Lumbar radiculopathy
Reading File
Finding Sources
Searching PubMed
"lumbar radiculopathy" AND management
Searching the Web
lumbar radiculopathy clinical features diagnosis treatment 2025
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
I now have comprehensive material from multiple authoritative textbooks plus recent systematic reviews. Here is the full structured answer:
Lumbar Radiculopathy
Definition
Lumbar radiculopathy is a condition in which a disease process impairs the function of one or more lumbosacral nerve roots, producing pain, sensory disturbance, and/or motor weakness in the back, buttock, or lower extremity. The term "sciatica" is commonly used when the sciatic distribution (L4-S1) is involved. - Adams and Victor's Principles of Neurology, 12th Ed.
Anatomy and Pathophysiology
The lumbar spine has five movable vertebral bodies (L1-L5). Each neural foramen lies just below the vertebra of the same number. Nerve roots are most commonly compressed at three sites:
- Within the thecal sac
- In the lateral recess, as the root exits the thecal sac
- As it traverses the neural foramen
Common causes:
- Herniated nucleus pulposus - by far the most common cause; pain occurs when disc material makes direct contact with a root and triggers inflammation
- Spondylosis / degenerative osteoarthritis - osteophytes and degenerative changes narrow the canal; roots are compressed between the posterior vertebral body, the facet joint laterally, and the ligamentum flavum posteriorly
- Lateral recess stenosis - a common feature of spondylotic change, sometimes the dominant mechanism
- Spondylolisthesis - forward slip of one vertebra on another; L5 > L4 most often
- Less common: epidural abscess, metastatic tumor, epidural hematoma, piriformis syndrome, pelvic mass
95% of clinically significant lumbar disc herniations occur at L4-L5 or L5-S1. - Symptom to Diagnosis, 4th Ed.
Clinical Features
Symptoms
- Moderate to severe pain radiating from the back through the buttock and down the leg, often to the foot or ankle (sciatica)
- Pain is sharp, shooting, burning, or electric; may also be described as throbbing, tingling, or dull
- Radicular pain is aggravated by coughing, sneezing, Valsalva, prolonged sitting, or lifting - all of which increase intrathecal/disc pressure
- Associated numbness, paresthesias, or weakness in the distribution of the affected root
Root-Level Localisation
| Nerve Root | Pain Distribution | Paresthesias / Sensory Loss | Motor Weakness | Absent Reflex |
|---|---|---|---|---|
| L4 | Anteromedial thigh | Medial lower leg | Knee extension, hip adduction | Knee (patellar) |
| L5 | Lateral thigh, lateral lower leg, dorsum of foot | Same | Foot dorsiflexion, eversion/inversion, hip abduction | None (or tibialis posterior) |
| S1 | Posterior thigh, calf, heel | Sole, lateral foot, 4th/5th toes | Foot plantar flexion, knee flexion, hip extension | Ankle (Achilles) |
Symptom to Diagnosis, 4th Ed.
Neurogenic Claudication (Lumbar Canal Stenosis)
A distinctive syndrome in which standing or walking provokes gradual numbness and weakness of the legs, with asymmetric sciatic, calf, or buttock discomfort. Relief occurs by sitting, squatting, or bending forward (which elongates the lumbar spine). Ankle reflexes may disappear after walking and return on flexion. Distinguished from vascular claudication by:
- Appears with standing even before walking
- Relief by forward flexion (not just rest)
- Prominent numbness component
- Normal distal pulses
- Loss of ankle reflexes
Adams and Victor's Principles of Neurology, 12th Ed.
Cauda Equina Syndrome (Emergency)
A large central disc herniation can compress the entire cauda equina, producing:
- Intense bilateral low back and sciatic pain
- Incomplete bilateral leg weakness (paraparesis)
- Loss of both ankle jerks
- Urinary retention or incontinence
- Saddle anesthesia
This requires urgent surgical decompression.
