Hernia
Reading File
Asking for Preferences
Finding Sources
Searching the Web
hernia types classification management overview 2024
Reading File
Reading File
Reading File
Searching Images
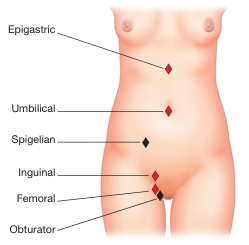
hernia types anatomy diagram inguinal femoral umbilical
Finding Sources
Reading File
Loading Image
Here is a comprehensive overview of hernias:
Hernia — Comprehensive Overview
Definition
A hernia is the protrusion of an organ or tissue through a defect or weakness in the wall that normally contains it. Most hernias involve abdominal contents pushing through weaknesses in the abdominal wall or peritoneum.
Anatomical Classification & Types
Groin Hernias
| Type | Location | Key Features |
|---|---|---|
| Indirect inguinal | Lateral to inferior epigastric vessels, through the deep inguinal ring | Most common overall; follows the processus vaginalis; more common in males |
| Direct inguinal | Medial to inferior epigastric vessels, through Hesselbach's triangle | Acquired weakness; pushes directly through the abdominal wall |
| Femoral | Below inguinal ligament, medial to femoral vein in femoral canal | More common in women; high incarceration rate (~45%) due to small, rigid neck |
| Pantaloon | Combination of direct + indirect | Straddles the inferior epigastric vessels; difficult to reduce manually |
Differentiating direct vs. indirect inguinal hernia clinically: Place the thenar eminence on the ASIS — the index finger points to a direct hernia, the middle finger to an indirect hernia. - Thieme Atlas of Anatomy
Ventral / Abdominal Wall Hernias
| Type | Location | Notes |
|---|---|---|
| Umbilical | Through the fibromuscular umbilical ring | Congenital in infants (often resolves by age 5); acquired in adults with raised intra-abdominal pressure (obesity, ascites, pregnancy) |
| Epigastric | Midline through linea alba, above umbilicus | Usually preperitoneal fat only |
| Incisional | Through a prior surgical scar | Occurs in ~20% of laparotomy patients; recurrence rate 20–50% |
| Spigelian | Through the semilunar line, lateral to rectus muscle | Intramural — often missed on examination |
| Obturator | Through obturator foramen | Rare; "little old lady" hernia; presents with medial thigh pain (Howship–Romberg sign) |
Diaphragmatic / Internal Hernias
| Type | Notes |
|---|---|
| Hiatal (sliding / Type I) | Gastro-oesophageal junction migrates above diaphragm; strongly associated with GERD |
| Paraesophageal (Type II–IV) | Gastric fundus or other organs herniate beside the oesophagus |
| Paraduodenal | Most common congenital internal hernia |
| Post-surgical internal hernia | After Roux-en-Y bypass, colectomy, or Whipple — bowel herniates through mesenteric defects |
| Congenital diaphragmatic hernia (CDH) | Bowel in thorax; neonatal emergency |
Pathophysiology
All hernias result from a combination of increased intra-abdominal pressure and a structural weakness in the containing wall. Predisposing factors include:
- Age, male sex (for inguinal)
- Obesity, chronic cough, straining, heavy lifting
- Previous surgery (incisional hernias)
- Connective tissue disorders
Clinical Spectrum — Reducible → Incarcerated → Strangulated
| State | Definition | Management |
|---|---|---|
| Reducible | Contents can be returned spontaneously or manually | Elective repair |
| Incarcerated | Contents are trapped; cannot reduce | Urgent; manual reduction may be attempted if no strangulation |
| Strangulated | Ischaemia of trapped contents (bowel/omentum) | Surgical emergency |
Strangulation risk is inversely related to the size of the hernia neck. Femoral hernias strangulate in up to 40% of cases at first presentation; incisional hernias in only ~2%. Umbilical hernias account for ~15% of emergency hernia surgery, with up to 60% showing strangulation at operation. — Sleisenger & Fordtran's GI & Liver Disease
Richter hernia: Only part of the bowel wall is trapped, so complete obstruction may be absent even with strangulation — a diagnostic trap, most often with femoral or inguinal hernias.
