Thyroiditis in detail
Reading File
Finding Sources
Searching PubMed
thyroiditis classification diagnosis treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
Hashimoto thyroiditis histology lymphocytic infiltration
Reading File
Searching Images
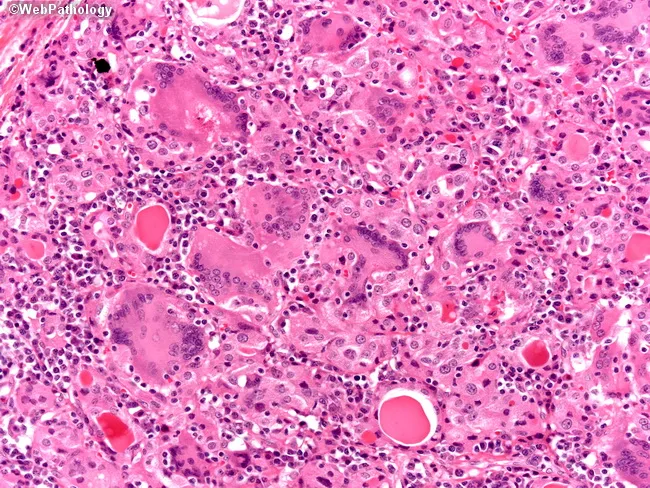
subacute granulomatous de Quervain thyroiditis giant cells
Reading File
Reading File
I now have comprehensive, multi-source content to write a detailed answer. Let me compose it:
Thyroiditis — A Comprehensive Overview
Thyroiditis refers to a heterogeneous group of disorders characterized by thyroid inflammation. They differ in etiology, clinical course, thyroid function changes, histology, and management.
Classification
Thyroiditis is best classified by onset/duration and presence or absence of pain (Harrison's 22e):
| Category | Subtypes |
|---|---|
| Acute | Suppurative (bacterial/fungal), Radiation, Amiodarone |
| Subacute | Viral (de Quervain), Silent (including postpartum), Drug-induced (IFN, TKIs, immune checkpoint inhibitors) |
| Chronic | Hashimoto's, Atrophic, Riedel's, Parasitic |
1. Hashimoto Thyroiditis (Chronic Lymphocytic Thyroiditis)
Epidemiology
- Most common cause of hypothyroidism in iodine-sufficient regions
- Peak incidence: 45–65 years
- Female predominance: 10:1 to 20:1
- Can affect children (major cause of non-endemic goiter in pediatrics)
- First described by Hakaru Hashimoto in 1912 (struma lymphomatosa)
Pathogenesis
A breakdown of self-tolerance to thyroid autoantigens via multiple immunological mechanisms:
- CD8+ cytotoxic T cells directly kill thyroid follicular cells
- CD4+ Th1 cells produce IFN-γ → macrophage activation → follicular damage
- Antithyroid antibodies (anti-TPO, anti-Tg): may damage follicular cells via complement-dependent or antibody-dependent cellular cytotoxicity (role as cause vs. consequence is debated)
Genetic susceptibility: Polymorphisms in CTLA4, PTPN22, and IL2RA (all regulators of T-cell responses) increase risk — same genes implicated in Graves disease.
Morphology (Histology)
- Diffuse, pale-yellow, firm, well-demarcated goiter
- Dense lymphoplasmacytic infiltrate with germinal center formation
- Thyroid follicles are atrophic
- Follicular epithelial cells undergo Hürthle (oncocytic) cell change — eosinophilic granular cytoplasm representing metaplasia under chronic injury
- Variable fibrosis

Clinical Presentation
- Initially: firm, symmetric goiter (lobulated, may mimic MNG)
- Gradually: gland atrophies → overt hypothyroidism
- Symptoms of hypothyroidism: fatigue, cold intolerance, constipation, weight gain, dry skin, bradycardia
Laboratory & Investigations
| Test | Findings |
|---|---|
| Anti-TPO antibodies | Positive in ~90% |
| Anti-Tg antibodies | Positive in 20–50% |
| TSH | Elevated (subclinical → overt hypothyroidism) |
| T4, T3 | Low in overt hypothyroidism |
| Thyroid ultrasound | Hypoechoic, heterogeneous texture; lobulated gland |
Progression: TSH rises first (subclinical hypothyroidism) → then T4 falls → T3 falls last (thyroid failure)
Complications
- Primary B-cell lymphoma of the thyroid (rare but strongly associated) — MALT or DLBCL; results from chronic B-cell stimulation
- Increased frequency of papillary thyroid carcinoma, particularly in women
- FNA biopsy needed to distinguish from lymphoma
Treatment
- Overt hypothyroidism or subclinical hypothyroidism with high antibody titers: levothyroxine (target: normalize TSH)
- TSH-suppressive doses may be used short-term to reduce goiter size
- Monitor with TSH
2. Subacute Granulomatous Thyroiditis (de Quervain / Viral / Painful Thyroiditis)
Etiology & Epidemiology
- Most common cause of painful thyroid
- Accounts for up to 5% of clinical thyroid disorders
- Incidence: 5× more common in women; peak in 4th–5th decades (Harrison: 30–50 years)
- Viral trigger (mumps, coxsackievirus, influenza, adenoviruses, echoviruses, SARS-CoV-2, post-COVID vaccine)
- Occurs seasonally coinciding with enterovirus peak
- HLA-B35 association
