
IMG_3865.jpg
Answer in detail
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Here are comprehensive, detailed answers to all questions on the paper:
SECTION B - Short Answer Questions
Q1. Stree Vishishta Marma and Clinical Signs of Injury (Viddha Lakshana)
Definition of Marma
Marma are vital anatomical points where Prana (life force) resides. They are the junctions of Mamsa (muscle), Sira (vessels), Snayu (ligaments/nerves), Asthi (bone), and Sandhi (joints). Injury to a Marma can cause severe impairment or death.
Stree Vishishta Marma (Female-Specific Vital Points)
Acharya Sushruta described Marmas specific to women located in the reproductive tract. The main Stree Vishishta Marmas are:
| Marma | Location | Type |
|---|---|---|
| Garbhashaya | Uterus | Mamsa Marma |
| Bhaga | Vaginal region/vulva | Sira Marma |
| Apatyapatha | Birth canal/cervix | Marma of mixed type |
| Stanmula | Base of breast | Sira Marma |
| Stanrohita | Nipple/areola region | Sira Marma |
| Apanga | Outer canthus (related via sira) | Sira Marma |
Viddha Lakshana (Signs of Injury to Stree Vishishta Marma)
Garbhashaya Marma injury:
- Repeated pregnancy loss (Garbhasrava, Garbhapata)
- Infertility (Vandhyatva)
- Uterine hemorrhage
- Severe dysmenorrhea
- Garbhadosha - fetal abnormality
Bhaga Marma injury (vaginal/vulvar):
- Excessive bleeding per vaginum
- Dyspareunia
- Urinary dysfunction
- Loss of sensation in the region
Apatyapatha Marma injury:
- Difficulty in childbirth
- Prolonged labor (Mudhagarbha)
- Post-partum hemorrhage
- Cervical incompetence
Stanmula / Stanrohita injury:
- Lactation failure (Stanya Kshaya)
- Breast abscess, mastitis
- Stanya vitiation
General Viddha Lakshana of Marma (as per Sushruta):
- Sadya Pranahara (immediate death) - if Sadya Pranahara Marma
- Kalantara Pranahara (delayed death)
- Vishalyaghna (death on removal of the foreign body)
- Vaikalyakara (permanent disability)
- Rujkara (severe pain only)
Q2. Garbhashayantara Garbha Sthiti - Ayurvedic Concept of Fetus-in-Utero
This corresponds to the modern concept of fetal lie, attitude, presentation, presenting part, denominator, and position.
(A) Lie (Garbha Sthiti / Garbha Avastthana)
Ayurveda describes the natural position of the fetus in the uterus:
- Sutika Sthiti (Normal): Head-down, spine parallel to maternal spine - corresponds to longitudinal lie
- Tiryak Garbha: Fetus lying transverse - transverse lie
- Urdhva Garbha: Head upward - corresponds to breech
(B) Attitude (Garbha Mudra)
- Natural curled posture of the fetus (like a coiled creature)
- Sushruta describes the fetus sitting with head between knees, arms folded, spine curved
- Corresponds to the universal attitude of flexion
(C) Presentation (Garbha Mukha / Avamukha)
| Ayurvedic Term | Meaning | Modern Equivalent |
|---|---|---|
| Shiro Garbha | Head first | Cephalic presentation |
| Pada Garbha | Feet first | Footling breech |
| Nitamba Garbha | Buttocks first | Frank breech |
| Hasta Garbha | Hand first | Arm prolapse |
| Tiryak Garbha | Transverse | Shoulder presentation |
(D) Presenting Part & Denominator
- In Shiro Garbha - the presenting part is the vertex (Shira)
- Denominator in Ayurveda corresponds to the reference bony landmark - for vertex it is the Shiratala (occiput)
- For breech it is the Nitamba (sacrum)
- For face it is the Hanugra (mentum)
(E) Position
Described in terms of which side the denominator faces relative to the mother's pelvis:
- Dakshina (right) or Vama (left) position
- Corresponds to modern LOA, ROA, LOP, ROP etc.
Q3. Define Garbha and Describe Garbhadhana (Conception) According to Ayurveda
Definition of Garbha
As per Charaka Samhita (Sharira Sthana 3/3):
"Shukra-shonita-jeevatmabhih samsrushta garbha iti uchyate"
Garbha is formed by the union of:
- Shukra - paternal seed (sperm/semen)
- Shonita - maternal seed (ovum/menstrual blood)
- Jeeva/Atma - the living soul/consciousness
- Satva - mind/psyche
- Tridosha (Vata, Pitta, Kapha) - in balanced form
- Panchamahabhuta - five basic elements
The Garbha thus formed embodies all factors necessary for life - body, mind, and soul.
