categorized by etiology:
2.1 Infectious
Viral (Most Common)
Viral causes are thought to be the most frequent infectious etiology. Adenoviruses dominate, accounting for the majority of cases and exhibiting high contagiousness. Other viral pathogens include:
| Pathogen | Notes |
|---|---|
| Adenovirus | Most common; causes epidemic keratoconjunctivitis (EKC) in certain serotypes |
| Herpes Simplex Virus (HSV) | Can extend beyond conjunctiva to cornea with dendritic keratitis |
| Varicella Zoster Virus (VZV) | Associated with pseudodendrites; may disseminate to deeper structures |
| Enterovirus / Coxsackievirus A24 | Causes acute hemorrhagic conjunctivitis |
| Influenza, EBV, Measles, Mumps, Rubella | Rare, self-limited |
| Molluscum contagiosum, HPV | Rare |
Symptoms typically resolve spontaneously within 2 weeks; however, certain adenovirus serotypes may cause EKC where symptoms last weeks to months.
- Tietz Textbook of Laboratory Medicine, 7th Ed.
Bacterial
Bacterial conjunctivitis can occur at any age from the first day of life. The major pathogens vary by age group:
Common (non-severe) organisms:
- Staphylococcus aureus (predominates in adults)
- Streptococcus pneumoniae
- Haemophilus influenzae (more common in children)
- Moraxella catarrhalis
- Escherichia coli, Pseudomonas aeruginosa (especially in soft contact lens wearers)
Serious/Hyperacute organisms:
- Neisseria gonorrhoeae - causes hyperacute conjunctivitis with copious thick yellowish-green discharge; can rapidly perforate the cornea; requires systemic antibiotics
- Neisseria meningitidis - less common but serious
- Chlamydia trachomatis - causes inclusion conjunctivitis and trachoma (leading infectious cause of blindness worldwide)
Chlamydial Conjunctivitis (Special Category)
Chlamydia trachomatis deserves particular attention:
- Inclusion conjunctivitis results from sexually acquired C. trachomatis, causing redness and mucopurulent discharge
- Trachoma (serotypes A, B, Ba, C) is the leading infectious cause of blindness globally. It begins with mild follicular conjunctivitis; repeated infections produce scarring that inverts the upper eyelids (trichiasis), and the eyelashes abrading the cornea ultimately cause corneal ulceration, scarring, and opacification.
- The WHO's SAFE strategy (Surgery for trichiasis, Antibiotics for active infection, Facial cleanliness, Environmental improvement) has brought the at-risk population down to ~142 million (as of 2019).
- Robbins & Kumar Basic Pathology, Tietz Textbook of Laboratory Medicine
2.2 Allergic
The second most common category. Allergens trigger IgE-mediated mast cell degranulation in the conjunctiva, releasing histamine and other mediators.
Subtypes:
- Seasonal allergic conjunctivitis (SAC): Most common; triggered by pollens; bilateral, seasonal
- Perennial allergic conjunctivitis (PAC): Year-round; triggered by dust mites, animal dander
- Vernal keratoconjunctivitis (VKC): Recurrent, seasonal (spring/early summer); more common in young males in warm climates; characteristic cobblestone papillae under the upper lid (see image below)
- Giant papillary conjunctivitis (GPC): Associated with soft contact lens wear; caused by allergy to sterilizing solutions and lens proteins; managed by switching to preservative-free solutions or daily-wear disposable lenses
2.3 Other Causes
- Toxic/Chemical: Exposure to chlorine, smoke, chemicals; also from certain topical medications (gentamicin, neomycin, sulfacetamide can cause toxic chemical conjunctivitis)
- Parasitic/Fungal: Rare
- Neonatal (Ophthalmia Neonatorum): Requires separate evaluation (discussed below)
3. Clinical Features and Diagnosis
The diagnosis is primarily clinical. Laboratory tests are not routine unless serious infection is suspected or the diagnosis is uncertain.
