Ectopic thyroid tissue
Reading File
Finding Sources
Finding Sources
Searching PubMed
"ectopic thyroid"[MeSH Terms]
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Loading Image
Reading File
I now have comprehensive, well-sourced material and excellent diagrams. Let me compile the full answer.
Ectopic Thyroid Tissue
Embryological Basis
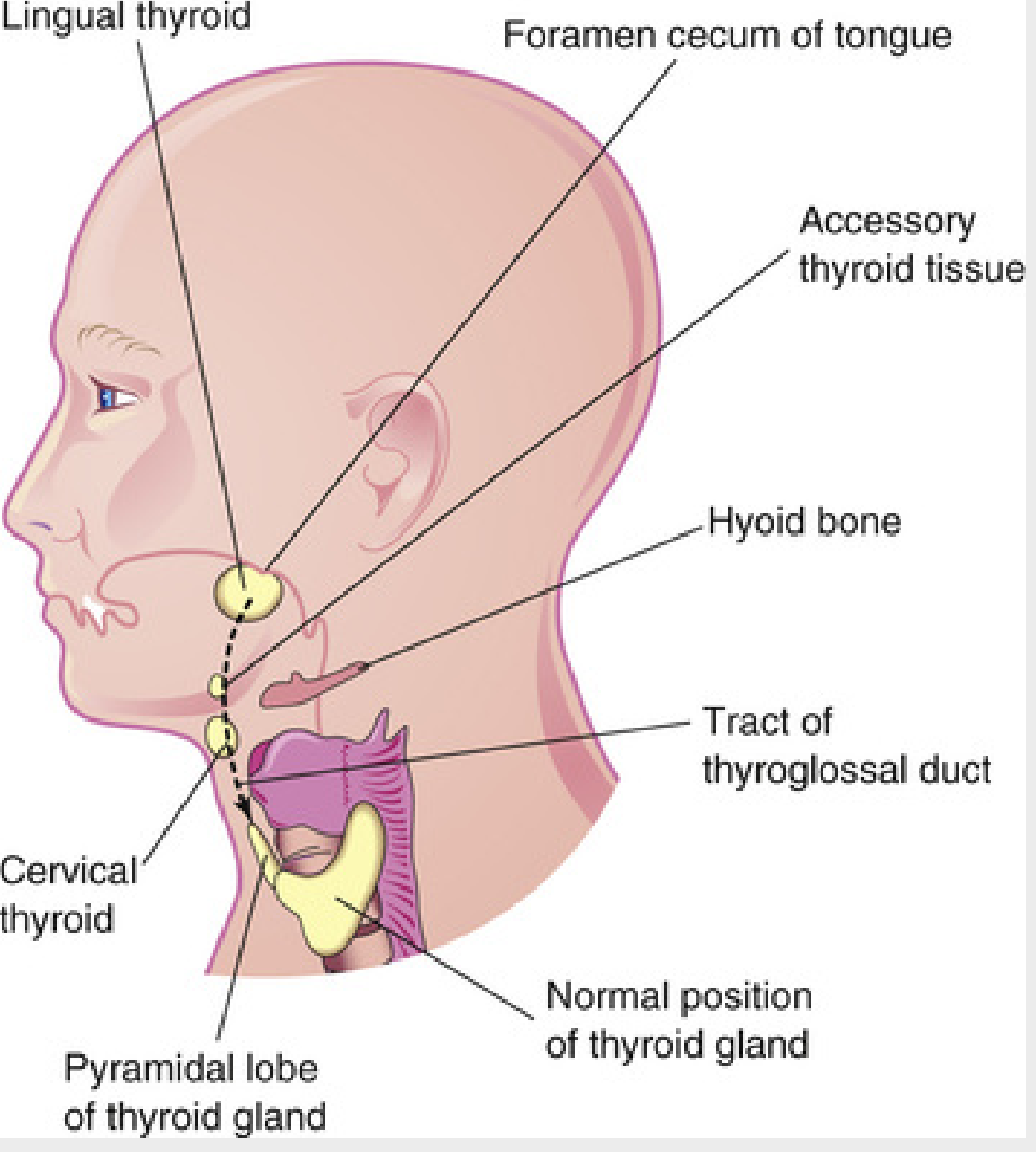
The thyroid gland originates from the floor of the primitive pharynx during the third week of gestation, at the site of the foramen cecum at the base of the tongue. It then migrates caudally along the thyroglossal duct to its final pretracheal position in the lower neck. Ectopic thyroid results from failure or arrest of this descent at any point along this path.
The transcription factors TTF-1, TTF-2, NKX2-1, FOXE1, and PAX8 orchestrate thyroid gland development; mutations in these genes can cause thyroid dysgenesis, including ectopic positioning.
- Harrison's Principles of Internal Medicine 22E, p. 3064
- The Developing Human (Clinically Oriented Embryology), p. 498
Locations
Ectopic thyroid can occur anywhere along the thyroglossal duct tract - from the foramen cecum down to the anterior mediastinum. A second pathway (the thyrothymic tract, from the 3rd pharyngeal pouch) extends inferiorly to the mediastinum.
Usual sites of ectopic thyroid tissue along the path of the thyroglossal duct. - The Developing Human, p. 498
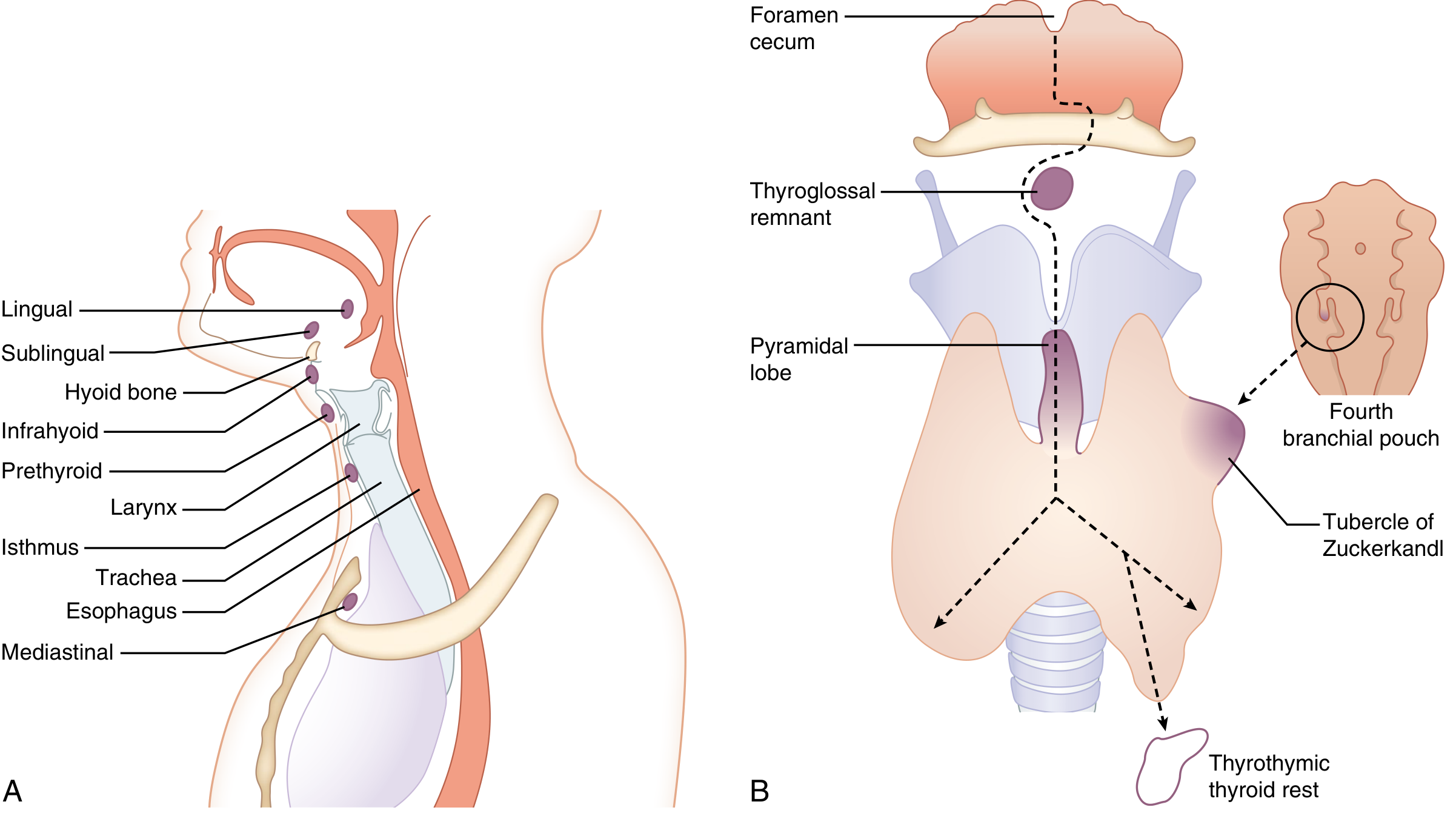
(A) Common sites for midline ectopic thyroid masses (lingual, sublingual, infrahyoid, prethyroid, isthmus, mediastinal). (B) Major medial and lateral embryological elements including thyrothymic thyroid rests. - Sabiston Textbook of Surgery, p. 1486
Named Locations
| Site | Notes |
|---|---|
| Lingual thyroid | Most common ectopic location; at the base of the tongue at the foramen cecum; found in up to 10% of autopsies, clinically relevant in 1/4000 |
| Sublingual thyroid | Appears high in the neck at or just inferior to the hyoid bone due to incomplete descent |
| Infrahyoid / Prethyroid | Along the midline of the neck |
| Thyroglossal duct remnant | Thyroid tissue within a persistent thyroglossal duct cyst |
| Intrathoracic / Mediastinal | Arise from thyroid rests along the thyrothymic tract; can enlarge to form primary intrathoracic goiters |
| Struma ovarii | Ectopic thyroid tissue comprising >50% of an ovarian teratoma; rare; can be benign or malignant |
Key Clinical Points
1. Lingual Thyroid
- Presents as a midline mass at the base of the tongue.
