Nephrotic syndrome
Reading File
Finding Sources
Searching PubMed
"nephrotic syndrome"[MeSH Terms] AND management
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Reading File
I now have all the information needed for a comprehensive answer. Let me compile it.
Nephrotic Syndrome
Definition
Nephrotic syndrome is defined by the triad of:
- Heavy proteinuria (>3.5 g/day in adults; >40 mg/m²/hr in children)
- Hypoalbuminemia (serum albumin typically <3.0 g/dL, often <2.5 g/dL)
- Edema
Associated findings include hyperlipidemia (total cholesterol usually >180 mg/dL) and lipiduria. Hematuria is typically absent or minimal, distinguishing it from nephritic syndrome.
- Tietz Textbook of Laboratory Medicine, 7th Edition
- Comprehensive Clinical Nephrology, 7th Edition
Pathophysiology
The common thread across all causes is podocyte injury - damage to the specialized visceral epithelial cells of the glomerulus. This disrupts the glomerular filtration barrier in two ways:
- Loss of the charge-selective property of the glomerular basement membrane (GBM)
- Disruption of slit diaphragm proteins (nephrin, podocin, CD2AP) in the interdigitating foot processes of podocytes
The result: massive protein leak into the urine.
Scanning electron microscopy showing normal podocyte foot processes (left) vs. complete foot process effacement in nephrotic syndrome (right):
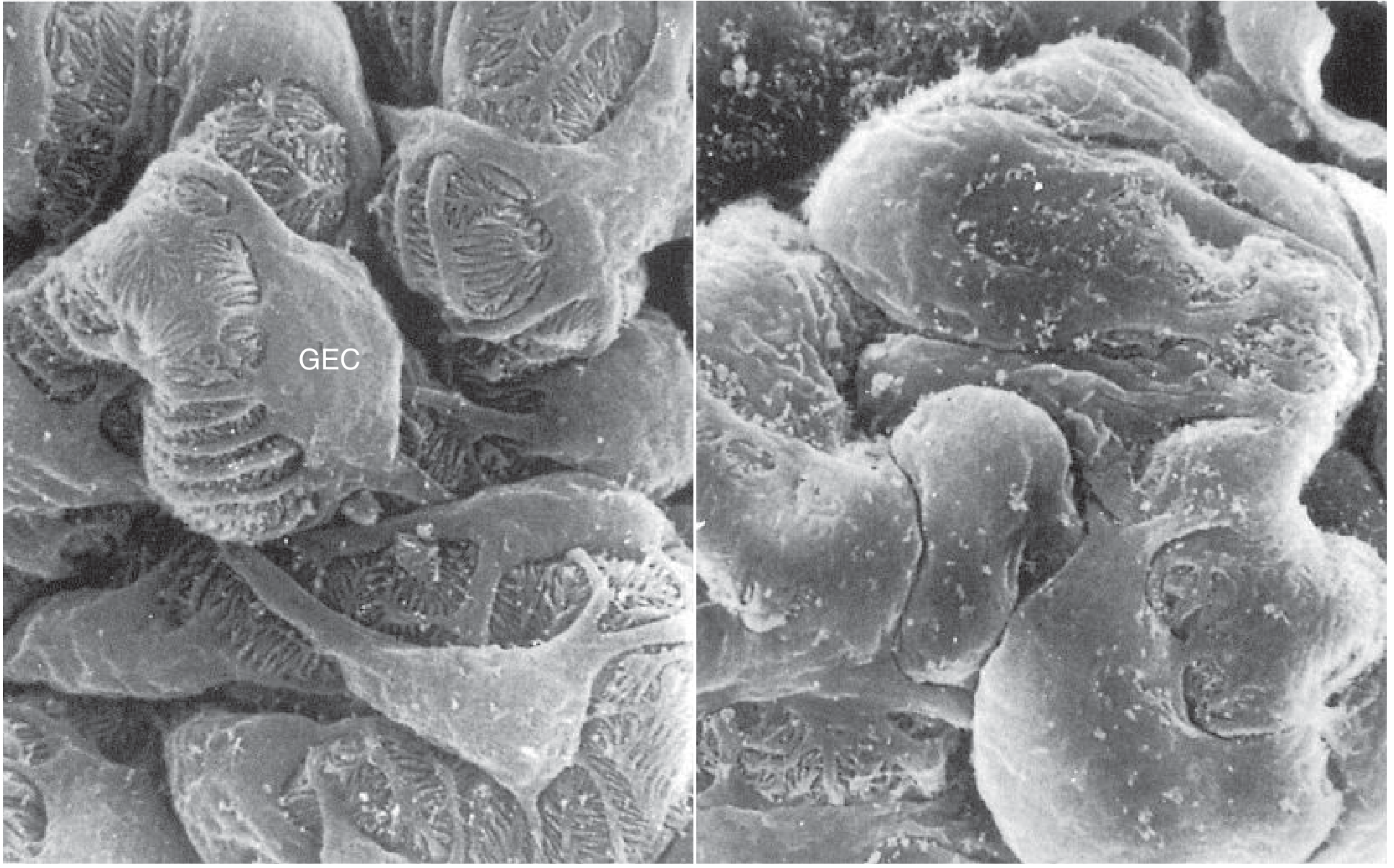
Fig. 49.17 - Tietz Textbook of Laboratory Medicine
Mechanism of Edema