3.1 Key Symptom Comparison
| Feature | Viral | Bacterial | Allergic |
|---|---|---|---|
| Discharge | Watery, serous | Mucopurulent, thick | Watery, stringy mucus |
| Laterality | Unilateral → bilateral | Unilateral or bilateral | Bilateral |
| Itching | Mild | Minimal | Prominent (hallmark) |
| Pain | Absent (mild if keratitis) | Absent | Absent |
| Lid crusting | Mild | Marked (lids stuck on waking) | Mild |
| Preauricular LN | Present (follicular) | Absent (except gonococcal) | Absent |
| Conjunctival finding | Follicles on inferior palpebral conjunctiva | Papillae; chemosis | Papillae; chemosis; eyelid edema |
| Associated history | URI, fever, systemic illness | None | Atopy, seasonal exposure |
3.2 Visual Findings
Bacterial conjunctivitis - mucopurulent discharge, conjunctival injection, lid edema:

Epidemic Keratoconjunctivitis (EKC) - diffuse bulbar conjunctival injection with papillae:
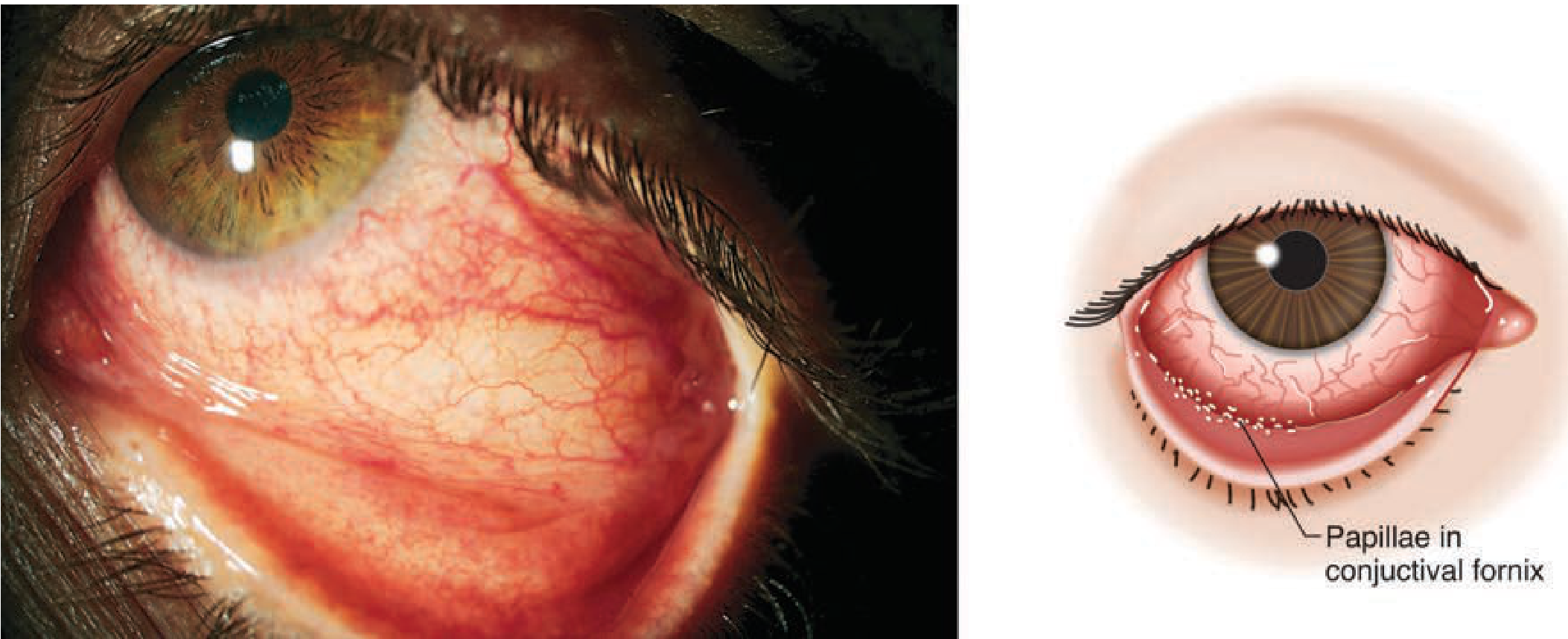
Vernal conjunctivitis - cobblestone papillae under upper lid:
3.3 Slit-Lamp Findings
- Follicles (small, regular, translucent bumps on inferior palpebral conjunctiva) - indicate viral or chlamydial etiology
- Papillae (irregular mounds with central vascular tuft) - indicate bacterial or allergic etiology
- Punctate fluorescein staining - indicates keratitis (most commonly in EKC or HSV)
- Chemosis (conjunctival edema) - common in bacterial and allergic types
3.4 Red Flags Requiring Urgent Ophthalmologic Consultation
The following should prompt urgent referral:
- Decreased visual acuity
- Severe eye pain (suggests iritis, keratitis, acute glaucoma)
- Photophobia
- Corneal opacity or fluorescein staining (possible herpetic dendrite or corneal ulcer)
- Copious purulent discharge suggestive of gonococcal infection
- Failure to improve after 2 weeks of treatment
- Neonatal conjunctivitis
4. Special Forms
4.1 Epidemic Keratoconjunctivitis (EKC)
- Caused by adenovirus (particularly serotypes 8, 19, 37)
- Highly contagious; can cause outbreaks in workplaces and healthcare settings
- Systemic symptoms (cough, high fever, malaise, myalgias) may precede ocular involvement
- Corneal subepithelial infiltrates develop, causing photophobia and decreased vision
- Can last weeks to months
- Infection control: examiner must wear gloves, disinfect slit lamp and furniture after each patient contact
4.2 Gonococcal Conjunctivitis
- Hyperacute onset with profuse, thick, purulent discharge within 12-24 hours
- Tender preauricular lymphadenopathy
- High risk of corneal perforation if untreated
- In neonates: presents within 2-5 days of birth (from maternal genital tract)
- Diagnosis: Gram stain shows gram-negative intracellular diplococci; culture on Thayer-Martin medium
- Treatment: systemic antibiotics required (not just topical) - ceftriaxone IV/IM
4.3 Chlamydial (Inclusion) Conjunctivitis in Adults