Garbhadhana - The Process of Conception
Prerequisites (Sambhava Samagri - factors required for conception):
- Riitu - Fertile period (Ritukala = days 4-16 of cycle)
- Kshetra - Healthy uterus (Garbhashaya shuddha)
- Ambu - Adequate nourishment/fluids (Aahar rasa)
- Beeja - Healthy seeds (Shukra + Shonita)
Ritukala (Fertile Period):
- Begins from day 4 after onset of menstruation
- Lasts 12 days (days 4-16)
- Odd nights (5th, 7th, 9th...) favor male progeny
- Even nights (4th, 6th, 8th...) favor female progeny
- Days 4-6 are inauspicious for conception
Process of Garbhadhana:
- Pumsavana Samskara precedes conception rituals
- Sexual union during Ritukala
- Shukra (sperm) travels upward through Apatyapatha (birth canal) via Sira and reaches Garbhashaya
- Shukra unites with Shonita (ovum) in the uterus
- Atma (soul) descends and enters the union due to Karma (past actions)
- Garbha is thus formed - Avyakta (invisible, undifferentiated) at first
Mahabhuta composition of Garbha (from parents):
| From Shukra (Father) | From Shonita (Mother) |
|---|---|
| Keshas (hair) | Tvak (skin) |
| Snayu (tendons) | Rakta (blood) |
| Asthi (bone) | Mamsa (muscle) |
| Majja (marrow) | Meda (fat) |
| Shukra (semen) | Hridaya (heart) |
Q4. Clinical Diagnosis of Pregnancy - Signs and Symptoms in First Trimester
Presumptive (Sambhavita) Signs - Subjective
- Amenorrhea - Absence of expected menses (most common first sign)
- Nausea and vomiting - "Morning sickness"; begins week 4-6, peaks week 8-10
- Breast changes - Fullness, tingling, tenderness; darkening of areola
- Urinary frequency - Due to pressure on bladder + increased GFR
- Fatigue and lassitude
- Food cravings/aversions (Dauhrida) - Also described in Ayurveda as Dauhrida (desire of two hearts - mother + fetus)
- Quickening - Fetal movements (usually weeks 16-20; not first trimester)
Probable (Sambhava) Signs - Objective but not definitive
- Uterine enlargement - Detectable per abdomen by 12 weeks
- Hegar's sign - Softening of the isthmus (week 6-10); bimanual; lower uterine segment soft, body firm, cervix firm - "three-part" sign
- Goodell's sign - Softening of the cervix (from 4th week)
- Chadwick's sign - Bluish-purple discoloration of the vagina and cervix due to engorgement
- Osiander's sign - Pulsations felt in the lateral vaginal fornices
- Ballottement - Internal ballottement (bimanual) at 16-20 weeks; external at 20 weeks
- Jacquemier's / Kluge's sign - Blue discoloration of vaginal walls
- Braxton-Hicks contractions - Painless irregular uterine contractions from 6th week
- Positive pregnancy test (urine/serum hCG)
Positive (Nishchita) Signs
- Fetal heart sounds - Doppler from week 10-12; stethoscope from week 20
- Fetal movements felt by examiner (not first trimester)
- Ultrasonography - Gestational sac from 4-5 weeks; fetal pole and cardiac activity from 6 weeks
Ayurvedic Signs of Pregnancy (Garbha Lakshana):
- Prasad (happiness, contentment)
- Manda pravrutti (sluggishness)
- Syava stana (nipple darkening)
- Aruchi (anorexia) or Abhilasha (cravings)
- Urdhva nabhivriddhi (elevation of umbilicus)
Q5. Precocious and Delayed Puberty - Differences, Etiological Factors, and Management
Normal Puberty (Reference)
- Girls: Begins 8-13 years; thelarche first, then pubarche, menarche
- Boys: Begins 9-14 years; testicular enlargement first
Precocious Puberty
Definition: Development of secondary sexual characteristics before age 8 in girls and 9 in boys.
Classification:
| Type | Mechanism |
|---|---|
| GnRH-dependent (Central/True) | Premature activation of HPG axis |
| GnRH-independent (Peripheral) | Autonomous sex steroid secretion |
Etiological Factors:
Central (GnRH-dependent):
- Idiopathic (most common, especially in girls)
- CNS tumors: hypothalamic hamartoma (most common organic cause), astrocytoma, ependymoma
- CNS infections, trauma, irradiation
- Hydrocephalus
- Neurofibromatosis type 1
- Tuberous sclerosis
Peripheral (GnRH-independent):
- McCune-Albright Syndrome (fibrous dysplasia + cafe-au-lait spots + precocious puberty)
- Congenital adrenal hyperplasia (CAH)
- Adrenal/gonadal tumors (estrogen or androgen-secreting)
- Exogenous sex steroid exposure
- Primary hypothyroidism (Van Wyk-Grumbach syndrome)
Clinical Features:
- Early breast development, pubic/axillary hair
- Menstruation before age 8
- Accelerated growth velocity initially, but premature epiphyseal fusion leads to short final adult height
- Advanced bone age on X-ray
Management:
- GnRH agonists (leuprolide, histrelin) - suppress HPG axis; treatment of choice for central precocious puberty
- Aromatase inhibitors (for peripheral, estrogen-dependent)
- Treat underlying cause (tumor, CAH, hypothyroidism)
- Monitor bone age, growth velocity, and pubertal staging every 6 months
- Psychological support
Delayed Puberty
Definition: Absence of breast development by age 13 in girls, or no testicular enlargement by age 14 in boys, or absence of menarche by 16 years (primary amenorrhea).
Etiological Factors:
| Category | Examples |
|---|---|
| Constitutional delay (most common in boys) | Family history; self-limiting |
| Hypogonadotropic hypogonadism | Kallmann syndrome, hypopituitarism, chronic illness, malnutrition, hypothyroidism, hyperprolactinemia, anorexia nervosa |
| Hypergonadotropic hypogonadism | Turner syndrome (45,X), Klinefelter syndrome, gonadal dysgenesis, autoimmune oophoritis, chemotherapy/irradiation |
| Anatomical | Imperforate hymen, Mayer-Rokitansky-Kuster-Hauser syndrome |
Investigations:
- FSH, LH (high = primary gonadal failure; low = hypogonadotropic)
- Karyotype (for Turner/Klinefelter)
- Bone age X-ray
- MRI brain (if CNS pathology suspected)
- Prolactin, thyroid function tests
Management:
- Constitutional delay: Reassurance; short course of low-dose sex steroids if psychosocial distress
- Hypogonadotropic hypogonadism: GnRH pulsatile therapy or gonadotropin therapy (for fertility); hormone replacement therapy (HRT) for secondary sexual development
- Hypergonadotropic: HRT (estrogen + progesterone) for feminization and bone protection
- Turner syndrome: GH therapy for height, then estrogen HRT
- Anatomic causes: Surgical correction
Q6. Clinical Indications, Diagnostic Uses, and Contraindications
I. Cusco's Speculum (Bivalve Speculum)
Description: A bivalve, self-retaining vaginal speculum made of stainless steel or disposable plastic with two flat blades joined at the distal end and a screw/ratchet locking mechanism.