Physical Examination
Key maneuvers:
- Straight Leg Raise (SLR, Lasègue sign): With the patient supine, passive elevation of the extended leg to 30-70° reproduces radicular leg pain. More sensitive but less specific for disc herniation
- Crossed SLR (contralateral SLR): Elevation of the asymptomatic leg reproduces pain on the affected side - less sensitive but more specific for large herniations
- Femoral stretch test: Hip extension with knee flexion - exacerbates upper lumbar radiculopathy (L2-L4)
- Neurologic testing: assess strength (heel walk / toe walk), sensation in dermatomes, deep tendon reflexes
Rosen's Emergency Medicine, 10th Ed.; Bradley & Daroff's Neurology in Clinical Practice
Investigations
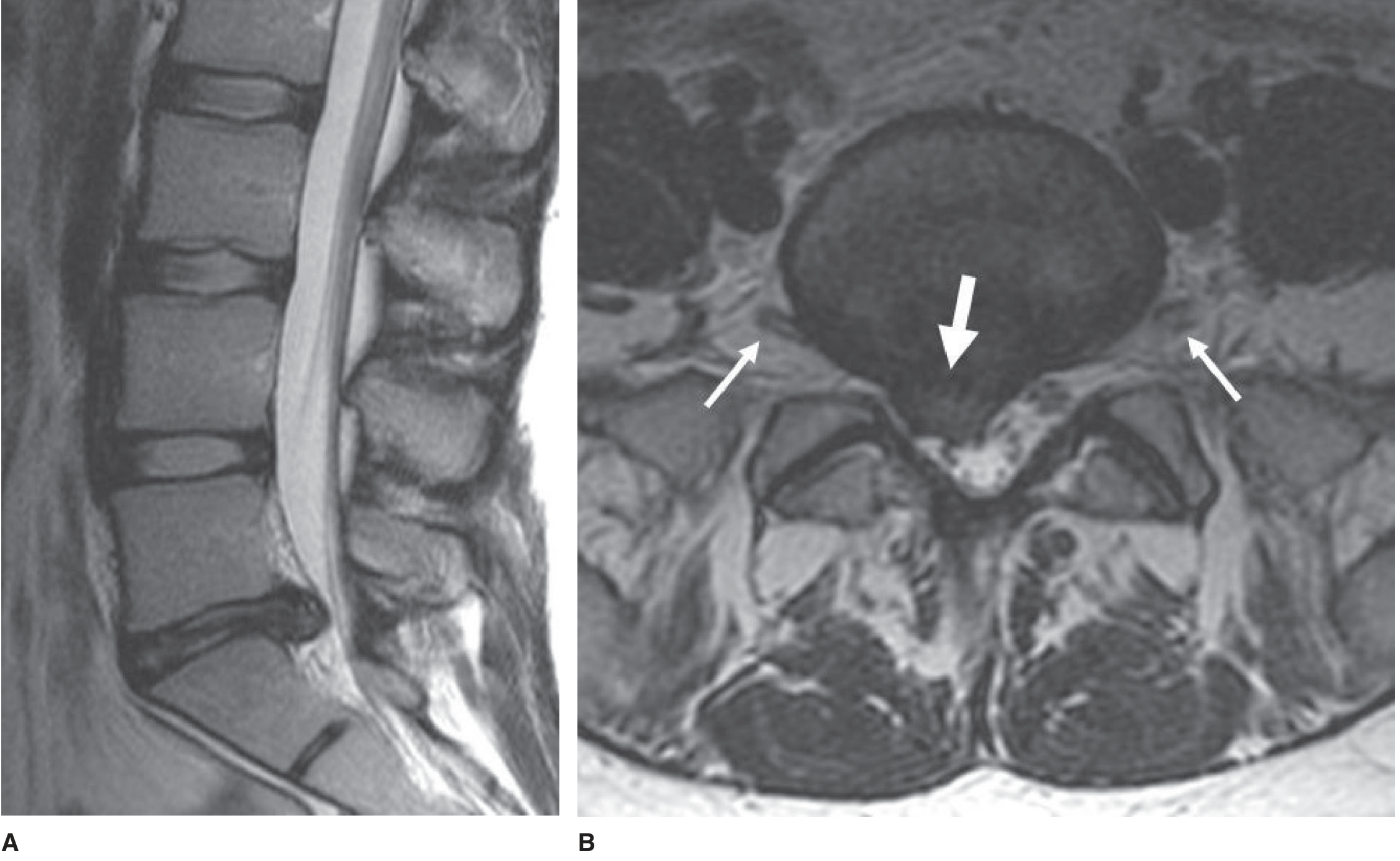
MRI Lumbar Spine
The imaging modality of choice. Provides clear sagittal and axial views of disc-nerve root relationships, defines the thecal sac, identifies herniations, stenosis, epidural collections, and tumors. Not necessary if pain is manageable and surgery is not contemplated.
CT / CT-Myelography
CT is superior for bony detail (fractures, cortical abnormalities). CT-myelography is used when MRI is contraindicated or inconclusive, providing excellent definition of root sleeves.