- Often the only thyroid tissue present - in ~70% of ectopic sublingual thyroid cases, no other thyroid tissue exists in the normal cervical position.
- Can enlarge due to inadequate thyroid hormone production (compensatory TSH stimulation), causing dysphagia, dysphonia, or airway obstruction.
- Surgical excision may be necessary for compressive symptoms.
2. Sublingual Thyroid
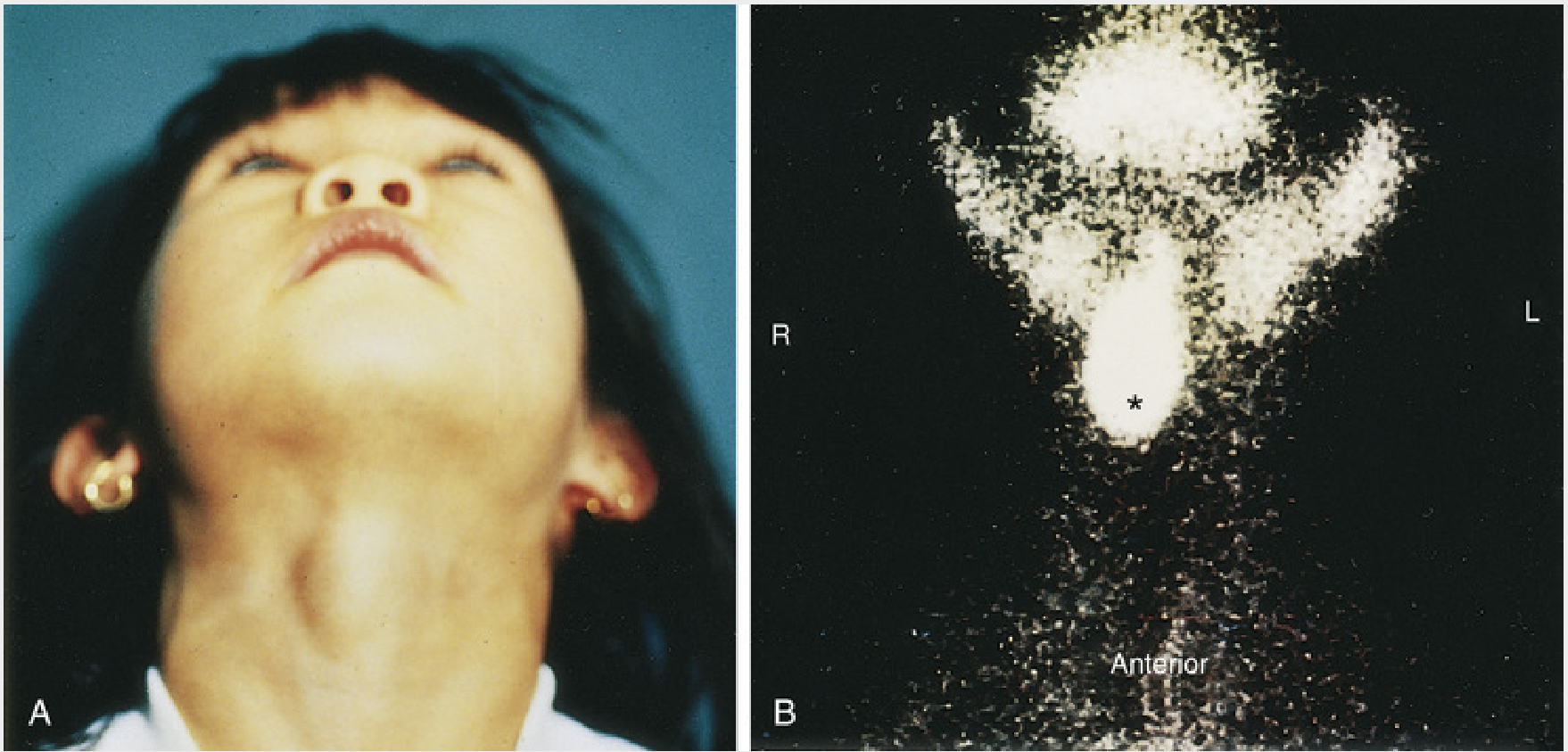
A sublingual thyroid mass in a child. Tc-99m scintigraphy confirms ectopic sublingual thyroid (asterisk) with no functioning thyroid in the normal anterior neck position. - The Developing Human, p. 499
3. Thyroid Rests (Thyrothymic Tract)
- Foci of thyroid tissue along the path of thymic descent; found in up to 50% of people and generally not pathological.
- May be mistaken for pathologic lymph nodes or parathyroid glands.
- Can be connected to the main gland by a thin stalk or exist as completely separate structures.
- Enlargement of intrathoracic rests gives rise to primary intrathoracic goiters.
4. Struma Ovarii
- Part of an ovarian teratoma; can produce thyroid hormone and cause thyrotoxicosis with low radioiodine uptake in the neck.
- Listed alongside thyrotoxicosis factitia and iodine excess as a cause of thyrotoxicosis with low/absent thyroidal radionuclide uptake on scan.
Diagnosis
- Ultrasound is the first-line investigation, especially to confirm the absence of normal cervical thyroid tissue.
- Tc-99m pertechnetate scintigraphy confirms functional ectopic tissue and is essential before any surgical excision to avoid removing the patient's only functioning thyroid tissue.
- CT/MRI for deeper or mediastinal locations.
Critical point: It is essential to differentiate ectopic thyroid from a thyroglossal duct cyst before surgery. Inadvertent removal of the only functioning thyroid tissue will render the patient permanently hypothyroid and dependent on lifelong thyroid hormone replacement.
Complications and Associations
- Congenital hypothyroidism - ectopic thyroid is a leading cause; ectopic glands are often insufficient producers of thyroid hormone, triggering compensatory goitrous enlargement under elevated TSH.
- Malignant transformation - thyroid cancers (papillary carcinoma most common) can arise in ectopic thyroid tissue including lingual thyroid and struma ovarii.
- Thyrotoxicosis - rarely, from hyperfunctioning ectopic tissue (struma ovarii, functional teratomas).
Sources:
- The Developing Human: Clinically Oriented Embryology, pp. 498-499
- Sabiston Textbook of Surgery, pp. 1485-1486
- Harrison's Principles of Internal Medicine, 22E, p. 3064
- Cummings Otolaryngology, Head and Neck Surgery
- Mulholland and Greenfield's Surgery, 7th ed.
Retrosternal goiter
Finding Sources
Finding Sources
Searching PubMed
"retrosternal goiter" AND surgery
Finding Sources
Finding Sources
Reading Article
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive material. Let me compile the complete answer.
Retrosternal Goiter
Also called substernal, intrathoracic, or diving goiter - these are terms used interchangeably, though "retrosternal" strictly refers to goiters behind the sternum while "intrathoracic" denotes at least 50% of thyroid tissue located below the thoracic inlet. It affects less than 1% of all goiter patients.
Classification
1. Secondary (Cervical Extension) - ~99%
The vast majority arise from downward extension of a cervical multinodular goiter along the fascial planes of the neck, drawn by gravity and negative intrathoracic pressure. These maintain their blood supply from the superior and inferior thyroid arteries (cervical vessels).
2. Primary (True Intrathoracic) - ~1%
Arise from ectopic accessory thyroid tissue within the chest, with no connection to cervical thyroid. They are supplied by intrathoracic blood vessels (internal mammary, innominate, or aortic branches). These are more likely to require a thoracic approach.
- Schwartz's Principles of Surgery, 11th ed. | Sabiston Textbook of Surgery
Clinical Presentation
About 40% can be asymptomatic, presenting as an incidental finding on chest X-ray or CT.
When symptomatic:
| Symptom | Mechanism |
|---|---|
| Dyspnea / airway obstruction | Tracheal compression (most common; acute distress in up to 20%) |
| Dysphagia | Esophageal compression |
| Stridor | Fixed tracheal narrowing (worse on exertion) |
| Hoarseness | Recurrent laryngeal nerve compression |
| SVC syndrome | Venous distension of neck/chest wall, facial oedema, plethora, cyanosis, papilloedema |
| Horner's syndrome | Sympathetic chain compression |
| Chylothorax | Thoracic duct compression |
| TIAs | Thyrocervical steal |
Pemberton's Sign
Raising both arms above the head causes facial congestion, cyanosis, and respiratory distress due to functional obstruction of the thoracic inlet by the goiter. This is a classic clinical sign of increased thoracic inlet pressure.
- Scott-Brown's Otorhinolaryngology, Head & Neck Surgery, p. 868
Investigations
Chest X-Ray
The classic finding is a superior mediastinal mass with tracheal deviation or compression, often discovered incidentally.