Clinical Indications and Diagnostic Uses:
- Visualization of vaginal walls and cervix
- Inspection of cervix for:
- Erosion, ectropion
- Cervicitis, polyp
- Carcinoma cervix
- Collection of Pap smear (cervical cytology)
- Colposcopy - directed biopsy
- Obtaining high vaginal swab (HVS) and endocervical swab
- IUCD insertion and removal
- Cervical cauterization, cryotherapy
- Assessment of vaginal discharge, foreign body
- Assessment of cervical dilatation in labor
- Application of cervical suture (Shirodkar/McDonald)
- Culdocentesis (posterior fornix aspiration)
- Ring pessary insertion/removal
Contraindications:
- Imperforate hymen or very narrow introitus (in virgo intacta)
- Severe vaginismus (relative)
- Active vaginal/vulval infections causing extreme pain (relative)
- Atrophic vaginitis (use lubrication + smaller size)
II. Vulsellum Forceps (Tenaculum/Volsellum)
Description: A ratchet-handled forceps with paired tooth-bearing blades (usually 1x2 or 2x2 sharp interlocking teeth) used to grasp and hold the cervix.
Clinical Indications:
- Grasping the cervix to steady it during:
- D&C (dilatation and curettage)
- MTP (medical termination of pregnancy)
- Cervical biopsy
- Endometrial biopsy
- Hysteroscopy
- IUCD insertion - to straighten the uterocervical angle
- Cervical polypectomy - to grasp and twist off cervical polyps
- Trachelorrhaphy (cervical repair surgery)
- Manchester/Fothergill operation - amputation of cervix in prolapse repair
- Shirodkar suture - to grasp anterior lip of cervix
- Colposcopy-directed biopsy - cervical stabilization
Diagnostic Uses:
- Assessment of cervical mobility and tenderness (PID evaluation)
- Steadying cervix for sound insertion (uterine sounding)
- Obtaining endocervical tissue for biopsy
Contraindications:
- Carcinoma cervix (friable cervix - risk of bleeding and dissemination)
- Active cervical infection (relative)
- Uncooperative patient without anesthesia (relative)
- Pregnancy (except in specific obstetric procedures - use with extreme care)
Q7. Artava Kshaya - Samprapti, Nidana, Lakshana, and Chikitsa; Correlation with Oligomenorrhea and Hypomenorrhea
Definition
Artava Kshaya = Diminution/deficiency of Artava (menstrual blood). Artava is the Upadhatu (secondary tissue) of Rasa Dhatu. Kshaya = decrease/depletion.
Nidana (Causative Factors)
- Ahara (dietary): Excessive intake of Ruksha (dry), Laghu (light), Ushna (hot), Katu (pungent) food; inadequate nutrition; fasting
- Vihara (lifestyle): Excessive exercise, physical strain, Vegadharana (suppression of urges), Ratri Jagarana (night vigil), excessive sexual intercourse
- Manasika (psychological): Chinta (worry), Shoka (grief), Bhaya (fear) - these vitiate Vata
- Vyadhi: Rajayakshma (tuberculosis), Pandu (anemia), Shosha (cachexia)
- Vata-Pitta Dosha predominant vitiation with Rasa-Rakta Kshaya
Samprapti (Pathogenesis)
Nidana Sevana
↓
Vata-Pitta Dosha Vridhi + Rasa-Rakta Dhatu Kshaya
↓
Artava Utpatti (Artava formed from Rasa Dhatu) impaired
↓
Artava Kshaya
↓
Alpa Artava Darshana (scanty menses) / Delayed / Absent menses
The Srotas involved is Artava Vaha Srotas with Sanga (obstruction) or Kshaya (depletion) as the Sroto Dushti.