Plain Radiographs
Low sensitivity for disc disease; useful only to assess alignment, instability (flexion/extension views in spondylolisthesis), or fracture.
EMG / Nerve Conduction Studies
Useful to corroborate subtle clinical findings, differentiate radiculopathy from peripheral neuropathy or plexopathy, and identify the affected root when imaging and clinical findings are discordant.
Indications for urgent advanced imaging (Red Flags):
- History of malignancy or unexplained weight loss
- Fever + localized back pain (epidural abscess, osteomyelitis)
- Immunocompromised state or IV drug use
- Anticoagulant use
- New bladder/bowel dysfunction or saddle anesthesia
- Bilateral motor weakness or Babinski sign
- Post-void residual >100 mL
Rosen's Emergency Medicine, 10th Ed.
Natural History
Spontaneous recovery is the rule in disc herniation-related radiculopathy:
- 36% recover in 2 weeks
- 70% recover in 6 weeks
- 87% recover in 3 months
- 25% have recurrent symptoms within 1 year
Symptom to Diagnosis, 4th Ed.
Treatment
Conservative (First-Line)
- Activity modification - avoid prolonged bed rest; early mobilisation is beneficial
- NSAIDs - first-line analgesia for acute pain
- Short-course oral corticosteroids - may provide short-term pain relief
- Gabapentinoids (gabapentin, pregabalin) - for neuropathic/radicular pain component
- Physical therapy - core stabilisation, McKenzie exercises, traction (limited evidence)
- Analgesics - acetaminophen, weak opioids for refractory pain
A 2024 systematic review of clinical practice guidelines for lumbosacral radiculopathy (Price et al., PM&R, 2024) found heterogeneous recommendations, with NSAIDs and short-course steroids being the most consistently recommended pharmacologic options.
Epidural Steroid Injections (ESI)
Transforaminal or interlaminar ESI can provide short-term pain relief and functional improvement. A 2025 AAN systematic review (Armon et al., Neurology, 2025) found evidence for modest short-term benefit in lumbar radicular pain; however, ESI does not alter the ultimate need for surgery. They are most useful as a bridge to allow rehabilitation or to confirm likely surgical benefit. - Adams and Victor's Principles of Neurology, 12th Ed.
Surgical Indications
Surgery is indicated for:
- Cauda equina syndrome - emergency decompression
- Progressive or severe motor deficit (e.g. foot drop, worsening paraparesis)
- Failure of 6-12 weeks of conservative treatment with ongoing disability
- Intractable pain unresponsive to all conservative measures
Procedure: Lumbar discectomy (microdiscectomy) for disc herniation; laminectomy or laminotomy for spinal stenosis. Patients who obtained substantial leg pain relief from transforaminal ESI but relapsed are often good surgical candidates. - Campbell's Operative Orthopaedics, 15th Ed. 2026
Differential Diagnosis
- Hip osteoarthritis (can mimic upper lumbar radiculopathy)
- Piriformis syndrome - focal mid-buttock pain, sciatic notch tenderness, pain with hip external rotation
- Trochanteric bursitis
- Peripheral neuropathy (bilateral, symmetric)
- Lumbosacral plexopathy
- Vascular claudication (no neurologic deficit, relieved purely by rest, absent pulses)
- Spinal cord tumor or metastases
- Cauda equina tumor
- Tarsal tunnel syndrome (may coexist - reported in ~5% of lumbosacral radiculopathy patients)
Key Points Summary
| Feature | Detail |
|---|---|
| Most common level | L4-L5, L5-S1 (95% of significant herniations) |
| Most specific sign | Crossed SLR |
| Most sensitive sign | Ipsilateral SLR |
| Imaging of choice | MRI lumbar spine |
| Emergency | Cauda equina syndrome (urgent surgery) |
| Natural history | ~87% recover by 3 months with conservative care |
| Surgery threshold | Failure of 6-12 weeks conservative therapy or neurologic emergency |
Sources:
- Adams and Victor's Principles of Neurology, 12th Ed., pp. 222-224
- Symptom to Diagnosis: An Evidence-Based Guide, 4th Ed., p. 141
- Rosen's Emergency Medicine, 10th Ed., pp. 2361-2363
- Bradley and Daroff's Neurology in Clinical Practice
- Campbell's Operative Orthopaedics, 15th Ed. 2026
- Price et al., PM&R 2024 - Medication recommendations systematic review (PMID 38629664)
- Armon et al., Neurology 2025 - AAN epidural steroids systematic review (PMID 39938000)
This is a shared conversation. Sign in to Orris to start your own chat.