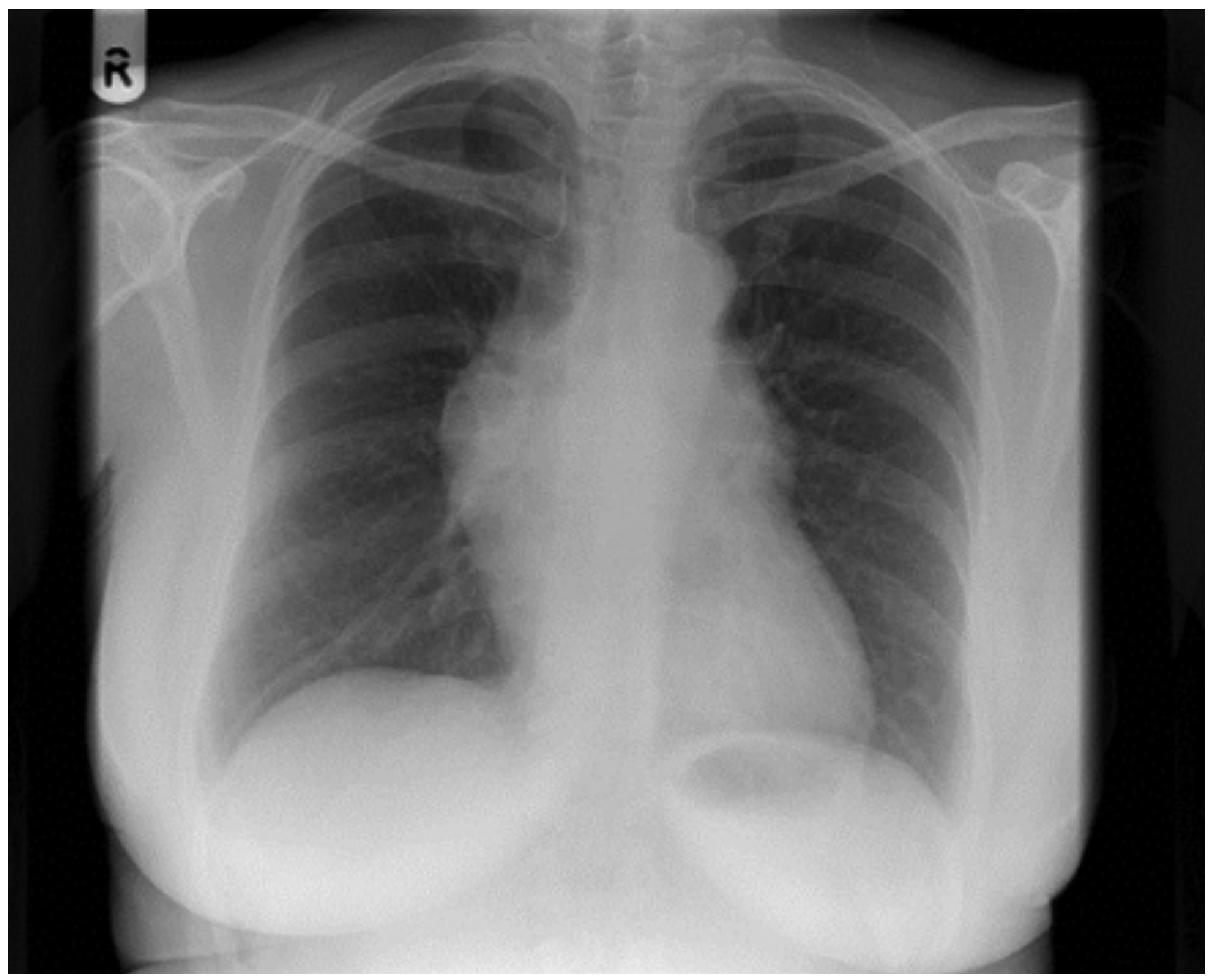
CXR: incidental finding of a mediastinal mass due to primary intrathoracic goiter. - Scott-Brown's, p. 868
CT Scan (Investigation of Choice)
The most important preoperative investigation. Key features to document:
- Full inferior extent of the intrathoracic component (scan from skull base to carina)
- Mediastinal compartment - anterior vs. posterior (posterior location increases the chance of lateral thoracotomy)
- Tracheal deviation and compression - degree and level
- Relationship to great vessels (innominate, SVC, aortic arch)
- Evidence of malignancy (extracapsular extension)
CT findings that predict sternotomy: extension below the aortic arch, evidence of extra-thyroid extension suggesting malignancy, posterior mediastinal location, or primary intrathoracic goiter.
For substernal goiter evaluation, non-contrast CT is sufficient. IV contrast is added only if malignancy is suspected.
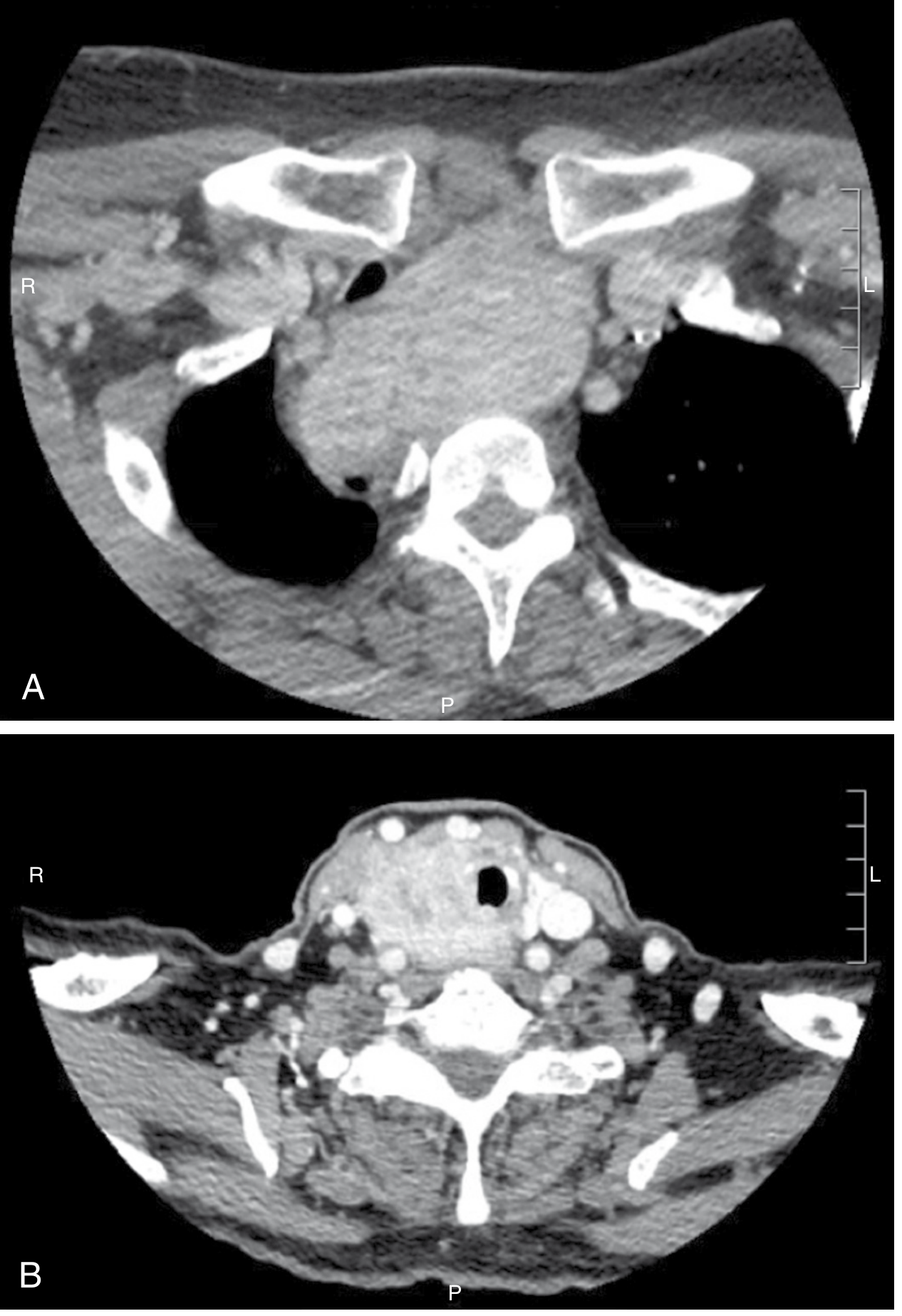
CT scan: (A) Left-sided substernal goiter extending into the posterior mediastinum with tracheal compression and deviation. (B) Contrast CT showing locally advanced follicular thyroid cancer with tracheal wall and esophageal invasion. - Sabiston Textbook of Surgery, p. 1494
Thyroid Function Tests
- Majority are euthyroid (80%)
- Up to 30% may have subclinical thyrotoxicosis (suppressed TSH with normal T3/T4)
- Overt hyperthyroidism is less common
Ultrasound
Cannot evaluate the intrathoracic component. Useful only for cervical thyroid morphology.
Scintigraphy
- Plays no role in the preoperative evaluation of biochemically euthyroid patients
- Intrathoracic goiters often demonstrate limited iodine avidity despite large size
- May be useful when ectopic functioning tissue is suspected as a cause of thyrotoxicosis
Pulmonary Function Tests
Objective assessment of respiratory compromise - flow-volume loops may demonstrate a fixed extrathoracic or variable intrathoracic obstruction pattern.
Risk of Malignancy
Reported in up to 11% of goiters with intrathoracic extension - FNA where accessible.
Management
Indications for Surgery
- Significant airway compression
- Symptomatic patients (dysphagia, dyspnoea)
- Young patients in whom symptoms are likely to develop
- Suspected or confirmed malignancy
In elderly patients with incidentally discovered retrosternal goiters and no symptoms, most surgeons favour observation rather than prophylactic surgery, balancing operative risk against benefit.