Hiatal Hernia & GERD
Hiatal hernia is present in 54–94% of patients with reflux oesophagitis. It promotes reflux by:
- Displacing the LES above the diaphragm → reduces basal LES pressure
- Creating a persistent acid pocket in the hernia sac
- Increasing transient LES relaxation (tLESR) frequency
- Abolishing the pressure augmentation normally provided by crural diaphragm contraction
Large (≥3 cm), non-reducible hiatal hernias are particularly prone to severe GERD and are associated with Barrett's oesophagus and oesophageal adenocarcinoma. — Sleisenger & Fordtran's GI & Liver Disease
Diagnosis
- Physical examination: visible or palpable bulge, cough impulse, reducibility
- Ultrasound: useful for groin hernias, especially in obese patients
- CT scan: gold standard for internal hernias, incarcerated hernias, and complex cases; differentiates hernia type and assesses bowel viability
- Endoscopy / barium swallow: for hiatal hernia
Management
Watchful Waiting
Acceptable for asymptomatic inguinal hernias in older or unfit patients, as annual risk of acute incarceration is low (~0.2%/year).
Surgery
Surgery is the definitive treatment. Urgency is dictated by the clinical state:
Elective repair principles:
- Tissue repair (e.g., Shouldice, Bassini): primary suture repair of the defect; higher recurrence than mesh
- Mesh repair (e.g., Lichtenstein): tension-free; gold standard for most adult inguinal hernias; significantly lower recurrence rates
- Laparoscopic approaches:
- TAPP (Transabdominal Preperitoneal): mesh placed in preperitoneal space via peritoneal flap
- TEP (Totally Extraperitoneal): mesh placed without entering peritoneal cavity
Emergency repair (incarceration/strangulation):
- Quick resuscitation, IV antibiotics, urgent OR
- Assess bowel viability; resect if non-viable
- Mesh use is controversial in contaminated fields — open tissue repair is preferred initially; mesh repair reserved for subsequent elective repair if needed. — Mulholland & Greenfield's Surgery
Pediatric Considerations
High incidence of indirect inguinal hernia in infants (due to patent processus vaginalis) — treated with high ligation without mesh. Umbilical hernias in children usually resolve spontaneously by age 5; surgery if persistent, >2 cm, or complicated.
Key Associations to Remember
| Hernia | Classic Association |
|---|---|
| Femoral | Middle-aged woman, high strangulation risk |
| Richter | Partial bowel wall trap; no complete obstruction |
| Obturator | Elderly thin woman; Howship–Romberg sign |
| Spigelian | Interparietal / intramural; easy to miss |
| Pantaloon | Direct + indirect combined |
| Hiatal | GERD, Barrett's, adenocarcinoma |
| CDH | Neonatal respiratory distress (Bochdalek most common) |
Sources: Mulholland & Greenfield's Surgery 7e; Sleisenger & Fordtran's GI & Liver Disease; Roberts & Hedges' Clinical Procedures in Emergency Medicine; Bailey & Love's Short Practice of Surgery 28e; Thieme Atlas of Anatomy; Schwartz's Principles of Surgery 11e
Explain the surgical repair techniques (mesh vs. tissue) in detail
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Searching Images
Lichtenstein hernia mesh repair technique surgical steps
Reading File
Reading File
Searching PubMed
hernia repair mesh versus tissue recurrence chronic pain
Loading Image
Reading Article
PMID: 38963034
Reading File
Reading File
Searching Images
TEP totally extraperitoneal laparoscopic hernia repair preperitoneal space steps
Loading Image
Reading File
The answer above covers all major repair techniques in depth. Here's a quick orientation to the structure:
Tissue repairs (4 techniques):
- Bassini — historic 3-layer; largely abandoned
- Shouldice — 4-layer running suture; best tissue repair; ~1% recurrence in expert hands; but 3.65× higher recurrence than mesh
- McVay — uses Cooper's ligament; uniquely repairs femoral defects; requires relaxing incision
- Desarda — autologous external oblique patch; good for mesh-free scenarios
Open mesh repairs (3 techniques):
- Lichtenstein — global gold standard; 0.2% recurrence; short learning curve; EHS-recommended
- Plug & Patch — 3D plug + flat mesh; equivalent outcomes to Lichtenstein but ~6% plug migration risk limits its use
- Rives-Stoppa — giant preperitoneal mesh; best for recurrent/bilateral/large defects
Minimally invasive repairs:
- TAPP — enters peritoneum; easier to learn; can inspect contralateral side
- TEP — stays extraperitoneal; lower visceral injury risk; steeper learning curve (~100 cases)
- eTEP / Robotic — emerging; expanding operative space; equivalent outcomes
The key clinical takeaway: mesh reduces recurrence by ~63% vs. tissue (OR 0.37). For open repair, Lichtenstein is preferred. For bilateral or recurrent hernias after prior anterior repair, laparoscopic TAPP/TEP is preferred. Tissue repair remains essential when mesh is contraindicated (contamination, strangulation).
This is a shared conversation. Sign in to Orris to start your own chat.