- Sexually transmitted; inoculation from genital secretions to eye
- Follicular conjunctivitis; chronic and persistent if untreated
- Treated with oral azithromycin or doxycycline (systemic treatment, as topical alone is insufficient)
4.4 Herpes Simplex Conjunctivitis
- Presents as unilateral follicular conjunctivitis
- Look for conjunctival dendrites or geographic ulceration
- Critical: always stain with fluorescein to detect herpetic dendrite in the cornea - a branching linear ulceration with club-shaped terminal bulbs at each branch end
- Treatment: topical antivirals (trifluridine, ganciclovir gel) or oral acyclovir/valacyclovir
- Avoid topical steroids without ophthalmologic consultation - can dramatically worsen HSV infection
4.5 Ophthalmia Neonatorum (Neonatal Conjunctivitis)
A serious condition requiring prompt evaluation in the newborn:
| Cause | Onset | Features |
|---|---|---|
| Chemical (silver nitrate) | Day 1 | Mild, self-limited |
| N. gonorrhoeae | Days 2-5 | Profuse purulent discharge; risk of corneal perforation |
| C. trachomatis | Days 5-14 | Mucopurulent; also causes neonatal pneumonia |
| Bacterial (Staph, Strep) | Days 4-7 | Purulent discharge |
| HSV | Days 6-14 | Can disseminate systemically |
- Prevention: neonatal ocular prophylaxis (erythromycin ointment is the standard in the US; silver nitrate is no longer recommended)
- Gonococcal ophthalmia neonatorum requires systemic ceftriaxone
5. Diagnosis and Investigations
- Primary diagnosis is clinical in most cases
- Conjunctival swab culture and Gram stain: Reserved for severe, hyperacute, or neonatal cases; grow on blood agar and chocolate agar
- Fluorescein staining with cobalt blue light: mandatory to rule out corneal involvement - especially important in infants and when viral etiology is suspected
- PCR: Most sensitive test for adenovirus, HSV, chlamydia - used when diagnosis is uncertain or for contact tracing in outbreaks
- Antigen detection tests: Rapid adenovirus assays are available but have variable sensitivity
- Textbook of Family Medicine, 9e
6. Treatment
6.1 Viral Conjunctivitis
- Largely self-limiting (1-3 weeks)
- Cool compresses
- Artificial tears 5-6 times daily
- Ocular decongestants (e.g., Naphcon-A) 3 times daily as needed
- Antihistamines if itching is prominent
- Antibiotics are NOT indicated (unless bacterial superinfection or etiology is unclear)
- Strict infection control: frequent handwashing, separate towels, no sharing of eye makeup
- HSV keratoconjunctivitis: topical trifluridine or ganciclovir gel; systemic acyclovir for primary or severe disease
6.2 Bacterial Conjunctivitis
Most cases are self-limited; antibiotics shorten the duration of symptoms.
First-line options:
- Trimethoprim-polymyxin B - very effective; avoids sulfa and neomycin allergy concerns