Surgical Approach
Transcervical (Collar) Incision - >95% of cases
The standard and most common approach. Key steps:
- Ligate and divide superior pole vessels and middle thyroid veins first
- Divide the isthmus early to allow independent mobilization of each lobe
- Blunt finger dissection along the thyroid capsule to free fascial attachments
- Large 1-0 or 2-0 sutures placed deep into the goiter to facilitate traction and delivery through the neck
- Ligamentous tissue between the sternal heads of the clavicles may be gently divided to increase the opening
Median Sternotomy - Indications (~5%)
Required in:
- Invasive thyroid malignancy
- Previous thyroid surgery (risk of parasitic mediastinal vessels from prior operations)
- Primary intrathoracic goiter with no cervical thyroid tissue
- Posterior mediastinal extension (may require lateral thoracotomy instead)
- Goiter too large to deliver through the cervical incision
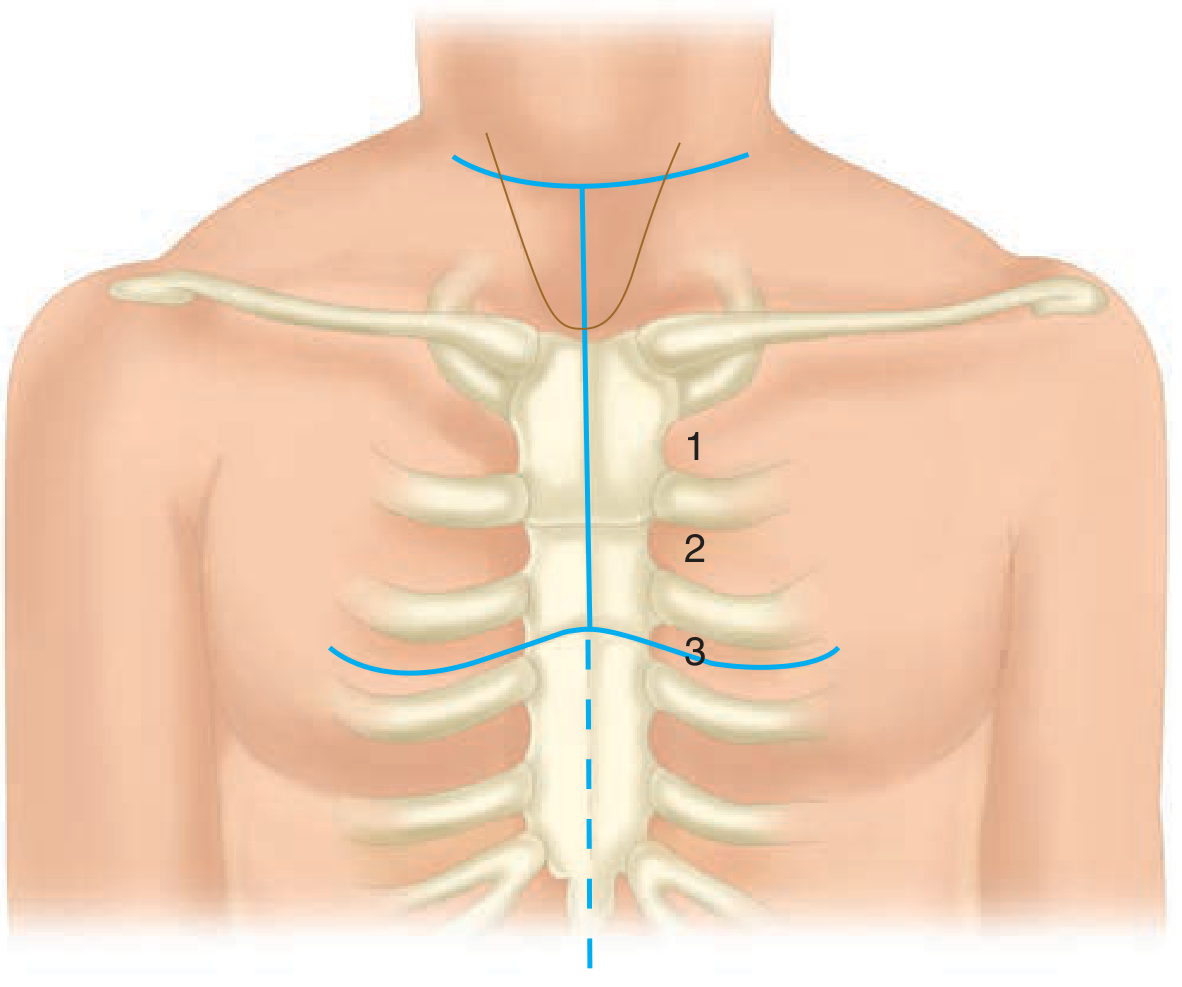
Incisions for partial sternotomy: collar incision combined with midline sternal division to the 3rd intercostal space, then laterally at the 3rd-4th intercostal space. - Schwartz's Principles of Surgery
The chest should be prepared and draped in all cases of substernal goiter surgery in the event emergency sternotomy is needed to control mediastinal bleeding or remove an unexpectedly invasive cancer.
Complications of Surgery
- Recurrent laryngeal nerve injury - risk is increased due to altered anatomy and limited visibility
- Hypoparathyroidism - parathyroids may be adherent or displaced
- Tracheomalacia - softening of tracheal rings from chronic compression; may cause airway collapse post-extubation ("tracheal kiss") - requires awake extubation planning
- Mediastinal haemorrhage
- Chylothorax
Recent Evidence (2025)
A 2025 systematic review (Miani et al., Acta Otorhinolaryngol Ital, PMID: 40567093) covering 93 articles confirms that transcervical excision remains the most common approach for intrathoracic goiters, while transthoracic approaches must always be planned for. Surgery should be performed at specialist centres with experienced multidisciplinary teams to minimize complications.
A concurrent 2025 systematic review and meta-analysis (Alqutub et al., J Surg Res, PMID: 40850248) specifically examined predictors of sternotomy in substernal goiter - the key factors identified include posterior mediastinal extension, primary intrathoracic location, prior neck surgery, and goiter extension below the aortic arch.
Sources:
- Sabiston Textbook of Surgery, pp. 1485-1494
- Schwartz's Principles of Surgery, 11th ed., pp. 1083-1092
- Bailey and Love's Short Practice of Surgery, 28th ed., pp. 882, 5211-5224
- Scott-Brown's Otorhinolaryngology, Head & Neck Surgery, pp. 867-869
- Cummings Otolaryngology, Head and Neck Surgery, p. 220
Thyroid swelling or case btao pura cover the viva qsn
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
I have enough from what I've already retrieved - S Das classification and clinical details (lines 3339-3735), plus the Sabiston and Bailey & Love material from earlier sessions. Let me now compile a comprehensive viva-format answer using all the textbook content collected.
Thyroid Swelling - Complete Surgical Viva Guide
1. HOW DO YOU RECOGNIZE A THYROID SWELLING?
"A thyroid swelling is recognized by its position, its shape, and by the fact that it moves upwards during deglutition."
- S Das, A Manual on Clinical Surgery
Why does it move on swallowing? Because the thyroid gland is enclosed within the pretracheal fascia, which is attached to the larynx and trachea - these structures move upward during swallowing, carrying the thyroid with them.
Exception (viva trap): Very large, fixed malignant thyroid masses may NOT move on swallowing because they have infiltrated surrounding structures.
Other swellings that move on swallowing: Thyroglossal cyst, subhyoid bursitis. Malignant/tuberculous lymph nodes fixed to trachea may also move.
Thyroglossal cyst vs thyroid swelling: A thyroglossal cyst moves up additionally when the tongue is protruded (because of its attachment to the foramen cecum via the thyroglossal tract). A thyroid swelling does NOT move on tongue protrusion.
2. CLASSIFICATION OF THYROID SWELLINGS (Das Classification)
(a) Non-toxic (Simple) Goitre
- Diffuse parenchymatous (hyperplastic)
- Colloid goitre
- Multinodular goitre
- Solitary nodular goitre
(b) Toxic Goitre
- Diffuse toxic - Graves' Disease (Primary thyrotoxicosis)
- Toxic multinodular goitre (Secondary thyrotoxicosis)
- Toxic adenoma (Plummer's disease - Tertiary/solitary toxic nodule)
(c) Neoplastic
- Benign - Follicular adenoma
- Malignant - Papillary, Follicular, Medullary, Anaplastic, Lymphoma
(d) Thyroiditis
- Acute bacterial (suppurative)
- Granulomatous (de Quervain's / subacute)
- Autoimmune - Hashimoto's (lymphocytic)
- Riedel's (fibrous / woody thyroiditis)
- Chronic bacterial (TB, syphilis)
(e) Other rare - Amyloid goitre, etc.
3. HISTORY TAKING
Presenting Complaint
- Duration of swelling (long history = benign; rapidly growing = malignant or anaplastic)
- Mode of onset: sudden increase in size suggests haemorrhage into a nodule
- Pain: usually absent; pain suggests thyroiditis, acute suppurative, or haemorrhage
- Rate of growth
Symptoms of Pressure (Compressive symptoms)
- Dysphagia - esophageal compression
- Dyspnoea / stridor - tracheal compression
- Hoarseness of voice - RLN involvement (DANGER sign - suggests malignancy)
- Venous engorgement - SVC / neck vein compression
Symptoms of Thyroid Dysfunction
Hyperthyroidism: Palpitations, weight loss despite good appetite, heat intolerance, excessive sweating, tremor, diarrhea, irritability, oligomenorrhea
Hypothyroidism: Weight gain, cold intolerance, constipation, lethargy, dry skin, hair loss, menorrhagia, bradycardia
Relevant History
- Endemic area? (Iodine deficiency)
- Goitrogenic diet - cabbage, cauliflower, brassica family, soya
- Antithyroid drugs / lithium / amiodarone
- Radiation exposure (neck irradiation in childhood - risk of papillary Ca)
- Family history - MEN 2A/2B (medullary thyroid Ca), familial papillary Ca
- Age and sex - female:male = 6:1 for goitre; males have higher risk of malignancy in a thyroid nodule
- Pregnancy / puberty - physiological goitre
4. EXAMINATION - SYSTEMATIC APPROACH
Expose Patient Properly
Neck exposed down to the nipple level; collar removed; patient seated with neck slightly extended.
General Examination
Look for signs of thyroid dysfunction:
| Feature | Hyperthyroid | Hypothyroid |
|---|---|---|
| Built | Thin | Obese/puffy |
| Skin | Warm, moist, velvety | Dry, coarse, cold |
| Hair | Fine, thinning | Coarse, thin, brittle |
| Pulse | Tachycardia, AF | Bradycardia |
| Eyes | Exophthalmos, lid lag, lid retraction | Periorbital puffiness |
| Hands | Tremor, palmar erythema | Dry, cold |
| Reflexes | Brisk | Slow-relaxing |
Specific eye signs (Graves' Disease):
- Exophthalmos (proptosis) - due to retroorbital infiltration
- Lid lag (von Graefe's sign) - upper lid lags behind descending eyeball
- Lid retraction (Dalrymple's sign) - sclera visible above iris
- Infrequent blinking (Stellwag's sign)
- Convergence weakness (Moebius sign)
- Joffroy's sign - absent forehead wrinkling when looking up
Local Examination of the Thyroid
INSPECTION (stand in front, then side)
Note:
- Site - midline vs lateral
- Size - rough estimate
- Shape - diffuse vs nodular
- Number of swellings - solitary vs multiple nodules
- Surface - smooth vs nodular
- Skin - normal / red (inflammation) / dilated veins / fixation
- Symmetry - which lobe is more enlarged
- Visible pulsation - thyrotoxic goitre may pulsate
- Move on swallowing - ask patient to swallow water; watch the swelling
PALPATION (stand behind the patient)
Ask patient to slightly flex the neck (relaxes sternomastoid).