Lakshana (Clinical Features)
- Alpata - Scanty menstrual flow (< 20 mL or < 2 days)
- Krichhra Artava Pravritti - Difficult / painful menstruation
- Chirakari - Delayed onset of menstruation
- Shoola - Pelvic pain (due to Vata)
- Daurbalya - General weakness
- Shyava/Krishna Varna - Dark-colored menstrual blood
- Klama, Shrama - Fatigue
- Vandhyatva - Infertility (if severe)
- Symptoms of Rasa Kshaya: Pallor, weakness, palpitations
Chikitsa (Treatment)
Shodhana (Purification):
- Virechana (purgation) to remove excess Pitta and clear Artava Vaha Srotas
- Uttara Basti (intra-uterine/vaginal medicated enema) with Shatapushpa, Eranda, Tila taila - most important treatment
Shamana (Palliative):
- Pushyanuga Churna - classical formulation for Artava disorders
- Rajapravartini Vati - promotes menstrual flow
- Kumaryasava - tonic for Artava
- Loha Bhasma + Mandura Bhasma - for Pandu/Anemia
- Shatavari Ghrita, Ashoka Ghrita - nourish Rasa-Artava
- Ashwagandha, Shatavari - Rasayana for general strength
Pathya (Diet and lifestyle):
- Nourishing diet: milk, ghee, sesame, jaggery
- Avoid excessive exercise and fasting
- Emotional rest
Correlation with Modern Medicine
| Artava Kshaya Feature | Modern Correlation |
|---|---|
| Alpa Artava (scanty flow) | Hypomenorrhea (< 20 mL blood loss per cycle) |
| Chirakari Artava (delayed menses) | Oligomenorrhea (cycles > 35 days, < 9 cycles/year) |
| Artava Abhava (complete absence) | Amenorrhea |
Causes of Hypomenorrhea:
- Intrauterine adhesions (Asherman's syndrome)
- Endometrial atrophy
- Hormonal - hypothyroidism, hyperprolactinemia
- Post-curettage, post-myomectomy
Causes of Oligomenorrhea:
- PCOS (most common)
- Thyroid disorders
- Hyperprolactinemia
- Hypothalamic amenorrhea (stress, weight loss)
- Perimenopause
Q8. Rasayana Chikitsa - Therapeutic Role and Mechanism in Managing Rajonivrutti Vikara
Rajonivrutti (Menopause)
- Natural cessation of menstruation, typically around age 45-55
- Defined as 12 consecutive months of amenorrhea
- Due to depletion of ovarian follicles and decline in estrogen/progesterone
Rajonivrutti Vikara (Menopausal Symptoms)
- Vasomotor: Hot flashes, night sweats (Daha, Svedana)
- Psychological: Irritability, depression, mood swings (Manasika vikara)
- Urogenital atrophy: Vaginal dryness, dyspareunia, urinary incontinence
- Musculoskeletal: Osteoporosis, joint pains (Asthi-Sandhi Shoola)
- Cardiovascular: Increased risk post-menopause
- General: Fatigue, insomnia, memory decline
In Ayurveda, menopause is a Vata-Pitta dominant state with Rasa-Artava Kshaya and Ojas Kshaya.
Rasayana Chikitsa (Rejuvenation Therapy)
Definition (Charaka Samhita):
"Labhopayo hi shastaanam rasaadinaam rasayanam" - Rasayana is the science of obtaining the best qualities of Rasa (nutritive fluid) and all subsequent Dhatus.
It promotes:
- Dirgha Ayuh (longevity)
- Smriti (memory)
- Medha (intellect)
- Arogya (health)
- Yauvan (youthfulness)
- Prabha (luster)
- Varna (complexion)
- Swara (voice)
- Deha Bala (physical strength)
Mechanism of Action in Rajonivrutti Vikara
-
Dhatvagni stimulation: Rasayanas enhance the Agni (metabolic fire) at the tissue level (Dhatvagni), improving Dhatu formation - especially Rasa, Rakta, Asthi, and Shukra/Artava
-
Srotas Shodhan: Clears micro-channels blocked due to aging and Dosha accumulation, improving nutrient delivery
-
Antioxidant effect (Vaya Sthapana): Herbs like Amalaki have potent antioxidant properties, reducing cellular damage associated with aging and estrogen decline
-
Adaptogenic / Nervine tonic: Ashwagandha modulates the HPA axis, reduces cortisol, improves energy, sleep, and mood - addressing Manasika vikara
-
Phytoestrogen activity: Shatavari, Ashoka, Nagakesara - contain steroidal saponins and phytoestrogens that partially compensate for estrogen decline
-
Osteogenic activity: Guduchi, Ashwagandha support Asthi Dhatu; clinically shown to improve bone mineral density
-
Immunomodulation: Strengthen Ojas (immunity), reducing vulnerability to disease
Specific Rasayana Formulations for Rajonivrutti Vikara
| Formulation | Action |
|---|---|
| Shatavari Rasayana | Phytoestrogen, Tarpana (nourishing), relieves hot flashes, vaginal dryness |
| Ashwagandha Rasayana | Adaptogen, nerve tonic, improves sleep and mood, anti-osteoporotic |
| Amalaki Rasayana (Chyavanprash) | Antioxidant, Vayasthapana, improves immunity and strength |
| Brahmi Rasayana | Medhya (nootropic), improves memory, relieves anxiety/depression |