- Erythromycin or bacitracin ointment - for mild cases, especially in children
- Topical fluoroquinolone (besifloxacin, gatifloxacin, levofloxacin, moxifloxacin, ofloxacin) - first-line for contact lens wearers (covers Pseudomonas) and for severe cases pending culture results
- Tobramycin - for gram-negative organisms
Caution: Gentamicin, neomycin, and sulfacetamide can cause toxic chemical conjunctivitis and should be used with caution.
Systemic antibiotics: Required when there is evidence of systemic spread, or for gonococcal (Neisseria) or chlamydial infection.
- Gonococcal: ceftriaxone IM/IV
- Chlamydial: oral azithromycin (1g single dose) or doxycycline (100mg BD x 7 days)
6.3 Allergic Conjunctivitis
Treatment is stepwise based on severity:
- Mild: Artificial tears alone; cool compresses 4 times daily; allergen avoidance
- Moderate: Topical antihistamine/decongestant (e.g., olopatadine, ketotifen); mast cell stabilizers (cromolyn sodium, lodoxamide); or topical NSAIDs
- Severe: Topical corticosteroids (consult ophthalmologist first - risk of activating latent HSV, inducing glaucoma, or cataract with prolonged use)
- Systemic antihistamines for associated rhinitis
6.4 Contact Lens Wearers
- Must be treated with a fluoroquinolone or tobramycin to cover Pseudomonas aeruginosa
- Contact lens wear should be discontinued until infection resolves
- Giant papillary conjunctivitis: switch to preservative-free solutions or daily-wear disposable lenses
- Tintinalli's Emergency Medicine
7. Complications
| Complication | Associated Type |
|---|---|
| Corneal ulceration and scarring | Trachoma (repeated C. trachomatis), gonococcal, HSV |
| Blindness | Trachoma (worldwide leading infectious cause), gonococcal, HSV |
| Corneal perforation | Gonococcal (hyperacute); can occur within hours |
| Subepithelial infiltrates | Epidemic keratoconjunctivitis (adenovirus) |
| Symblepharon | Severe chemical injury, Stevens-Johnson syndrome |
| Trichiasis | Advanced trachoma - inturned eyelashes scratching cornea |
| Systemic dissemination | Neonatal gonococcal, neonatal HSV |
| Keratoconjunctivitis sicca (dry eye) | Post-inflammatory scarring of lacrimal glands |
8. Differential Diagnosis of the Red Eye
Conjunctivitis must be distinguished from other important causes of red eye:
| Condition | Key Differentiating Features |
|---|---|
| Acute angle-closure glaucoma | Severe pain, halos, fixed mid-dilated pupil, hard globe, nausea/vomiting |
| Anterior uveitis (iritis) | Deep aching pain, photophobia, ciliary flush (perilimbal injection), cells/flare on slit lamp |
| Corneal ulcer/abrasion | History of trauma/contact lens use; pain; fluorescein staining positive; corneal opacity |
| Episcleritis | Sectoral redness; minimal discharge; mild or no pain |
| Scleritis | Severe boring pain; deep violaceous hue; associated with autoimmune disease |