Note:
- Temperature - warm in thyroiditis, normal in simple goitre
- Tenderness - present in thyroiditis, haemorrhage into nodule
- Size and extent - measure lobes; feel for substernal extension (lower border not felt = retrosternal)
- Surface - smooth vs nodular
- Consistency:
- Soft/elastic = colloid goitre, simple goitre
- Firm = adenoma, multinodular
- Hard/stony = malignancy (papillary, anaplastic), calcification, Riedel's
- Rubbery/firm = Hashimoto's (like cartilage), lymphoma
- Cystic = colloid cyst, haemorrhage, thyroglossal cyst
- Mobility - freely mobile vs fixed (fixation = malignancy)
- Confirmation of movement on swallowing
- Carotid pulsation - "Berry's sign": in malignant goitre, the carotid pulsation is absent on the affected side because the malignant thyroid mass envelops the carotid artery
- Cervical lymph nodes - palpate all groups; enlarged nodes = malignancy / Hashimoto's
PERCUSSION
- Percuss over the manubrium sterni - dull note indicates retrosternal extension
AUSCULTATION
- Bruit over the thyroid = hypervascular gland (Graves' disease, thyrotoxicosis)
- Must differentiate from a carotid bruit (heard in the neck, not directly over the gland)
PEMBERTON'S SIGN
Ask patient to raise both arms above the head. Positive = facial congestion, cyanosis, elevation of JVP, respiratory distress. Indicates functional obstruction of the thoracic inlet - suggests retrosternal goitre.
KOCHER'S TEST (Tracheal Compression Test)
Gently compress the thyroid laterally with fingers. Positive = stridor produced, indicating tracheal compression (narrowed trachea).
5. FEATURES SUGGESTING MALIGNANCY (Viva Favourite!)
| Feature | Significance |
|---|---|
| Stony hard consistency | Papillary Ca, anaplastic, calcification |
| Rapid growth | Anaplastic carcinoma |
| Hoarseness | RLN involvement |
| Fixation to surrounding structures | Invasion by malignancy |
| Dysphagia (late) | Esophageal invasion |
| Cervical lymphadenopathy | Nodal metastases (especially papillary Ca - bilateral nodes) |
| Berry's sign | Carotid enveloped by malignant mass |
| Male patient with solitary nodule | Higher malignancy risk |
| Children with nodule | Higher malignancy risk (~50%) |
| History of neck irradiation | Papillary Ca |
| Solitary nodule (vs multinodular) | Relatively higher risk of malignancy |
6. INVESTIGATIONS
Biochemical
- Serum T3, T4, TSH - essential to determine functional status
- TSH low + T3/T4 high = hyperthyroid
- TSH high + T3/T4 low = hypothyroid
- TSH suppressed with normal T3/T4 = subclinical hyperthyroidism
- Thyroid antibodies:
- Anti-TPO antibody - Hashimoto's (>95%)
- Anti-TSH receptor (TRAb / TSIG) - Graves' disease
- Anti-thyroglobulin antibody
- Serum calcitonin - if medullary thyroid carcinoma suspected (MEN 2)
- Serum thyroglobulin - tumour marker for differentiated thyroid cancer (post-thyroidectomy surveillance)
- Serum calcium - pre-operatively (parathyroid function)
Imaging
| Investigation | When/Why |
|---|---|
| Ultrasound neck | First-line for all thyroid swellings; size, cystic vs solid, nodule characteristics (TIRADS) |
| FNAC (Fine Needle Aspiration Cytology) | Gold standard investigation for a thyroid nodule; Bethesda system reporting |
| Radioisotope scan (Tc-99m or I-123) | Hot/warm/cold nodule characterization; ectopic thyroid; post-thyroidectomy remnant |
| CT neck + chest | Retrosternal extension; tracheal compression; malignancy staging |
| MRI | Same as CT without radiation; good for soft tissue detail |
| X-ray chest | Tracheal deviation, mediastinal widening, retrosternal goitre |
| X-ray neck | Tracheal deviation; soft tissue calcification (papillary Ca - psammoma bodies) |
| Laryngoscopy | Pre-op assessment of vocal cord mobility; if hoarseness present |
FNAC - Bethesda System
| Category | Risk of Malignancy | Management |
|---|---|---|
| I - Non-diagnostic | - | Repeat FNAC |
| II - Benign | <3% | Observe |
| III - AUS/FLUS | ~10-30% | Repeat / molecular testing |
| IV - Follicular neoplasm | 25-40% | Hemithyroidectomy |
| V - Suspicious for malignancy | 60-75% | Near-total/total thyroidectomy |
| VI - Malignant | >97% | Surgery |
Viva trap: FNAC cannot distinguish follicular adenoma from follicular carcinoma - this requires histology (capsular and vascular invasion). Hence Category IV requires diagnostic hemithyroidectomy.
Radioisotope Scan
- Hot nodule = increased uptake = functioning = almost never malignant (Toxic adenoma)
- Cold nodule = decreased uptake = non-functioning = 10-15% chance of malignancy
- Warm nodule = same uptake as rest of gland
7. DIFFERENTIAL DIAGNOSIS OF A MIDLINE NECK SWELLING
| Condition | Key Features |
|---|---|
| Thyroid swelling | Moves on swallowing; does NOT move on tongue protrusion |
| Thyroglossal cyst | Midline; moves on swallowing AND tongue protrusion; usually subhyoid |
| Subhyoid bursitis | Midline; moves on swallowing; rare |
| Lipoma | Does not move on swallowing; soft; lobulated |
| Dermoid cyst | Midline; tense; does not move on swallowing |
| Lymph node | Lateral usually; does not move on swallowing unless fixed to trachea |
8. MANAGEMENT OVERVIEW
Indications for Surgery in Goitre
- Pressure symptoms - dyspnoea, dysphagia, stridor
- Cosmetic disfigurement
- Suspected or confirmed malignancy
- Retrosternal extension
- Toxic goitre failing medical management or not suitable for RAI
- Failure to respond to medical treatment
Types of Surgery
| Procedure | Indication |
|---|---|
| Hemithyroidectomy (lobectomy + isthmusectomy) | Solitary nodule (diagnostic or therapeutic), Bethesda IV, unilateral disease |
| Near-total thyroidectomy | Most thyroid cancers, bilateral disease |
| Total thyroidectomy | Differentiated thyroid cancer >1 cm, medullary thyroid Ca, Graves' disease (surgical option) |
| Subtotal thyroidectomy | Graves' disease (historical), bilateral toxic MNG |
| Hartley-Dunhill operation | One lobe + partial contralateral = for bilateral MNG |
Medical Management
- Antithyroid drugs: Carbimazole, propylthiouracil (PTU)
- Beta-blockers: Propranolol - control symptoms (palpitations, tremor) rapidly
- Iodine (Lugol's): Pre-op in Graves' to reduce vascularity
- Radioactive Iodine (I-131): Graves' disease, toxic MNG (not in pregnancy/children)
- Thyroxine: Hypothyroidism post-thyroidectomy; also used to suppress TSH in differentiated Ca
- Iodine supplementation: Endemic goitre prevention and treatment
9. COMPLICATIONS OF THYROIDECTOMY (Classic Viva Topic)
Immediate (0-24 hrs)
| Complication | Mechanism | Feature |
|---|---|---|
| Reactionary haemorrhage | Slipped ligature | Neck swelling, stridor, cyanosis |
| Respiratory obstruction | Haemorrhage compressing trachea | Emergency - open wound at bedside |
| Thyroid storm | Excess hormone release | Hyperpyrexia, tachycardia, agitation |
| RLN injury (unilateral) | Nerve cut/stretched | Hoarseness |
| RLN injury (bilateral) | Both nerves cut | Aphonia, stridor - re-intubation needed |
Early (24 hrs - 1 week)
| Complication | Mechanism | Feature |
|---|---|---|
| Hypoparathyroidism | Parathyroids removed/devascularized | Hypocalcaemia → tetany; Chvostek's, Trousseau's signs |
| Wound infection | ||
| Tracheomalacia | Chronic pressure on tracheal rings | Post-extubation stridor - "tracheal kiss" |
Late
| Complication | |
|---|---|
| Hypothyroidism | After total/near-total thyroidectomy → lifelong thyroxine |
| Recurrence of goitre / toxicity | After subtotal thyroidectomy |
| Keloid scar | |
| Hypoparathyroidism (permanent) | 1-3% after total thyroidectomy |
| Voice change (external laryngeal nerve) | Loss of high-pitched notes, voice fatigue |
Viva trap - "Bed-side emergency kit": Every patient post-thyroidectomy must have a stitch-cutter or clip remover at the bedside to open the wound in emergency to evacuate haematoma.
10. HIGH-YIELD VIVA QUESTIONS & ANSWERS
Q: Why does thyroid swelling move on swallowing?
A: The thyroid is enclosed within the pretracheal fascia, which is attached to the trachea and larynx. On swallowing, these structures elevate, carrying the thyroid with them.
Q: What is the difference between primary, secondary, and tertiary thyrotoxicosis?
- Primary = Graves' disease (diffuse toxic goitre) - de novo autoimmune
- Secondary = Toxic multinodular goitre - pre-existing MNG becomes toxic
- Tertiary = Solitary toxic adenoma (Plummer's disease)
Q: FNAC cannot differentiate follicular adenoma from carcinoma. Why?