Two competing theories explain nephrotic edema:
1. Underfill hypothesis (classic): Hypoalbuminemia → reduced oncotic pressure → fluid transudation into interstitium → contracted blood volume → RAAS activation → aldosterone-mediated Na+ retention (worsening edema). Seen classically in minimal change disease.
2. Overfill hypothesis (more common): Primary defect in distal nephron Na+ excretion (likely via ENaC activation by proteolytic enzymes leaking into the tubule) → Na+ and water retention independent of volume status. Plasma volume is expanded and RAAS is suppressed.
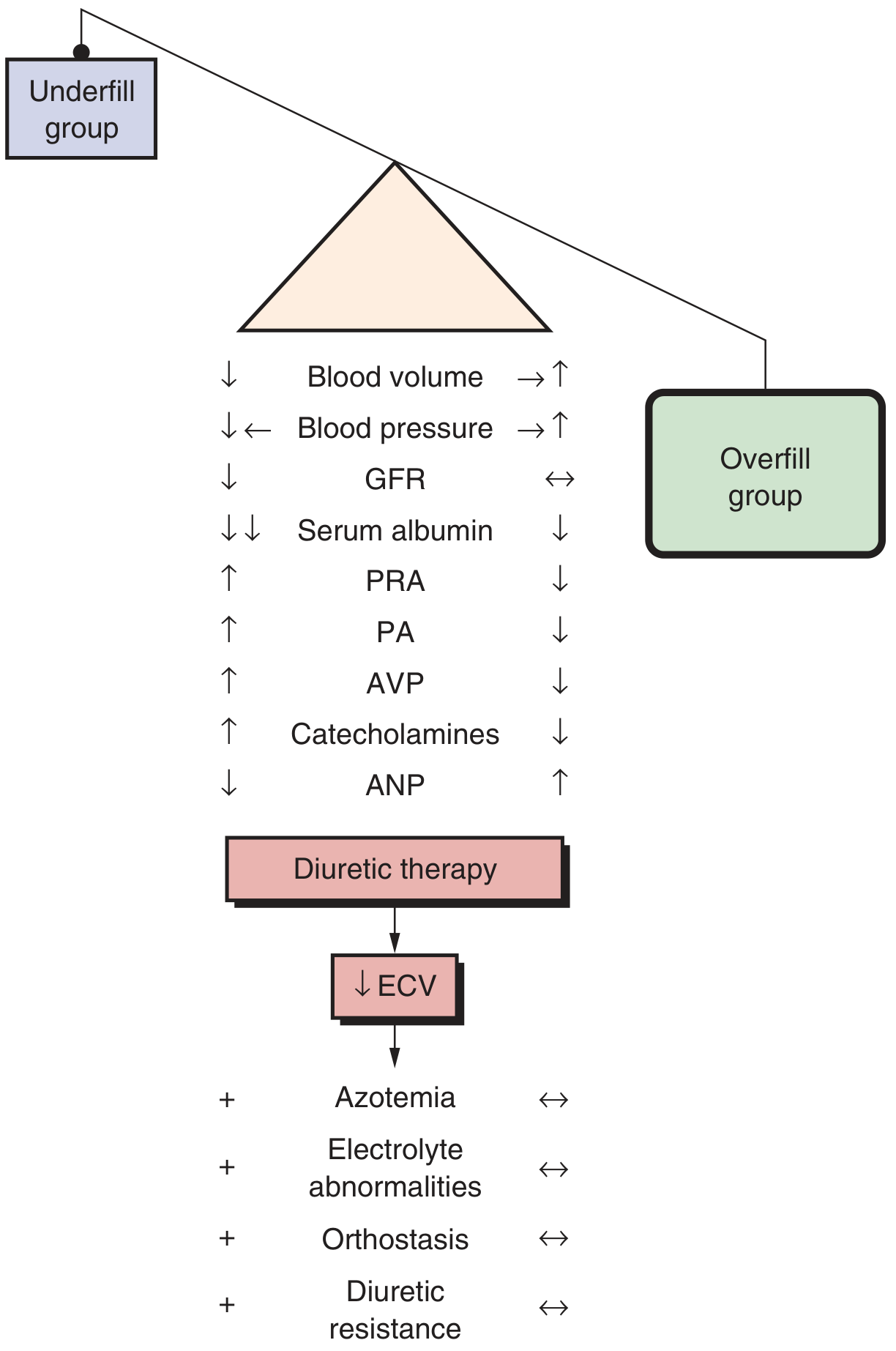
Fig. 50.17 - Brenner and Rector's The Kidney
Causes
Primary (Idiopathic) Glomerular Diseases
| Disease | Key Features | Age Group |
|---|---|---|
| Minimal Change Disease (MCD) | Most common cause in children; autoantibodies vs. nephrin; steroid-responsive; normal LM, foot process effacement on EM | Children (80%), adults (peak 50-60 yrs) |
| Focal Segmental Glomerulosclerosis (FSGS) | Most common cause in adults (esp. African Americans); focal/segmental capillary obliteration; often steroid-resistant; may progress to ESKD | Adults > Children |
| Membranous Nephropathy (MN) | Autoimmune (anti-PLA2R antibodies against podocytes); granular subepithelial deposits; GBM thickening; often steroid-resistant | Adults |
| MPGN | Immune complex deposition in mesangium and capillary walls; may be mixed nephrotic/nephritic | Any age |
Secondary Causes
Systemic diseases:
- Diabetes mellitus (most common secondary cause globally)
- SLE (lupus nephritis class V)
- Amyloidosis (AL or AA)
- Multiple myeloma
Infections:
- Bacterial: post-streptococcal GN, syphilis, leprosy, infective endocarditis
- Viral: Hepatitis B, Hepatitis C, HIV (collapsing FSGS), CMV, EBV
- Parasitic: malaria (quartan), schistosomiasis, filariasis, toxoplasmosis
Medications/Chemicals:
- Mercury, gold, penicillamine
- NSAIDs (MCD pattern)
- Heroin (FSGS)
- Lithium, captopril, pamidronate
Neoplasms:
- Hodgkin lymphoma (associated with MCD)
- Solid tumors, leukemias
Hereditary/Genetic:
- Congenital nephrotic syndrome (Finnish type - nephrin mutation)
- Podocin mutation (NPHS2), WT1 mutation (Denys-Drash syndrome)
- Alport syndrome, Fabry disease, nail-patella syndrome
Brenner and Rector's The Kidney, 2-Volume Set
Lab Findings
| Test | Finding |
|---|---|
| Urine protein | >3.5 g/day (or urine protein:creatinine ratio >3.5) |
| Urine microscopy | Oval fat bodies, fatty casts, lipiduria ("Maltese cross" under polarized light) |
| Serum albumin | <3.0 g/dL |
| Serum cholesterol | Elevated (often >250-300 mg/dL) |
| Triglycerides | Elevated |
| Serum creatinine | Variable |
| Serum complement | Normal in MCD/FSGS/MN; low in MPGN, lupus, post-infectious GN |
Hypoalbuminemia causes compensatory hepatic protein synthesis. Large proteins (fibrinogen, VWF, clotting factors V, VII) increase; small proteins (antithrombin III, factors IX/X/XI/XII) are lost in urine or reduced.
