Disc Bulge and herniation in 30s pt
Reading File
Finding Sources
Finding Sources
Searching PubMed
"lumbar disc herniation" AND "young adults" AND treatment
Reading File
Reading File
Reading File
Searching PubMed
"lumbar disc herniation" AND conservative treatment
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Here is a comprehensive clinical overview of disc bulge and herniation, with particular relevance to patients in their 30s.
Lumbar Disc Bulge & Herniation in a 30-Year-Old Patient
Terminology - Getting the Definitions Right
These terms are often used loosely, but Campbell's Operative Orthopaedics (2026) provides precise definitions:
| Term | Definition |
|---|---|
| Bulge | Circumferential, symmetric extension of disc beyond the interspace around endplates (>50% of circumference) |
| Protrusion | Focal or asymmetric extension - base against the disc of origin is broader than any other dimension |
| Extrusion | More extreme extension - base narrower than the diameter of extruding material, or no connection remains |
| Sequestration | Disc fragment completely separated from the disc of origin |
A bulge is technically NOT a herniation - it is a morphological descriptor without a specific pathological implication. - Campbell's Operative Orthopaedics 15th Ed, Box 3.1
Epidemiology & Risk Factors in the 30s
Symptomatic lumbar disc herniation affects approximately 2-4% of the population over a lifetime. The peak age of occurrence is 30-50 years, making this a primary concern for patients in their third decade. Risk factors include:
- Family history (strong genetic component)
- Male sex (higher incidence)
- Heavy lifting or twisting
- Physically stressful occupation
- Lower socioeconomic status
- Cigarette smoking
Over 90% of lumbar herniations occur at L4/5 or L5/S1. - Bailey and Love's Short Practice of Surgery, 28th Ed
Pathophysiology
The intervertebral disc consists of a viscoelastic nucleus pulposus surrounded by a dense fibrous annulus fibrosus. With sufficient axial load or repetitive stress, the nucleus pulposus herniates through a tear in the annulus. The displaced material can then impinge on adjacent nerve roots.
- A posterolateral L4/5 disc protrusion affects the L5 nerve root (traversing root)