A: Because the distinction requires histological evidence of capsular invasion or vascular invasion, which cannot be assessed on fine needle aspirate cytology.
Q: What is a "cold nodule" and what is its significance?
A: A nodule with decreased radionuclide uptake on scintigraphy. Non-functioning. About 10-15% of cold nodules are malignant - hence all cold nodules require FNAC.
Q: What is Berry's sign?
A: Absence of carotid pulsation on the side of the thyroid swelling, indicating that the malignant thyroid mass has encircled/enveloped the carotid artery. Strong indicator of malignancy and inoperability.
Q: What is Pemberton's sign?
A: Raising both arms above the head causes facial congestion, cyanosis, elevation of JVP and respiratory distress - indicates a retrosternal goitre causing functional obstruction of the thoracic inlet.
Q: What is Kocher's test?
A: Lateral compression of the goitre produces stridor - indicates significant tracheal compression.
Q: The most common thyroid cancer is...?
A: Papillary carcinoma (~80%). Spreads via lymphatics. Good prognosis. Associated with Psammoma bodies (calcification), radiation exposure, RET/PTC mutations.
Q: Which thyroid cancer has the WORST prognosis?
A: Anaplastic carcinoma - median survival ~3-6 months. Usually occurs in elderly. Very rapidly growing, rock-hard mass.
Q: Which thyroid cancer is a marker of MEN syndrome?
A: Medullary thyroid carcinoma - associated with MEN 2A (with phaeochromocytoma + hyperparathyroidism) and MEN 2B (with phaeochromocytoma + mucosal neuromas + marfanoid habitus). RET proto-oncogene mutation.
Q: Pre-operative preparation for Graves' disease thyroidectomy?
A: (1) Render euthyroid with antithyroid drugs (carbimazole) over 6-8 weeks. (2) Give Lugol's iodine (potassium iodide) for 10-14 days pre-op to reduce gland vascularity and firmness. (3) Propranolol to control sympathetic symptoms.
Q: What is the Hartley-Dunhill operation?
A: Total removal of one lobe + isthmus + subtotal removal of the other lobe. Used for bilateral multinodular goitre - balances the risk of recurrence vs hypothyroidism.
Sources: S Das - A Manual on Clinical Surgery 13th ed. | Bailey & Love's Short Practice of Surgery 28th ed. | Sabiston Textbook of Surgery | Schwartz's Principles of Surgery 11th ed. | Harrison's Principles of Internal Medicine 22E
Brest topic in surgery cover the history taking , examination point,and other viva qsn
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Breast - Complete Surgical Viva Guide
1. HISTORY TAKING
Patient Details
- Age - single most important demographic factor:
- <35 yrs: Fibroadenoma most likely
- 20-40 yrs: Fibroadenosis (mammary dysplasia)
-
40 yrs: Carcinoma must always be excluded
- Young lactating woman: Mastitis / breast abscess
- Sex - rare but carcinoma in males is possible
- Residence - carcinoma + fibroadenosis more common in western world; rare in Japan
- Parity / Social status - nulliparous women have higher risk of carcinoma and fibroadenosis; breastfeeding is protective
Chief Complaint
1. Lump (most common presenting complaint)
- Mode of onset, duration
- Rate of growth: slow + long history = benign; fast + short history = likely malignant
- Sudden enlargement: haemorrhage into a cyst or nodule
- Note: average time between patient discovering a breast lump and reporting to a surgeon is ~6 weeks in carcinoma
2. Pain (mastalgia)
"Carcinoma of the breast is a painless condition." - S Das
| Pain type | Diagnosis |
|---|---|
| Throbbing, severe | Acute mastitis / abscess (pus formation) |
| Cyclical, worse before periods | Fibroadenosis (most common benign cause) |
| Non-cyclical, localized | Periductal mastitis, fat necrosis |
| Back / hip / shoulder pain (late) | Bony metastases from carcinoma |
| Painless lump accidentally felt | Must rule out carcinoma |
3. Nipple Discharge
| Discharge colour | Diagnosis |
|---|---|
| Bright red / blood | Duct papilloma (most common), duct carcinoma |
| Serous / clear | Duct papilloma, early carcinoma |
| Green / brown | Fibroadenosis (duct ectasia) |
| White (milk) | Galactorrhoea (prolactinoma, drugs) |
| Purulent | Abscess, infected duct ectasia |
4. Nipple changes
- Retraction / inversion - recent onset = malignancy; lifelong = normal variant
- Eczema / scaling of nipple = Paget's disease of nipple (must exclude underlying ductal carcinoma)
- Ulceration
5. Skin changes - redness, dimpling, peau d'orange, ulceration, satellite nodules
6. Axillary swelling - may indicate nodal metastases
Past History
- Previous breast lumps, biopsies, operations
- History of chest wall irradiation (risk factor for breast cancer)
- Hormone use - OCP, HRT (risk factors)
- Previous carcinoma of the opposite breast or endometrium
Menstrual & Obstetric History
- Menarche age (early menarche = risk factor)
- Menopause age (late menopause = risk factor)
- Pregnancies: nulliparity or first child after 30 = risk factor
- Breastfeeding: protective
- Last menstrual period
Family History
- First-degree relative (mother, sister) with breast cancer = 2-3x increased risk
- BRCA1 / BRCA2 mutations (ask for family history of ovarian cancer too)
- Bilateral or early-onset (<50 yrs) breast cancer in family = high risk
Drug History
- OCP, HRT (slight increased risk)
- Phenothiazines, metoclopramide, domperidone → galactorrhoea
- Tamoxifen (if currently being treated)
2. EXAMINATION - SYSTEMATIC APPROACH
General Examination
- Build, weight loss (late cancer)
- Pallor, jaundice (liver metastases)
- Lymphoedema of the arm (post-surgery or nodal blockage)
- Lumbar spine / hip tenderness (bone metastases)
- Hepatomegaly (liver metastases)
- Signs of pleural effusion (lung metastases)
LOCAL EXAMINATION
Setup
- Patient seated facing examiner, fully exposed to the nipple level
- Adequate privacy; chaperone
- Examine normal breast first, then compare with affected side
INSPECTION (4 positions)
Position 1: Arms by the side (at rest)
Note:
- Symmetry of both breasts - any size difference
- Contour and shape - any flattening, bulge, distortion
- Skin changes:
- Redness / erythema = mastitis, inflammatory carcinoma
- Peau d'orange = skin oedema with pitting, deepening of sweat gland openings - classic sign of carcinoma (lymphatic blockage by cancer cells)
- Dimpling / puckering = invasion of Cooper's ligaments by carcinoma
- Dilated superficial veins = cystosarcoma phylloides, rapidly growing sarcoma, acute duct obstruction
- Ulceration / fungation = advanced carcinoma
- Skin nodules = satellite / metastatic skin deposits
- Nipple position, level, symmetry
- Retraction (recent = malignant; central mass pulling nipple)
- Deviation / asymmetry
- Ulceration / eczema = Paget's disease
- Axillae - visible swelling, skin puckering

Peau d'orange - oedema of the skin of the breast with deepening of the sweat gland mouths, due to blockage of subcuticular lymphatics by cancer cells. - S Das Clinical Surgery
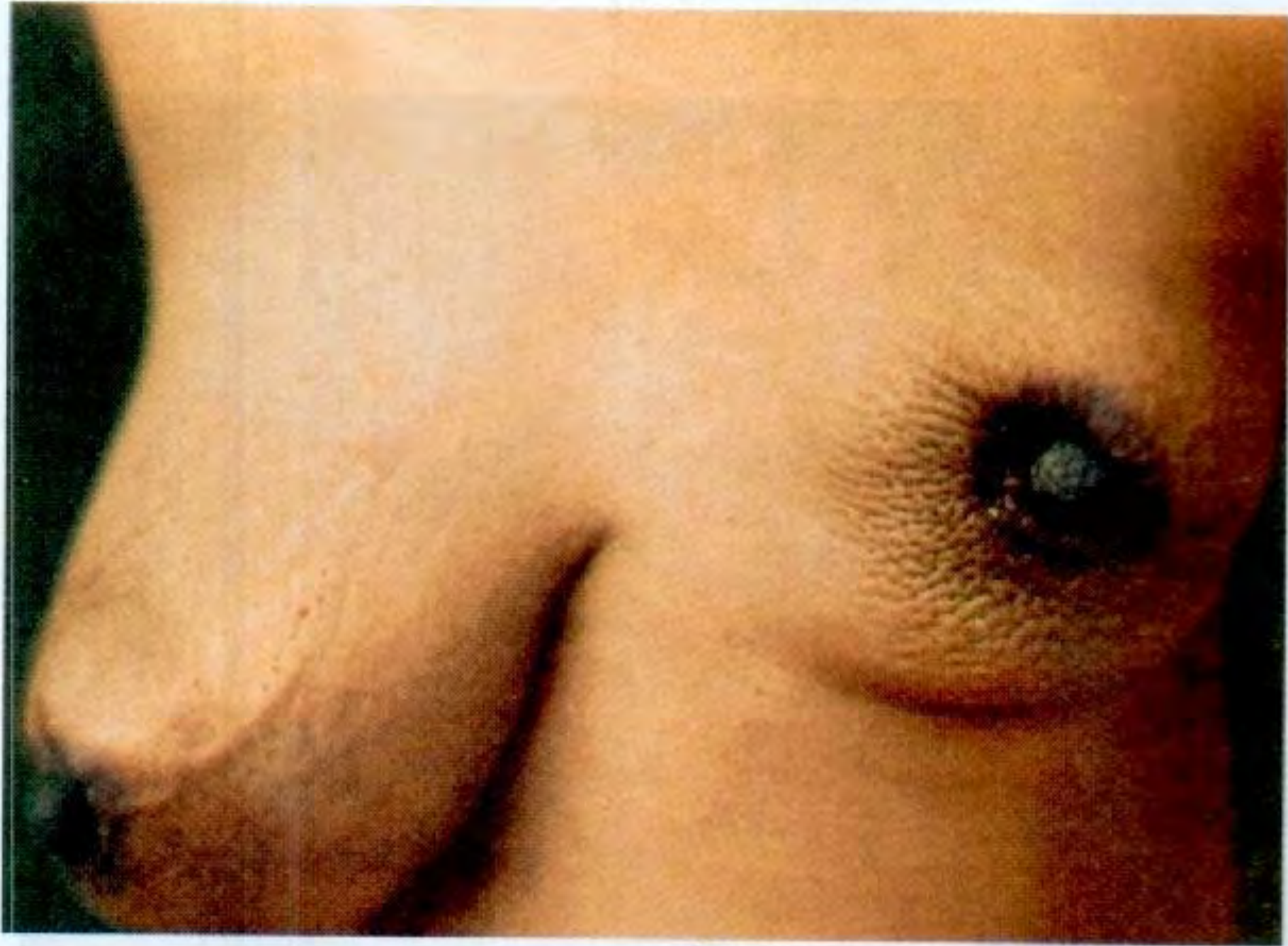
Nipple retraction caused by deep carcinoma pulling along the lactiferous ducts via fibrosis - S Das
Position 2: Arms raised above the head
- Reveals the lower surfaces of both breasts
- Brings out lumps, puckering and distortion not visible at rest
- Inspect the submammary fold (lift breast if needed)
- Inspect axillae for swelling and ulceration
Position 3: Hands pressed on hips (pectoral contraction)
- Tenses the pectoralis major
- Accentuates dimpling / tethering if present (Cooper's ligament invasion)
- Any change in contour with muscle contraction
Position 4: Leaning forward
- Pendulous breasts fall forward - reveals asymmetry and skin changes on undersurface
PALPATION
Patient position: Start in sitting, then semi-recumbent (45°), then lying supine with a small pillow under the scapula of the side being examined (prevents breast falling laterally).