Complications
1. Thromboembolism (10-40% of patients)
The hypercoagulable state results from the imbalance in coagulation proteins shown below:
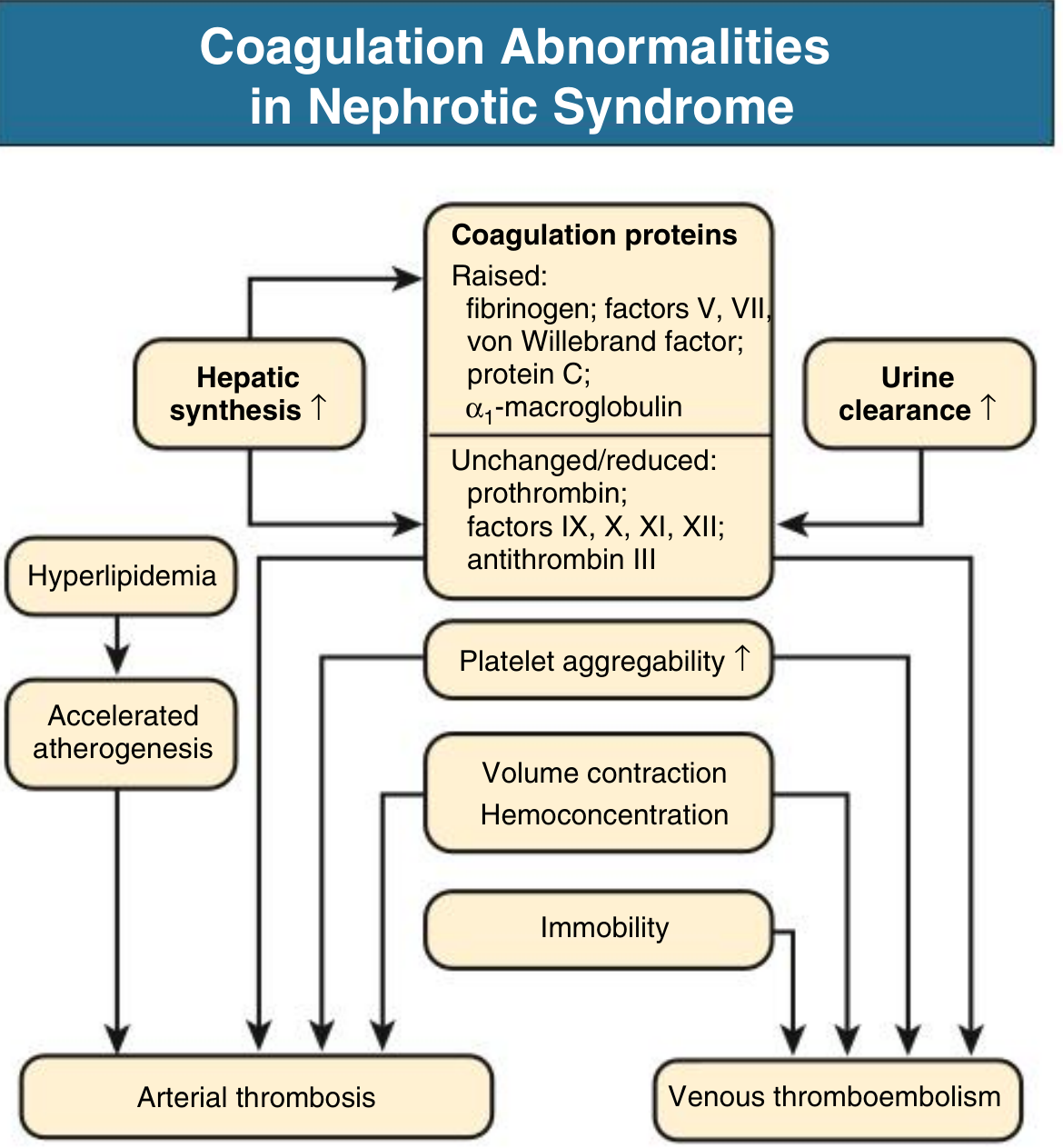
Fig. 16.10 - Comprehensive Clinical Nephrology, 7th Edition
- Raised: fibrinogen, factors V and VII, VWF, protein C, alpha-1 macroglobulin (due to increased hepatic synthesis)
- Reduced/lost: antithrombin III, factors IX, X, XI, XII (urinary loss)
- Increased platelet aggregability
- Clinical: deep vein thrombosis, renal vein thrombosis (especially in membranous nephropathy), pulmonary embolism, arterial thrombosis
2. Infection
- Loss of immunoglobulins (IgG) in urine → susceptibility to encapsulated organisms (Streptococcus pneumoniae, Haemophilus influenzae)
- Peritonitis (especially in children), cellulitis
- Urinary loss of complement factor B impairs alternative pathway opsonization
3. Hyperlipidemia and Accelerated Atherosclerosis
- Increased hepatic VLDL synthesis (compensatory response to low oncotic pressure)
- Reduced catabolism of lipoproteins (urinary loss of lipoprotein lipase)
- Raised total cholesterol, LDL, triglycerides, VLDL
4. Acute Kidney Injury
Causes include:
- Acute tubular necrosis (especially in MCD, patients >50 years)
- Interstitial nephritis (NSAID-induced MCD)
- Renal vein thrombosis
- Tubular injury in collapsing FSGS
5. Other
- Muehrcke's lines (white bands in nails) - sign of hypoalbuminemia
- Malnutrition
- Hypothyroidism (urinary loss of thyroid-binding globulin and T4)
- Vitamin D deficiency (urinary loss of vitamin D-binding protein)
- Drug toxicity (altered binding of drugs to hypoalbuminemia, e.g., furosemide resistance)
Management
General Principles
| Intervention | Rationale |
|---|---|
| Low-sodium diet | Reduce edema |
| Protein 0.8-1.0 g/kg/day | Balance nitrogen losses without worsening proteinuria |
| Loop diuretics (furosemide) | First-line for edema; may need higher doses due to hypoalbuminemia-related altered pharmacokinetics |
| ACE inhibitors / ARBs | Reduce intraglomerular pressure and proteinuria; first-line antiproteinuric therapy |
| Statins | Treat hyperlipidemia; reduce cardiovascular risk |