| Loha Rasayana / Mandura | Corrects Pandu (anemia associated with menopause) |
| Swarna Bhasma | Ojas-vardhaka, Medhya, immunomodulatory |
| Ashoka Rasayana | Acts on Artava Vaha Srotas, uterine tonic |
Panchakarma in Rajonivrutti:
- Abhyanga (oil massage): Reduces Vata, relieves joint pains and dryness
- Shirodhara: Relieves insomnia, anxiety, mood disorders
- Uttara Basti: For urogenital atrophy
- Virechana: For Pitta-dominant symptoms (hot flashes, irritability)
SECTION C - Long Answer Questions
Q.III.1. Phases of Menstrual Cycle and Role of Hypothalamo-Pituitary-Ovarian (HPO) Axis
The Normal Menstrual Cycle - Overview
- Normal cycle: 21-35 days (average 28 days)
- Duration of flow: 2-6 days
- Normal blood loss: 20-60 mL
- Two interconnected cycles: the ovarian cycle and the uterine (endometrial) cycle
THE OVARIAN CYCLE
Phase 1: Follicular Phase (Days 1-14)
- Begins from day 1 of menstruation to ovulation
- Variable in duration (accounts for cycle length variation)
Events:
- FSH rises (due to corpus luteum degeneration of previous cycle)
- A cohort of antral follicles is recruited from the ovary
- One dominant follicle is selected (by day 5-7) - secretes increasing estradiol
- Rising estrogen causes endometrial proliferation
- Estrogen provides negative feedback on FSH (FSH falls mid-follicular phase)
- Follicle produces inhibin B - further suppresses FSH
- LH shows paradoxical biphasic response: first inhibited by estrogen, then dramatically stimulated (positive feedback) as estrogen peaks late in follicular phase
Ovulation (Day 14 in 28-day cycle)
- Triggered by the LH surge (begins ~36 hours before ovulation)
- LH surge causes:
- Resumption of meiosis I in the oocyte
- Prostaglandin synthesis - follicular rupture
- Luteinization of granulosa cells
- Oocyte released; follicle collapses and transforms to corpus luteum
Phase 2: Luteal Phase (Days 14-28)
- Fixed duration: 14 days
- Corpus luteum secretes progesterone, estradiol, and inhibin A
- Progesterone causes secretory transformation of endometrium (prepares for implantation)
- Progesterone + estrogen + inhibin A suppress LH and FSH (negative feedback)
- If no implantation: corpus luteum degenerates (luteolysis) by day 24-26 - progesterone falls - menstruation occurs
THE UTERINE (ENDOMETRIAL) CYCLE
Phase 1: Menstrual Phase (Days 1-4)
- Progesterone and estrogen fall → withdrawal of hormonal support
- Endometrial spiral arteries spasm → ischemia → endometrial shedding
- Prostaglandins mediate uterine contractions (cause dysmenorrhea)
- Shed endometrium, blood, and tissue pass as menstrual fluid
Phase 2: Proliferative Phase (Days 4-14)
- Driven by rising estrogen from developing follicle
- Endometrium regenerates from the basal layer (stratum basalis)
- Glands become straight, stroma proliferates
- Endometrium grows from ~0.5 mm to 3-5 mm
Phase 3: Secretory Phase (Days 14-28)
- Driven by progesterone (from corpus luteum)
- Endometrial glands become tortuous ("saw-tooth" on histology)
- Glands secrete glycogen-rich fluid - "uterine milk"
- Spiral arteries lengthen
- Endometrium reaches 6-10 mm (maximum)
- If fertilized ovum implants (day 7-10 post-ovulation): hCG is secreted → rescues corpus luteum → progesterone maintained → no menstruation (pregnancy)
ROLE OF THE HYPOTHALAMO-PITUITARY-OVARIAN (HPO) AXIS
HYPOTHALAMUS
| GnRH (pulsatile, from arcuate nucleus)
↓
ANTERIOR PITUITARY
| FSH + LH (pulsatile)
↓
OVARY
| Estradiol, Progesterone, Inhibin A/B
↓
FEEDBACK to hypothalamus and pituitary
Key Feedback Mechanisms:
| Mechanism | Hormone | Effect |
|---|---|---|
| Negative feedback (follicular) | Rising estrogen | Suppresses FSH |
| Negative feedback (luteal) | Progesterone + Estrogen + Inhibin A | Suppresses LH + FSH |
| Positive feedback | High-sustained estrogen (late follicular) | TRIGGERS LH surge → ovulation |
| Inhibin B | From granulosa cells (follicular phase) | Specifically suppresses FSH |
| Inhibin A | From corpus luteum (luteal phase) | Suppresses FSH in luteal phase |
GnRH Pulse Frequency Significance:
- Slow pulses (1/90 min) → favor FSH secretion
- Fast pulses (1/60 min) → favor LH secretion
- Continuous (non-pulsatile) GnRH → downregulates GnRH receptors → suppresses both FSH and LH (basis of GnRH agonist therapy)
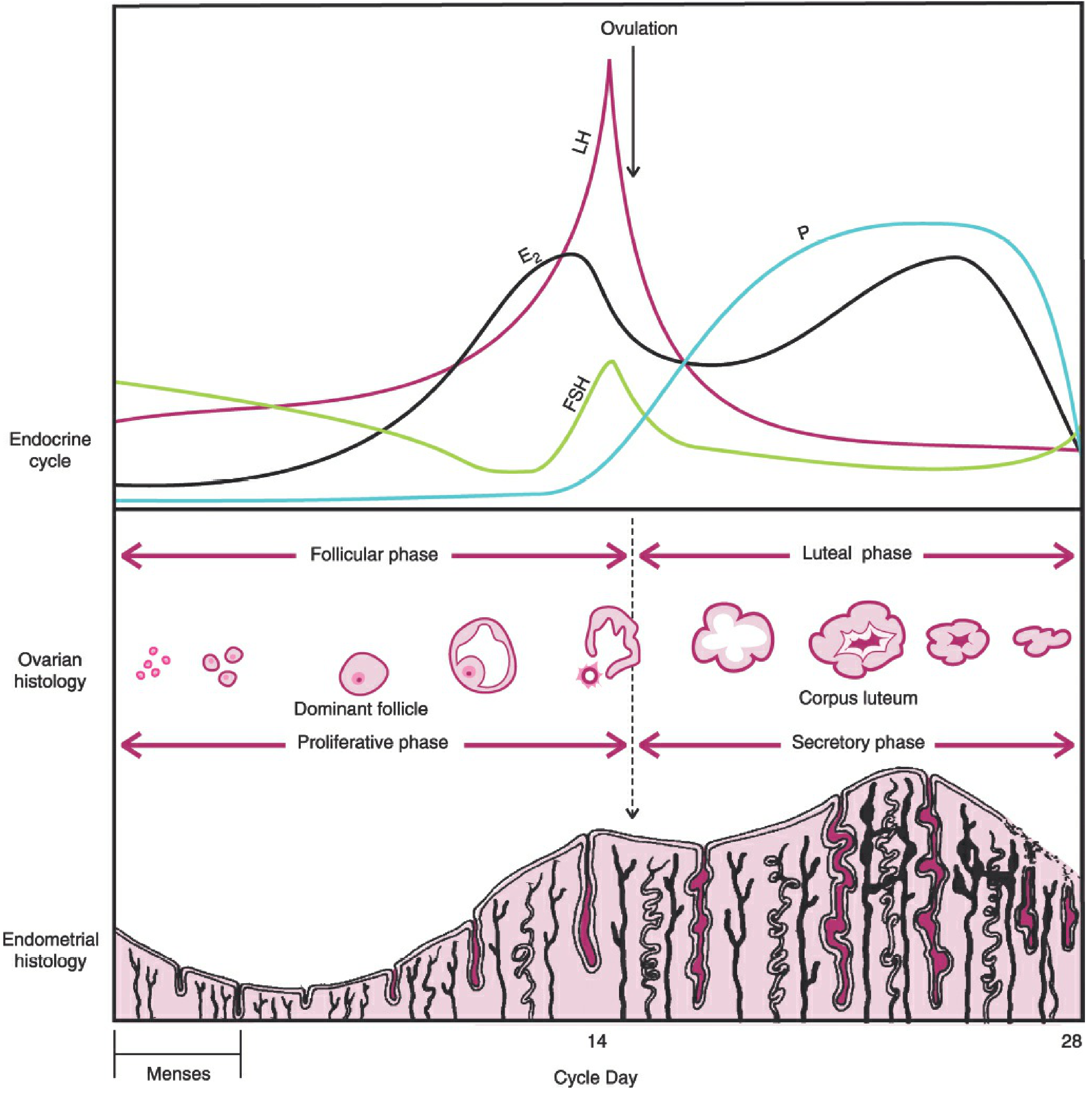
(From Berek & Novak's Gynecology - cyclical changes in hormones over 28-day cycle divided into follicular and luteal phases)