Technique:
- Use the palmar surface of the fingers with the hand flat (NOT the palm of hand, NOT fingertips)
- Palpate between pulps of fingers and thumb to examine a lump
- Always palpate the normal breast first to know the baseline texture
Quadrant Examination
Systematically palpate all four quadrants:
- Upper outer (UOQ) - most common site of carcinoma (50%)
- Upper inner
- Lower outer
- Lower inner
- Retroareolar region (just behind the nipple - easy to miss!)
- Axillary tail of Spence
On Finding a Lump - Assess All These Features:
1. Site / Position
- Quadrant + distance from nipple
- UOQ is most common; retroareolar is often missed
2. Size and Shape
- Measure in cm
- Globular = fibroadenoma
- Irregular = carcinoma
3. Number
- Solitary: fibroadenoma, cyst, carcinoma
- Multiple bilateral: fibroadenosis
4. Surface
- Smooth = fibroadenoma, cyst
- Irregular / nodular = carcinoma, fibroadenosis
5. Edge / Margin
- Well-defined = fibroadenoma, cyst
- Ill-defined / spiculated = carcinoma
6. Consistency
| Consistency | Diagnosis |
|---|---|
| Soft, cystic | Breast cyst, abscess |
| Firm, India-rubber / diffuse | Fibroadenosis |
| Firm, well-encapsulated | Fibroadenoma |
| Stony hard, irregular | Carcinoma |
| Varies (soft to hard) | Sarcoma / cystosarcoma phylloides |
7. Fluctuation - test for cystic swellings (cyst, abscess)
8. Transillumination - in dark room; cyst = translucent; solid tumour = opaque; fat = translucent
9. Tenderness - mastitis, abscess; absent in carcinoma (painless)
10. Fixity to Skin - Three levels:
(i) Tethering to skin: Invasion of Cooper's ligaments (fibrous septae from gland to skin). The lump can still be moved slightly but at the extremes of movement, skin dimples.
- Test: move lump side to side - skin dimples at extremes = tethered
(ii) Fixed to skin: Direct infiltration of skin by tumour. Lump cannot be moved independent of skin. Overlying skin cannot be pinched up.
(iii) Note: Any tumour deep to the nipple will be fixed to the nipple (benign or malignant) because the main lactiferous ducts pass through it.
11. Fixity to Breast Tissue
- Fibroadenoma: freely mobile within breast substance = "Breast Mouse" / "Floating Tumour"
- Carcinoma: fixed to breast tissue; fibrous strands radiating from mass
12. Fixity to Pectoralis Major
- Ask patient to press her hand on her hip lightly (muscle relaxed) - test lump mobility
- Now ask her to press hip as hard as she can (muscle taut) - retest mobility
- Reduced mobility in the line of muscle fibres = fixed to pectoralis major or pectoral fascia

Testing lump fixity to pectoralis major - patient presses hip to tighten muscle, then lump mobility is reassessed in direction of muscle fibres. - S Das
13. Fixity to Serratus Anterior
- Lower outer quadrant lumps may fix to serratus anterior
- Test: ask patient to push against a wall with outstretched hand of affected side - fixed lump barely moves
14. Fixity to Chest Wall
- Lump restricted in ALL directions irrespective of any muscle contraction = fixed to chest wall (T4 carcinoma)
15. Nipple Palpation
- Feel tissue just behind the nipple
- Press the lump behind the nipple - note if this expresses discharge
- Colour of discharge (see above)
- From single duct (papilloma) or multiple ducts (fibrocystic)
16. Axillary Examination
Patient's arm supported by examiner's ipsilateral hand (relaxing pectoralis)
Palpate all groups:
- Anterior (pectoral) nodes - most commonly first involved in breast cancer
- Central nodes
- Posterior (subscapular) nodes
- Lateral (brachial) nodes
- Apical nodes (infraclavicular)
Note: Size, number, consistency, mobility, tenderness of any palpable nodes
17. Supraclavicular Nodes
- Feel in the angle between the clavicle and sternomastoid from behind
- Enlarged = advanced (N3) disease
18. Opposite Breast and Axilla - must always be examined
3. DIFFERENTIAL DIAGNOSIS OF A BREAST LUMP
| Condition | Age | Consistency | Mobility | Tender | Skin/Nipple | Other |
|---|---|---|---|---|---|---|
| Fibroadenoma | 15-35 | Firm, smooth | Highly mobile ("breast mouse") | No | Normal | Well-defined, no nodes |
| Breast cyst | 30-55 | Cystic/fluctuant | Mobile | No | Normal | Transilluminates; may refill |
| Fibroadenosis | Any (20-50) | Firm, diffuse, nodular | Diffuse bilateral | Yes (cyclical) | Normal | Multiple lumps |
| Carcinoma | >40 | Stony hard | Fixed to breast tissue | No | Peau d'orange, dimpling | Hard nodes, nipple retraction |
| Abscess | Lactating | Fluctuant | Fixed (inflamed) | Very tender | Red, warm | Fever, raised WBC |
| Fat necrosis | Any (post-trauma) | Hard, irregular | May be fixed | ± | Skin tethering possible | History of trauma |
| Cystosarcoma phylloides | >40 | Varies; huge | Mobile (initially) | No | Dilated veins; not fixed | Rapidly growing, giant tumour |
| Duct papilloma | >30 | Cystic near areola | Mobile | No | Bloody nipple discharge | Retroareolar |
| Paget's disease | >50 | Underlying mass | - | No | Eczema of nipple | Represents underlying DCIS/Ca |
| Gynaecomastia (male) | Any | Firm disc | Central | Tender | Normal | Bilateral rubbery disc |
4. TRIPLE ASSESSMENT (The Standard for any Breast Lump)
The gold standard is Triple Assessment - all three must be done:
| Component | What |
|---|---|
| 1. Clinical examination | History + full breast exam |
| 2. Imaging | Mammogram (<35 yrs: USG; >35 yrs: Mammogram ± USG) |
| 3. Tissue sampling | FNAC (cytology) or Core needle biopsy (histology) |
If all 3 are benign = safe to observe. If ANY is suspicious = proceed to excision/surgery.