| Anticoagulation | Prophylactic if albumin <2.0-2.5 g/dL with additional risk factors; therapeutic for documented DVT/PE/renal vein thrombosis (heparin then oral anticoagulant) |
| Infection vigilance | Pneumococcal vaccination; early antibiotic treatment |
| BP control | Target <130/80 mmHg with RAAS blockade |
Immunosuppressive Therapy (Cause-Specific)
| Disease | First Line | Second Line |
|---|---|---|
| MCD | Prednisolone (high dose for 8-12 weeks) - ~90% respond | Cyclophosphamide, cyclosporine, tacrolimus for relapses; rituximab for steroid-dependent/refractory |
| FSGS (primary) | Corticosteroids | Calcineurin inhibitors (tacrolimus/cyclosporine), mycophenolate mofetil |
| Membranous nephropathy | Rituximab (anti-CD20, targets PLA2R-Ab-producing B cells) | Cyclophosphamide + alternating steroids (Ponticelli regimen) |
| Lupus nephritis class V | Mycophenolate mofetil + steroids | Azathioprine for maintenance |
| Amyloidosis | Treat underlying disease; melphalan + dexamethasone (AL type) | - |
Note on steroid response in MCD: around 60% of steroid-responsive patients experience multiple relapses. Cyclophosphamide is limited to 8-12 weeks to reduce gonadal toxicity risk. Rituximab has shown promise in steroid-dependent childhood nephrotic syndrome per a 2025 Cochrane systematic review.
- Washington Manual of Medical Therapeutics
- Tietz Textbook of Laboratory Medicine, 7th Edition
- Comprehensive Clinical Nephrology, 7th Edition
When to Biopsy
Kidney biopsy is generally indicated in all adults presenting with nephrotic syndrome to guide therapy. In children, an empirical trial of corticosteroids is standard first (given the high prevalence of MCD); biopsy is reserved for steroid-resistant or atypical cases.
Recent Evidence Update
A 2025 Cochrane meta-analysis (PMID 40337980) on steroid-resistant nephrotic syndrome in children evaluated interventions for idiopathic cases. A 2026 systematic review (PMID 41843217) highlighted rituximab-induced hypogammaglobulinemia as a significant complication requiring monitoring in children treated with rituximab - a consideration when choosing this agent for steroid-dependent cases.
This is a shared conversation. Sign in to Orris to start your own chat.