Pathophysiology
Viral injury → follicular rupture → granulomatous inflammation → release of preformed thyroid hormones into circulation → transient thyrotoxicosis → hormone depletion → transient hypothyroidism → recovery (euthyroidism in most)
Histology
- Foreign-body giant cells surrounding disrupted follicles containing colloid
- Epithelioid histiocyte aggregates (granulomas)
- Dense lymphoplasmacytic infiltrate
- Follicular architecture disrupted; no caseous necrosis (distinguishes from TB)
Clinical Features
- Onset 2–3 weeks after upper respiratory tract infection
- Neck pain: moderate to severe, may radiate to jaw, ear, or anterior chest; may migrate from one lobe to the other
- Fever, myalgias, fatigue
- Firm, exquisitely tender thyroid on palpation
- No cervical lymphadenopathy
- ~50% have symptoms of thyrotoxicosis (palpitations, heat intolerance, tremor)
Phases
| Phase | Duration | TSH | T4/T3 | Symptoms |
|---|---|---|---|---|
| Thyrotoxic | 2–4 months | ↓ (suppressed) | ↑ (T4:T3 ratio >20) | Palpitations, heat intolerance |
| Euthyroid (transitional) | 1–2 months | Normal | Normal | Asymptomatic |
| Hypothyroid | Up to 6–9 months | ↑ | ↓ | Fatigue, cold intolerance |
| Recovery | — | Normalizes | Normalizes | Full recovery in ~95% |
The T4:T3 ratio >20 (reflecting stored hormone ratios) distinguishes from Graves disease, where T3 is preferentially elevated.
Investigations
| Test | Result |
|---|---|
| ESR | Markedly elevated (hallmark during painful phase) |
| WBC | Normal or mildly elevated |
| Anti-TPO / Anti-Tg | Usually negative (unlike Hashimoto's) |
| TRAb | Negative (distinguishes from Graves) |
| Radioactive iodine uptake (RAIU) | Low to undetectable during thyrotoxic phase |
| Ultrasound | Hypoechoic regions; decreased Doppler flow |
| Serum thyroglobulin | Elevated (early biomarker of inflammatory thyroiditis) |
Treatment
- β-blockers (e.g., atenolol 25–50 mg/day) for thyrotoxic symptoms — antithyroid drugs are contraindicated (no excess synthesis)
- NSAIDs for mild-moderate pain
- Prednisone 40–60 mg/day with slow taper over ≥4–6 weeks for severe pain (taper slowly to prevent recurrence)
- Levothyroxine if symptomatic hypothyroidism develops (weight-based if overt; low-dose if subclinical)
- Prognosis: ~95% achieve full recovery; permanent hypothyroidism in a minority
3. Silent / Painless Thyroiditis (Subacute Lymphocytic Thyroiditis)
Includes:
- Sporadic silent thyroiditis — occurs outside pregnancy
- Postpartum thyroiditis — occurs within 12 months of delivery
Epidemiology
- Postpartum thyroiditis: 4–10% of pregnancies
- In women TPO-antibody positive in first trimester: 50% develop postpartum thyroiditis
- Sporadic: age 30–60 years; 1.5× more frequent in women
- Postpartum incidence ~20× higher than Graves disease postpartum
Pathophysiology
- Autoimmune destruction; similar to Hashimoto's but transient
- HLA haplotype associations
- Lymphocyte and complement-mediated damage
- Release of preformed hormones → destruction-induced thyrotoxicosis
Clinical Patterns (Postpartum)
- ~20%: triphasic — thyrotoxicosis → euthyroid → hypothyroidism
- ~50%: isolated hypothyroidism only
- ~30%: isolated thyrotoxicosis only
- Thyrotoxic phase: usually mild, relatively asymptomatic; nontender goiter
- Toxic phase: 1–3 months; hypothyroid phase: up to 1 year
Key Differentiating Features from Graves Disease
| Feature | Silent/Postpartum Thyroiditis | Graves Disease |
|---|---|---|
| Pain | None | None |
| TRAb | Negative | Positive |
| T3:T4 ratio | Low (<20) | High (T3 dominant) |
| RAIU | Low | High |
| Color Doppler | Decreased flow | Markedly increased flow |
| Exophthalmos/bruit | Absent | May be present |
| Anti-TPO | Usually positive | Sometimes positive |
Treatment
- Thyrotoxic phase: β-blockers if symptomatic; antithyroid drugs contraindicated
- Hypothyroid phase: Levothyroxine if TSH >10 mIU/L or symptomatic
- Long-term risk: up to 30–50% of women remain hypothyroid at 1 year; annual TSH monitoring recommended