Q.III.2. Masanumasika Garbhini Paricharya - Month-Wise Antenatal Regimen with Clinical Relevance
Definition: Masanumasika = month-by-month; Garbhini = pregnant woman; Paricharya = regimen/care. This is the Ayurvedic month-wise antenatal protocol, described in Charaka Samhita (Sharira Sthana 4/14-22) and Ashtanga Hridayam (Sharira Sthana).
Rationale
The fetus develops progressively each month. The dietary and therapeutic regimen is prescribed to:
- Nourish the growing fetal structures (Poshana)
- Maintain maternal health (Matru Swasthya)
- Ensure optimal labor and delivery
- Prevent pregnancy complications
Month-Wise Regimen
| Month | Fetal Development (Garbha Vridhi) | Prescribed Regimen | Clinical Relevance |
|---|---|---|---|
| 1st Month | Kalala (undifferentiated mass) - all Panchamahabhutas present | Cool, sweet, liquid diet (Madhura Sheeta Drava Ahara); Cow's milk plain or with sweet herbs | Prevents miscarriage; combats nausea; folic acid equivalent |
| 2nd Month | Ghana (solid mass; all tissues beginning to form) | Milk medicated with sweet herbs (Madhura Gana drugs) | Supports organogenesis; antiemetic |
| 3rd Month | Anga Pradesha (limb buds form; gender differentiation begins) | Milk + honey + ghee (Kshira-Madhu-Ghrita); Yava (barley), Shashtika rice | Limb formation supported; prevents Dauhrida-related complications |
| 4th Month | Sthira (firm body; cardiac activity felt); Fetus first expresses its desires (Dauhrida) | Butter (Navanita) + milk; granting of Dauhrida (fetal wishes) | Cardiac development; failure to honor Dauhrida → Kubjata (hunchback), Khanja (lame), Muta (mute) fetus |
| 5th Month | Manas (mind develops) | Milk + Ghrita + meat soup (Mamsa Rasa) | Neurological development; prevents Pandu and emaciation |
| 6th Month | Bal (strength develops); Tridosha active | Milk medicated with Prithak Parnyadi group (Gokshura, Bala); Ghrita with Madhura drugs; Bala Taila massage | Renal development; prevents Shotha (edema); prevents IUGR |
| 7th Month | Sarva Anga Sampurnata (all organs complete); Ojas transferred to fetus | Anuvasana Basti with Bala Taila; Ghrita with Madhura drugs; Milk | Prevents premature labor; ensures Ojas transfer; nourishes fetus |
| 8th Month | Ojas oscillates between mother and fetus (Adana-Pradana of Ojas) | Milk alone (simple nourishing diet only); Avoid Basti; keep calm | Ojas is unstable - interventions, stress, travel contraindicated; correlates with increased risk at 8 months gestation |
| 9th Month | Full term (Paripakva Garbha) | Basti with medicated oil/ghee (Sneha Basti, Anuvasana Basti); Vaginal application of oils (Pichu with Bala Taila, Shatpushpa Taila) | Prepares birth canal; lubricates perineum; prevents perineal tears; induces labor readiness; relaxes pelvic muscles |
| 10th Month | Delivery expected (Charaka counts 10 lunar months) | Continue Anuvasana Basti; active monitoring; diet of Mudga (green gram), rice, soup | Normal delivery; prevents dystocia |
Special Practices in Garbhini Paricharya
Garbhini Paricharya also includes:
- Pumsavana (2nd-3rd month) - ritual for fetal sex/health promotion
- Simantaonnayana (4th-5th month) - ceremony to honor mother and fetus
- Manasa Paricharya: Avoid anger, fear, grief; engage in devotion, pleasant activities (Sattvik mental regimen)
- Vihara (Behavioral rules):
- Avoid heavy lifting, strenuous exercise
- Avoid sitting on hard surface
- Sleep on left lateral position (Vama Parshva Shayan)
- Avoid Vegadharana
- Daily gentle walking (Manda Gati)
- Avoid: Alcohol, smoking, Tikta-Katu food, fasting, excessive travel, sexual intercourse (especially in 1st and 9th months)
Clinical Correlation of Masanumasika Paricharya
| Ayurvedic Practice | Modern Clinical Equivalent |
|---|---|
| Milk + folic acid herbs (1st month) | Folic acid supplementation (prevents NTDs) |
| Granting Dauhrida (4th month) | Addressing food cravings; nutritional counseling |
| Avoidance of stress | Mental health care in antenatal period |
| Anuvasana Basti (9th month) | Perineal massage with oils (reduces tears) |
| 8th month caution | High-risk period monitoring |
| Avoiding intercourse in 1st trimester | Sexual restriction advice in threatened abortion |
Q.III.3. Asrugdara - Nidana, Samprapti, Lakshana, and Chikitsa; Correlation to AUB
Definition
Asrugdara = "Asruk" (blood) + "Dara" (to flow/gush forth) = Abnormal/excessive uterine bleeding. It is described by Charaka and Sushruta as excess Artava flow. Corresponds to modern Abnormal Uterine Bleeding (AUB).