- A far-lateral (extraforaminal) L5/S1 disc protrusion affects the L5 nerve root (exiting root)
- A central herniation primarily causes back pain but can cause cauda equina syndrome acutely
Clinical Presentation
Typical progression:
- Initial episode of mechanical low back pain
- Development of sciatica - leg pain worse with sitting, better with standing/lying
- Pain/numbness radiating below the knee in a dermatomal distribution
- Motor weakness and bowel/bladder dysfunction are less common but must be assessed
Root compression syndromes by level:
| Disc Level | Root Affected | Weakness | Sensory Loss | Reflex Lost |
|---|---|---|---|---|
| L3/4 | L4 | Knee extension | Medial leg | Patellar (knee jerk) |
| L4/5 | L5 | Foot/great toe dorsiflexion (foot drop) | Lateral leg/dorsum foot | None (or minimal) |
| L5/S1 | S1 | Plantarflexion/toe walking | Lateral foot | Achilles (ankle jerk) |
Physical Examination
Key provocative tests: - Miller's Review of Orthopaedics, 9th Ed
- Straight-leg raise (SLR) - supine: Positive at 30-70° if it reproduces/exaggerates leg symptoms - sensitive for L4, L5, S1 root irritation
- Seated SLR: Less sensitive variation
- Crossed SLR (contralateral): More specific - raising the asymptomatic leg reproduces pain down the symptomatic leg; indicates an axillary (medial) disc herniation
- Lasegue sign: Relief of radiating symptoms with knee flexion while hip is flexed
- Femoral tension sign (prone, knee flexed): Sensitive for L2, L3, L4 root - anterior thigh pain
Red Flags Requiring Urgent/Emergent Evaluation
Immediately refer or image if any of the following are present:
- Acute bowel or bladder dysfunction (urinary retention, incontinence)
- New or progressive leg weakness (including foot drop)
- Saddle anesthesia
- Bilateral symptoms
- Fever, weight loss, night sweats (concern for infection or malignancy)
These may indicate cauda equina syndrome, a surgical emergency. Even a "large disc bulge" in the lumbar spine can obliterate the spinal canal and compress the entire cauda equina. - ROSEN's Emergency Medicine; Sabiston Textbook of Surgery
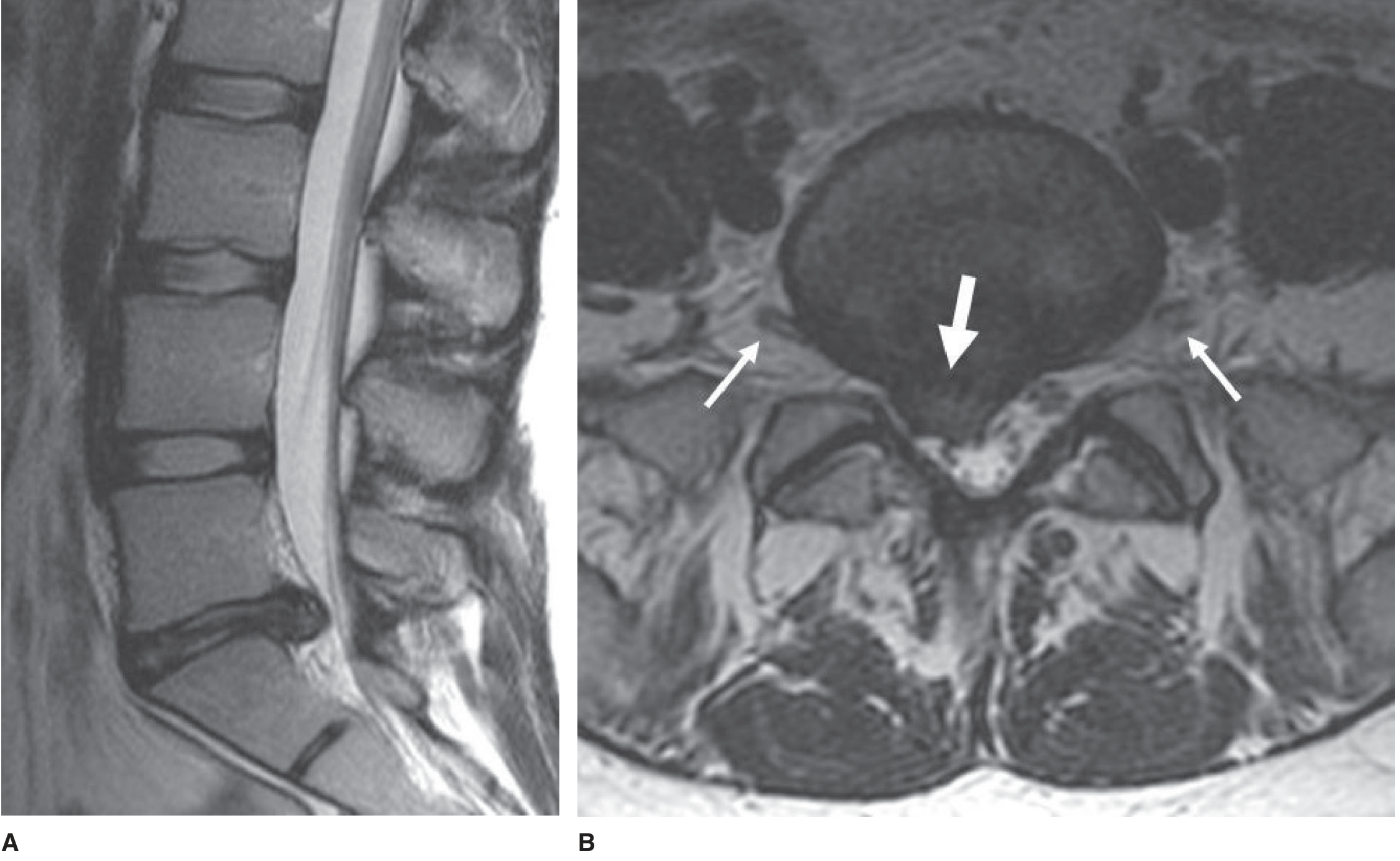
Imaging
MRI is the gold standard - preferred over CT due to sagittal imaging capability and clear disc-to-nerve-root anatomical relationships. Also excludes unsuspected tumor or other etiology.