5. INVESTIGATIONS
Imaging
Mammography
- Investigation of choice for women >35-40 years
- Two views: craniocaudal (CC) and mediolateral oblique (MLO)
- Malignant features: spiculated mass, pleomorphic calcifications, skin thickening, nipple retraction
- BIRADS classification: BIRADS 1 = normal; BIRADS 5 = highly suggestive malignancy
- Screening mammogram: every 2 years for women 50-74 yrs (national programs)
Ultrasound (USG)
- Preferred for women <35 years (dense breast tissue makes mammography less useful)
- Distinguishes solid vs cystic lesions
- Guides FNAC/core biopsy
- Benign features: smooth margins, posterior acoustic enhancement (cyst)
- Malignant features: irregular hypoechoic mass, spiculated margins, posterior shadowing
MRI Breast
- Not routine; used for:
- BRCA mutation carriers (high-risk screening)
- Assessing extent of lobular carcinoma
- Occult primary breast cancer with axillary nodes
- Pre-operative planning for BCS (breast conserving surgery)
- Implants assessment
Tissue Diagnosis
FNAC (Fine Needle Aspiration Cytology)
- 22-25G needle, syringe, no anaesthesia
- Gives cytological diagnosis only
- Reports as: C1 (inadequate) / C2 (benign) / C3 (atypia) / C4 (suspicious) / C5 (malignant)
- Advantage: quick, cheap, outpatient
- Limitation: cannot distinguish invasive from in-situ cancer; cannot give hormone receptor status
Core Needle Biopsy (Tru-cut)
- 14-16G needle; gives a core of tissue = histological diagnosis
- Can determine: invasive vs in-situ; grade; ER/PR/HER2 status
- Preferred over FNAC when preoperative planning is needed
Excision Biopsy
- When FNAC/core is inconclusive (Bethesda III equivalent / C3)
- Provides definitive diagnosis
Blood Tests
- CBC - anaemia in advanced disease
- LFT, ALP - liver / bone metastases
- Serum calcium - hypercalcaemia in bone metastases
- Tumour markers: CA 15-3, CEA - used for monitoring treatment response, not diagnosis
- Hormone receptor status (ER, PR, HER2) on biopsy - determines treatment
Staging Investigations (if cancer confirmed)
- Chest X-ray - lung metastases
- CT chest / abdomen / pelvis - staging
- Bone scan - bone metastases (indicated if bone pain or raised ALP)
- PET-CT - accurate staging in high-risk disease
6. STAGING OF BREAST CANCER
TNM Classification
| T | Description |
|---|---|
| T1 | ≤2 cm; no fixation; no nipple retraction |
| T2 | 2-5 cm; skin may be tethered; no pectoral fixation |
| T3 | >5 cm; skin fixed or ulcerated; pectoral fixation |
| T4 | Chest wall fixation; peau d'orange over large area; inflammatory carcinoma |
| N | Description |
|---|---|
| N0 | No palpable ipsilateral nodes |
| N1 | Mobile ipsilateral axillary nodes |
| N2 | Fixed axillary nodes |
| N3 | Supraclavicular / infraclavicular nodes; arm oedema |
| M | Description |
|---|---|
| M0 | No distant metastasis |
| M1 | Distant metastasis present |
Clinical Stages (S Das)
- Stage I: Growth limited to breast; ± small skin adherence
- Stage II: + Mobile axillary nodes; ± slight pectoral tethering
- Stage III: Fixed to pectoral muscle; skin involvement > tumour size
- Stage IV: Fixed to chest wall; fixed axillary nodes; supraclavicular nodes; distant metastases
7. TYPES OF BREAST CARCINOMA
| Type | Features |
|---|---|
| Scirrhous carcinoma | Most common; very hard, fibrotic; slow growing; infiltrative |
| Atrophic scirrhous | Least malignant; very slow growing; may mimic benign |
| Encephaloid (Medullary) | Soft brain-like; rapidly growing; less fibrosis; better prognosis |
| Comedocarcinoma | Intraductal; DCIS type; "toothpaste-like" plugs from ducts |
| Colloid (Mucinous) | Gelatinous; better prognosis; older women |
| Mastitis carcinomatosa (Inflammatory Ca) | Most malignant; entire breast red, hot, oedematous; no palpable lump; poor prognosis |
| Paget's disease of nipple | Eczema-like change of nipple; underlying DCIS or invasive Ca; always biopsy |
| Lobular carcinoma | Diffuse, bilateral; harder to detect on mammogram |
Metastatic spread:
- Lymphatic: Axillary nodes (most common) → supraclavicular → internal mammary nodes
- Blood: Bones (most common - especially spine, pelvis, femur), lung, liver, brain, ovary (transcoelomic)
8. MANAGEMENT
Benign Conditions
| Condition | Management |
|---|---|
| Fibroadenoma | Small (<3 cm): observe; large / growing / symptomatic: excision |
| Breast cyst | Aspiration (diagnostic + therapeutic); if bloody fluid / residual lump → biopsy |
| Fibroadenosis | Reassurance; evening primrose oil; danazol for severe mastalgia |
| Mastitis / Abscess | Antibiotics (flucloxacillin); if abscess = incision and drainage (I&D) or needle aspiration |
| Duct papilloma | Microdochectomy (excision of affected duct); considered premalignant |
| Cystosarcoma phylloides | Wide local excision or simple mastectomy (tends to recur); rarely malignant |
| Gynaecomastia | Treat cause; if persists / painful: subcutaneous mastectomy |
Malignant Conditions - Breast Cancer Surgery
Breast Surgery Options
| Procedure | Indication |
|---|---|
| Wide Local Excision (WLE) / Lumpectomy | Early cancer; followed by radiotherapy = Breast Conserving Surgery (BCS) |
| Quadrantectomy | Removal of involved quadrant |
| Simple (Total) Mastectomy | Carcinoma in-situ; prophylactic (BRCA1/2); when BCS not possible |
| Modified Radical Mastectomy (MRM) | Most common surgery for breast cancer today; removes breast + axillary nodes; preserves pectoralis major |
| Radical Mastectomy (Halsted) | Historical; removes breast + pectoralis major + minor + axillary nodes; rarely done now |
| Extended Radical Mastectomy | Also removes internal mammary nodes; obsolete |
Axillary Management
| Procedure | Indication |
|---|---|
| Sentinel Lymph Node Biopsy (SLNB) | Clinically node-negative axilla; if SLNB negative = no further axillary surgery |
| Axillary Lymph Node Dissection (ALND) | SLNB positive; clinically / radiologically positive nodes |
Adjuvant Therapy
| Treatment | Indication |
|---|---|
| Radiotherapy | Post-BCS (mandatory); post-mastectomy in high-risk; chest wall |
| Chemotherapy | Triple-negative, HER2+, high-grade, node-positive disease |
| Hormonal therapy (Tamoxifen / Aromatase inhibitors) | ER/PR positive (5-10 years) |
| HER2 targeted (Trastuzumab/Herceptin) | HER2-positive tumours |
9. HIGH-YIELD VIVA QUESTIONS & ANSWERS
Q: What is the most common site of carcinoma in the breast?
A: Upper outer quadrant (UOQ) - approximately 50% of all breast carcinomas. It has the greatest volume of breast tissue and the axillary tail.
Q: What is "peau d'orange" and what causes it?
A: Peau d'orange (French: "skin of an orange") is oedema of the breast skin with deepening of the sweat gland and hair follicle openings, giving an orange-peel appearance. It is caused by obstruction of the subcuticular lymphatics by cancer cells, leading to skin oedema, while the tethered skin over follicles cannot expand - creating the pitted appearance.
Q: What is Cooper's ligament and what happens when it is invaded?
A: Cooper's ligaments (suspensory ligaments of the breast) are fibrous septae passing from the glandular breast tissue to the overlying skin. When invaded by carcinoma, they become shorter and inelastic, pulling the skin inwards, causing skin dimpling, puckering or retraction.
Q: What is a "breast mouse"?
A: A fibroadenoma - it is highly mobile within the breast substance and freely movable under the examining fingers, hence the term. It is NOT fixed to the skin or deeper structures.
Q: What is Paget's disease of the nipple?
A: A form of breast cancer presenting as eczema-like changes (scaling, weeping, crusting) of the nipple and areola. It represents extension of an underlying ductal carcinoma in-situ (DCIS) or invasive carcinoma through the lactiferous ducts to the nipple epidermis. Always biopsy nipple eczema in a woman over 40. Treatment: total mastectomy or BCS + nipple excision + radiotherapy.
Q: "Breast cancer is painless" - always true?
A: Painless at onset - all neoplasms of the breast (benign or malignant) are painless to start. However, late-stage carcinoma can cause pain from bone metastases (back, hip, shoulder pain). Inflammatory carcinoma is a painful exception. Pain should never be used to exclude carcinoma.
Q: What is the most common type of breast cancer?
A: Invasive ductal carcinoma (IDC) / scirrhous carcinoma - accounts for ~75-80% of all breast cancers. Presents as a hard, stony, irregular mass with fibrous stroma.
Q: What is the difference between tethering and fixation to skin?
- Tethering: Malignancy has spread to Cooper's ligaments; lump can still move independently through a small range, but skin dimples at the extremes of movement. (T2 feature)
- Fixed: Direct infiltration of skin by tumour; lump cannot be moved independently at all; overlying skin cannot be pinched up. (T4 feature)
Q: What is triple assessment?
A: The gold standard approach for evaluating any breast lump:
- Clinical examination
- Imaging (mammogram ± ultrasound)
- Tissue sampling (FNAC or core biopsy) All three results must be concordant. If any one is suspicious → proceed to surgery.
Q: How do you test for fixity to pectoralis major?
A: Ask the patient to press her hand on her hip (muscle relaxed) - assess lump mobility. Then ask her to press as hard as possible (muscle taut) - retest mobility in the line of the muscle fibres. Restricted mobility with the muscle contracted indicates fixity to pectoralis major or pectoral fascia.
Q: What is Modified Radical Mastectomy (MRM)?
A: Removal of the entire breast + all axillary lymph nodes, while preserving both pectoralis major and minor. This is the standard surgical procedure for breast cancer today. It replaced Halsted's radical mastectomy (which removed both pectoral muscles) as outcomes were equivalent with less morbidity.
Q: Most common site of blood-borne metastasis from breast cancer?
A: Bones (spine, pelvis, femur) - most common. Others: lungs, liver, brain, ovary (Krukenberg - transcoelomic).
Q: Risk factors for breast cancer?
A: MNEMONIC - "FEMALE BRAS"
- Family history (first-degree relative, BRCA1/2)
- Early menarche (<12 yrs)
- Menopause late (>55 yrs)
- Age (>40 yrs)
- Late first pregnancy / nulliparity
- Exposure to radiation
- Body weight (obesity - increases oestrogen)
- Risk from HRT / OCP
- Alcohol, diet rich in saturated fat
- Socioeconomic (more in Western world)
Q: What is inflammatory carcinoma?
A: The most malignant type of breast cancer (mastitis carcinomatosa). The entire breast becomes red, hot, swollen, oedematous - resembling acute mastitis. There may be no discrete palpable mass. Due to massive lymphatic infiltration causing dermal lymphatic obstruction. Very poor prognosis. Treatment: neoadjuvant chemotherapy first, then surgery + radiotherapy. Do NOT mistake it for mastitis and delay diagnosis.
Sources: S Das - A Manual on Clinical Surgery, 13th ed. | Bailey & Love's Short Practice of Surgery, 28th ed. | Schwartz's Principles of Surgery, 11th ed. | Harrison's Principles of Internal Medicine, 22E
Create a PDF summary of breast examination techniques with diagrams
Reading File
Running Command
Writing File
Running Command
Editing File
Running Command
Editing File
Editing File
Running Command
This is a shared conversation. Sign in to Orris to start your own chat.