Nidana (Etiology)
Ahara Nidana:
- Excessive intake of Amla (sour), Lavana (salty), Katu (pungent), Ushna (hot), Tikshna foods
- Excessive alcohol (Sura), fermented foods
- Meat of aquatic/marshy animals
Vihara Nidana:
- Atiyoga of Maithuna (excessive intercourse)
- Excessive strenuous exercise and jumping
- Pressure injuries, trauma to abdomen
Manasika Nidana:
- Krodha (anger), Shoka (grief), Chinta (anxiety) - vitiate Pitta and Rakta
Vyadhija Nidana:
- Pradara in the context of Garbhashaya roga (uterine diseases)
- Raktaj Gulma (blood tumor - possibly fibroid/polyp)
Samprapti (Pathogenesis)
Nidana Sevana (especially Pitta/Rakta aggravating causes)
↓
Pitta Dosha vridhi + Rakta Dhatu Dushti
↓
Pitta enters Rakta (Pitta-Rakta Sammurchhana)
↓
Artava Vaha Srotas Dushti (especially by Atipravrutti type)
↓
Teekshna, Ushna, Drava properties of Pitta → Rakta Atipravrutti
↓
Asrugdara (Excessive uterine bleeding)
Types of Asrugdara (based on Dosha):
- Vataj Asrugdara: Dark/blackish, frothy blood; Severe pain; irregular; thin
- Pittaj Asrugdara: Bright red, warm blood; burning sensation; continuous flow
- Kaphaj Asrugdara: Pale/whitish blood; slimy, heavy; mild pain
- Sannipataj: Mixed features; most serious
Lakshana (Clinical Features)
- Atyartava - Excessive menstrual flow (> 80 mL)
- Atidirghakala - Prolonged bleeding (> 7 days)
- Akala Artava - Bleeding at irregular times (intermenstrual)
- Daurbalya - General weakness
- Panduta - Pallor (anemia)
- Hridrava - Palpitations
- Bhrama - Dizziness
- Trishna - Excessive thirst
- Klama, Shrama - Fatigue
- Mukha Vaivarnya - Facial discoloration
Chikitsa (Treatment)
Principle: Raktasthambhana (hemostasis) + Pitta-Rakta Shamana + Rakta-Rasa Poshan (rebuild blood)
Shodhana:
- Virechana (purgation) - removes excess Pitta; most important
- Rakta Mokshana (blood-letting) - only in extreme Pitta-Rakta Dushti
Shamana (Internal Medicines):
- Pushyanuga Churna - classical first-line for all types of excessive vaginal discharge/bleeding
- Chandraprabha Vati - reduces uterine inflammation
- Ashoka Ghrita / Ashoka Arishtam - Ashoka bark is the primary drug (Saraka asoka = Ashoka); hemostatic, uterine tonic
- Lodhra Churna - astringent, hemostatic
- Nagakesara - specific for Pittaj Asrugdara (hemostatic + anti-inflammatory)
- Dhatri Loha / Mandura - for associated Pandu (anemia)
- Bolbaddha Rasa - for acute hemorrhage
Uttara Basti: Medicated enema via the cervical/vaginal route with Shatapushpa + Tila oil for uterine srotas cleansing.
Correlation with AUB (Abnormal Uterine Bleeding)
Modern AUB Classification (PALM-COEIN - FIGO 2011):
| Structural Causes (PALM) | Functional Causes (COEIN) |
|---|---|
| Polyp | Coagulopathy |
| Adenomyosis | Ovulatory dysfunction |
| Leiomyoma (fibroid) | Endometrial dysfunction |
| Malignancy/hyperplasia | Iatrogenic |
| Not otherwise classified |
| Asrugdara Type | AUB Correlation |
|---|---|
| Heavy menstrual flow | HMB (Heavy Menstrual Bleeding) = Menorrhagia |
| Irregular/intermenstrual | IMB (Intermenstrual Bleeding) = Metrorrhagia |
| Both heavy + irregular | Menometrorrhagia |
| Raktaj Gulma causing bleeding | Fibroid/polyp-related AUB |
| Pittaj + Pitta-Rakta | Coagulopathy, DIC |
Q.III.4. Artava Dushti as Described by Acharya Sushruta - Types, Lakshanas, and Chikitsa Siddhanta
Definition
Artava = Menstrual blood (also used for ovum/reproductive fluid in broader context)
Dushti = Vitiation/pathological alteration
Acharya Sushruta described Artava Dushti in Sushruta Samhita - Sharira Sthana Chapter 2 and Chikitsa Sthana, wherein he classified the types based on Dosha predominance.