- Associated conditions: Graves disease, type 1 diabetes, SLE, chronic viral hepatitis
4. Acute (Suppurative) Thyroiditis
Etiology
- Rare; bacterial, fungal, or parasitic infection of the thyroid
- Common pathogens: Staphylococcus, Streptococcus, Enterobacter, Aspergillus, Candida, Histoplasma, Pneumocystis
- In children/young adults: piriform sinus fistula (remnant of 4th branchial pouch, predominantly left-sided)
- In elderly: pre-existing goiter, malignancy degeneration
Clinical Features
- Thyroid pain radiating to throat or ears
- Fever, dysphagia, erythema overlying the thyroid
- Small, tender, possibly asymmetric goiter
- Systemic febrile illness, lymphadenopathy
- Thyroid function usually normal
Investigations
- ESR and WBC elevated
- FNA biopsy: PMN infiltration; culture identifies organism
- CT/ultrasound: to localize abscess
Complications
- Tracheal obstruction, septicemia, retropharyngeal abscess, mediastinitis, jugular venous thrombosis
Treatment
- Antibiotics guided by Gram stain and culture
- Surgical drainage if abscess present
- Immunocompromised patients: rule out fungal/mycobacterial/Pneumocystis thyroiditis
5. Riedel Thyroiditis (Chronic Fibrous Thyroiditis / Riedel Disease)
- Extremely rare: 0.05% of thyroid disease
- Dense fibrosis replacing thyroid tissue and invading adjacent structures (trachea, esophagus, vessels)
- Now recognized as part of the IgG4-related systemic sclerosing disease spectrum
- Histology: lymphocytes, plasma cells, and dense fibrosis
- Presentation: rock-hard thyroid, tracheal compression, dysphagia
- Most patients euthyroid initially → hypothyroidism as fibrosis progresses
- Thyroid antibodies may be present
- Diagnosis: open (surgical) biopsy (FNA usually insufficient through dense fibrous tissue)
- Treatment: Surgery (to relieve compression); immunosuppressants (tamoxifen, steroids) effective in early disease
6. Drug-Induced Thyroiditis
| Drug | Mechanism | Type |
|---|---|---|
| Amiodarone | Iodine excess + direct toxicity | Can be subacute or chronic |
| Interferon-α | Immune activation | Hashimoto-like or silent |
| Tyrosine kinase inhibitors (sorafenib, sunitinib) | Immune dysregulation | Destructive |
| Immune checkpoint inhibitors (anti-PD-1, anti-CTLA-4) | T-cell disinhibition | Destructive thyroiditis |
Comparative Summary
| Feature | Hashimoto | Subacute (de Quervain) | Silent/Postpartum | Acute Suppurative | Riedel |
|---|---|---|---|---|---|
| Pain | No | Yes | No | Yes | Variable (compressive) |
| Autoimmune | Yes | No | Yes | No | Partially (IgG4) |
| Course | Chronic → hypothyroid | Self-limited | Self-limited | Acute | Progressive fibrosis |
| Anti-TPO | >90% | Usually negative | Usually positive | Negative | Variable |
| ESR | Normal/mildly elevated | Markedly elevated | Normal/mild | Elevated | Normal |
| RAIU | Low-normal | Very low | Very low | Normal | Low if hypothyroid |
| Treatment | Levothyroxine | NSAIDs/steroids, β-blockers | β-blockers, LT4 if needed | Antibiotics ± surgery | Surgery ± immunosuppressants |
Key Points to Remember
- Most common thyroiditis: Hashimoto's (most common cause of hypothyroidism in iodine-sufficient countries)
- Most common painful thyroiditis: de Quervain's
- Transient thyrotoxicosis + low RAIU = destructive thyroiditis (de Quervain, silent, postpartum) — never treat with antithyroid drugs
- Anti-TPO positive + TRAb negative + low RAIU: favors silent/postpartum thyroiditis over Graves
- Riedel thyroiditis: IgG4-related; mimics malignancy clinically; diagnose by open biopsy
- Piriform sinus fistula: structural predisposition to acute suppurative thyroiditis in children
- Postpartum thyroiditis: annual TSH monitoring for life after episode
Sources: Harrison's Principles of Internal Medicine 22e; Robbins, Cotran & Kumar Pathologic Basis of Disease; Robbins & Kumar Basic Pathology; Goldman-Cecil Medicine International Edition; Tietz Textbook of Laboratory Medicine 7e
This is a shared conversation. Sign in to Orris to start your own chat.