- MRI is not required if pain is manageable and surgery is not being considered
- Gadolinium-enhanced MRI is best for recurrent disc herniations (distinguishes disc from scar)
- CT myelogram if MRI contraindicated or prior surgery complicates anatomy
- Upright X-rays with flexion-extension views if surgical intervention is being considered (assess instability)
Important caveat: False-positive MRI results are very common in asymptomatic individuals. Clinical correlation is essential. - Miller's Review of Orthopaedics, 9th Ed
Spontaneous Regression - A Key Point for the 30s Patient
This is clinically important and often under-communicated to patients:
Spontaneous regression of lumbar disc herniation is common. Hypothesized mechanisms include:
- Dehydration/shrinkage of disc material
- Retraction back into the disc space
- Resorption via inflammatory/immune response
Factors predicting regression: free fragment extrusions, peripheral contrast enhancement on T1-MRI, high T2 signal herniation, and disc material exposed to the epidural space (rather than subligamentous herniations).
A recent meta-analysis (PMID: 37559207, 2024) confirmed a clinically meaningful incidence of spontaneous resorption - reinforcing a conservative-first approach.
Management
Conservative (First-Line for 6-12 Weeks)
Over 90% of patients with back and leg pain recover within 1-3 months with conservative measures. - Miller's Review of Orthopaedics, 9th Ed
Components:
- Brief relative rest (avoid prolonged bed rest)
- NSAIDs (first-line analgesic)
- Physical therapy - core stabilization, McKenzie exercises, mobilization
- A 2025 systematic review (PMID: 40128486) confirms exercise is effective for lumbar disc herniation
- Pregabalin (GABA analogue) - useful for neuropathic/radicular pain
- Transforaminal epidural steroid injections - can reduce radicular inflammation and pain, helpful as an adjunct
- IV dexamethasone (6-10 mg single dose) or oral prednisone taper may benefit patients with acute radiculopathy in the ED setting
Surgical Indications
Surgery is indicated when:
- Conservative treatment fails after 6-12 weeks of persistent, disabling pain
- Progressive motor weakness (e.g., foot drop that is not improving)
- Cauda equina syndrome (emergency)
Standard surgical procedure: Microdiscectomy (hemilaminectomy with disc fragment excision)
- 85-90% success rate for sciatic pain from L4/5 or L5/S1 herniations
- Patients typically home the next day and resume activities within weeks
- Complication rate (CSF leak, infection): ~1-2%
- Rerupture rate: <5%
- Fusion is reserved for significant spondylolisthesis or instability
Evidence note: The SPORT trial and Dutch randomized trial both showed that early surgery provides faster pain relief and faster functional return compared to conservative care, but at 1 year, outcomes are similar between surgical and conservative groups. For patients with persistent sciatica >4-12 months, surgery showed better outcomes at 6 and 12 months follow-up. - Adams and Victor's Principles of Neurology, 12th Ed
A 2024 network meta-analysis (PMID: 38506677) comparing minimally invasive techniques vs. open discectomy found comparable outcomes, supporting use of the least invasive approach available.
Age-Specific Considerations in the 30s
- Younger age is a predictive factor for better surgical outcomes
- The disc at this age still has significant hydration and healing potential - spontaneous regression is more likely than in older patients
- A clear precipitating event (lifting injury, trauma) and radicular leg pain both predict good surgical outcomes
- Foot drop - if not improving over 1-2 weeks, most experts recommend early referral for surgery, though evidence is limited on whether delay causes permanent deficit
- Long-term recurrence risk: even after surgery, rerupture at the same or adjacent level is a consideration - core strengthening and ergonomic modification are important for prevention
Sources:
- Bailey and Love's Short Practice of Surgery, 28th Ed
- Campbell's Operative Orthopaedics, 15th Ed (2026)
- Adams and Victor's Principles of Neurology, 12th Ed
- Miller's Review of Orthopaedics, 9th Ed
- Grainger & Allison's Diagnostic Radiology
- ROSEN's Emergency Medicine
- Sabiston Textbook of Surgery
- PMID: 37559207 (Spontaneous resorption meta-analysis, 2024)
- PMID: 40128486 (Exercise for LDH systematic review, 2025)
- PMID: 38506677 (MIS vs. open discectomy network meta-analysis, 2024)
This is a shared conversation. Sign in to Orris to start your own chat.