| Subconjunctival hemorrhage | Flat blood under conjunctiva; no discharge, no itching; typically painless |
| Blepharitis | Lid margin inflammation; crusting at lash bases; chronic course |
- Goldman-Cecil Medicine, Tintinalli's Emergency Medicine
9. Conjunctivitis in Special Contexts
9.1 Contact Lens Wearers
At elevated risk for gram-negative (especially Pseudomonas) infection. Contact lenses must be removed and discarded. Always treat with a fluoroquinolone or tobramycin.
9.2 Immunocompromised Patients
More susceptible to unusual pathogens including fungi, atypical bacteria, and drug-resistant organisms. Lower threshold for culture.
9.3 HIV-Associated Conjunctivitis
Kaposi's sarcoma of the conjunctiva can rarely present as a subconjunctival hemorrhage-like lesion.
9.4 Stevens-Johnson Syndrome (SJS/TEN)
A severe mucocutaneous reaction that involves the conjunctiva with pseudomembranous conjunctivitis, which can lead to cicatricial (scarring) conjunctivitis and symblepharon formation - a sight-threatening emergency.
10. Prevention and Public Health
- Ophthalmia neonatorum prophylaxis: Erythromycin 0.5% ophthalmic ointment at birth (prevents gonococcal and partially chlamydial disease)
- Trachoma - WHO SAFE strategy:
- Surgery for trichiasis
- Antibiotics for active infection (oral azithromycin mass drug administration)
- Facial cleanliness
- Environmental improvement (access to water and sanitation)
- Contact precautions for EKC: Potentially requires exclusion from work/school; highly contagious via fomites; persists on surfaces for days
- Hand hygiene is the single most effective measure for preventing spread of viral and bacterial conjunctivitis
11. Summary Comparison Table
| Feature | Viral | Bacterial | Chlamydial | Allergic |
|---|---|---|---|---|
| Main pathogen | Adenovirus, HSV | Staph, Strep, H. flu | C. trachomatis | IgE-mediated |
| Discharge | Watery | Mucopurulent | Mucopurulent | Watery/stringy |
| Itching | Mild | Minimal | Absent | Prominent |
| Laterality | Bilateral | Uni or bilateral | Bilateral | Bilateral |
| Preauricular LN | Yes (follicular) | No (except GC) | Yes | No |
| Corneal risk | EKC, HSV dendrite | Gonococcal perforation | Trachoma scarring | Low |
| Treatment | Supportive | Topical antibiotics | Systemic antibiotics | Antihistamines/steroids |
| Self-limited? | Yes (1-3 weeks) | Yes (mild cases) | No (needs treatment) | Variable |
Sources:
- Tintinalli's Emergency Medicine: A Comprehensive Study Guide
- Robbins & Kumar Basic Pathology
- Tietz Textbook of Laboratory Medicine, 7th Edition
- Bailey and Love's Short Practice of Surgery, 28th Edition
- Textbook of Family Medicine, 9th Edition
- Goldman-Cecil Medicine, International Edition
- Wills Eye Manual - Office and Emergency Room Diagnosis and Treatment of Eye Disease
This is a shared conversation. Sign in to Orris to start your own chat.