Types of Artava Dushti According to Sushruta
Sushruta classifies 20 types of Yonivyapad (uterovaginal disorders) in which Artava Dushti is implicitly described, and separately addresses Artava Dushti in the context of Garbha formation defects.
Primary Classification - Dosha-wise:
1. Vataj Artava Dushti:
| Feature | Description |
|---|---|
| Varna (Color) | Krishna (dark/black), Aruna (reddish-dark), Shyava |
| Consistency | Phena (frothy), Shushka (dry), Tanu (thin/watery) |
| Smell | Phenila (foamy), Matsya Gandha (fishy) |
| Symptoms | Toda (pricking pain), Shoola (colic), Rukshata (dryness), Karshaniya (emaciating) |
| Quantity | Alpa (scanty) or intermittent |
2. Pittaj Artava Dushti:
| Feature | Description |
|---|---|
| Varna (Color) | Peeta (yellow), Neela (blue-black), Haridra (turmeric-yellow) |
| Consistency | Ushna (hot), Drava (liquid), Puya-like (purulent) |
| Smell | Amla Gandha (sour/acidic), Durgandhi (offensive) |
| Symptoms | Daha (burning), Kleda (wetness/moisture), Arsha (piles-like), Trushna (thirst) |
| Quantity | Excessive |
3. Kaphaj Artava Dushti:
| Feature | Description |
|---|---|
| Varna (Color) | Pandu (pale), Shveta (white), Avadatta (normal color but abnormal) |
| Consistency | Snigdha (oily), Guru (heavy), Pichchila (slimy/mucoid) |
| Smell | Madhura Gandha (sweet smell) |
| Symptoms | Kandu (itching), Nistoda (dull pain), Sthaimithya (heaviness) |
| Quantity | Excess, prolonged |
4. Sannipataj (Tridosha) Artava Dushti:
- Mixed features of all three
- Most difficult to treat
- Corresponds to complex AUB or mixed infection
5. Raktaj Artava Dushti (Sushruta-specific):
- Sushruta specifically mentions Raktaj Pradara separately
- Features: Bright red, hot, coppery smell (Tamra Gandha)
- Due to pure Rakta Dushti (blood vitiation)
Lakshanas (Signs and Symptoms of Artava Dushti)
- Artava Vaivarnya - change in color of menstrual blood
- Artava Vaishamya - irregularity in amount and timing
- Artava Durgandha - foul smell
- Artava Vikara - abnormal consistency (clots, frothy, slimy)
- Associated Vedana (pain), Daha, Kandu
- Systemic symptoms: Pandu, Daurbalya, Bhrama
Artava Dushti and Garbha Dosha (Congenital defects):
Sushruta states that vitiated Artava affects the quality of conception:
- Vataj Artava Dushti → Vata-predominant defects in fetus (sensory/motor)
- Pittaj → Jaundice, skin disorders in newborn
- Kaphaj → Sluggish, heavy-built child with Shleshma disorders
- This is clinically relevant: maternal conditions like infection, nutritional deficiency, and hormonal disorders can cause fetal abnormalities
Chikitsa Siddhanta (Treatment Principles - Sushruta's Approach)
General Principle: Correct the underlying Dosha vitiation, purify Artava Vaha Srotas, and restore normal Artava.
Vataj Artava Dushti:
- Snehana (oil therapy) - internal and external
- Vata-pacifying diet: milk, ghee, Bala, Ashwagandha
- Anuvasana Basti with medicated oils
- Shatavari Ghrita
Pittaj Artava Dushti:
- Virechana (purgation) - primary Shodhana
- Pitta-pacifying diet: cool, sweet, bitter foods
- Chandanasava, Usheerasava, Sarivadyasava
- Nagakesara, Lodhra, Praval Pishti
Kaphaj Artava Dushti:
- Langhana (lightening therapy), Ruksha Udavartana
- Kapha-pacifying: light, dry, pungent foods
- Trikatu, Triphala, Guggulu preparations
- Kanchanara Guggulu (for Kapha-type uterine growths)
Raktaj Artava Dushti:
- Rakta-sthambhana herbs: Lodhra, Nagakesara, Chandana, Mocharasa
- Rakta Shodhana: Sariva (Hemidesmus), Nimba, Patola
- Pushyanuga Churna, Ashoka preparations
Uttara Basti (Sushruta's own emphasis):
- Medicated oil/ghee introduced via vaginal/uterine route
- Directly acts on Artava Vaha Srotas
- Both diagnostic (assesses Yoni type) and therapeutic
- Most cited treatment for all Artava-related disorders
Pathya (Diet and Conduct for all Artava Dushti):
- Avoid spicy, sour, fermented, hot foods
- Avoid excessive exercise, sexual intercourse during treatment
- Mental peace, sattvic lifestyle
- Regular sleep and meal times
- Tila (sesame), Mudga (green gram), Yava (barley) as staple grains
Sources: Charaka Samhita (Sharira Sthana, Chikitsa Sthana), Sushruta Samhita (Sharira Sthana, Chikitsa Sthana), Ashtanga Hridayam (Sharira Sthana), Berek & Novak's Gynecology (for modern clinical correlations), Costanzo Physiology, Medical Physiology (Boron & Boulpaep) - for HPO axis and menstrual cycle physiology.
This is a shared conversation. Sign in to Orris to start your own chat.