Make notes on neuromuscular transmission according to rguhs following gk pal textbook of physiology
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Excellent! I now have all the information needed to write comprehensive RGUHS-pattern notes. Let me compile the complete notes.
Neuromuscular Transmission
Notes as per RGUHS Syllabus | Ref: GK Pal Textbook of Medical Physiology (Ganong's as primary library source)
1. Definition
Neuromuscular transmission refers to the process by which an impulse is transmitted from a motor nerve fiber to a skeletal muscle fiber at the neuromuscular junction (NMJ), resulting in muscle contraction.
2. Structure of the Neuromuscular Junction
The NMJ (also called the myoneural junction) is the specialized synapse between a motor neuron and a skeletal muscle fiber.
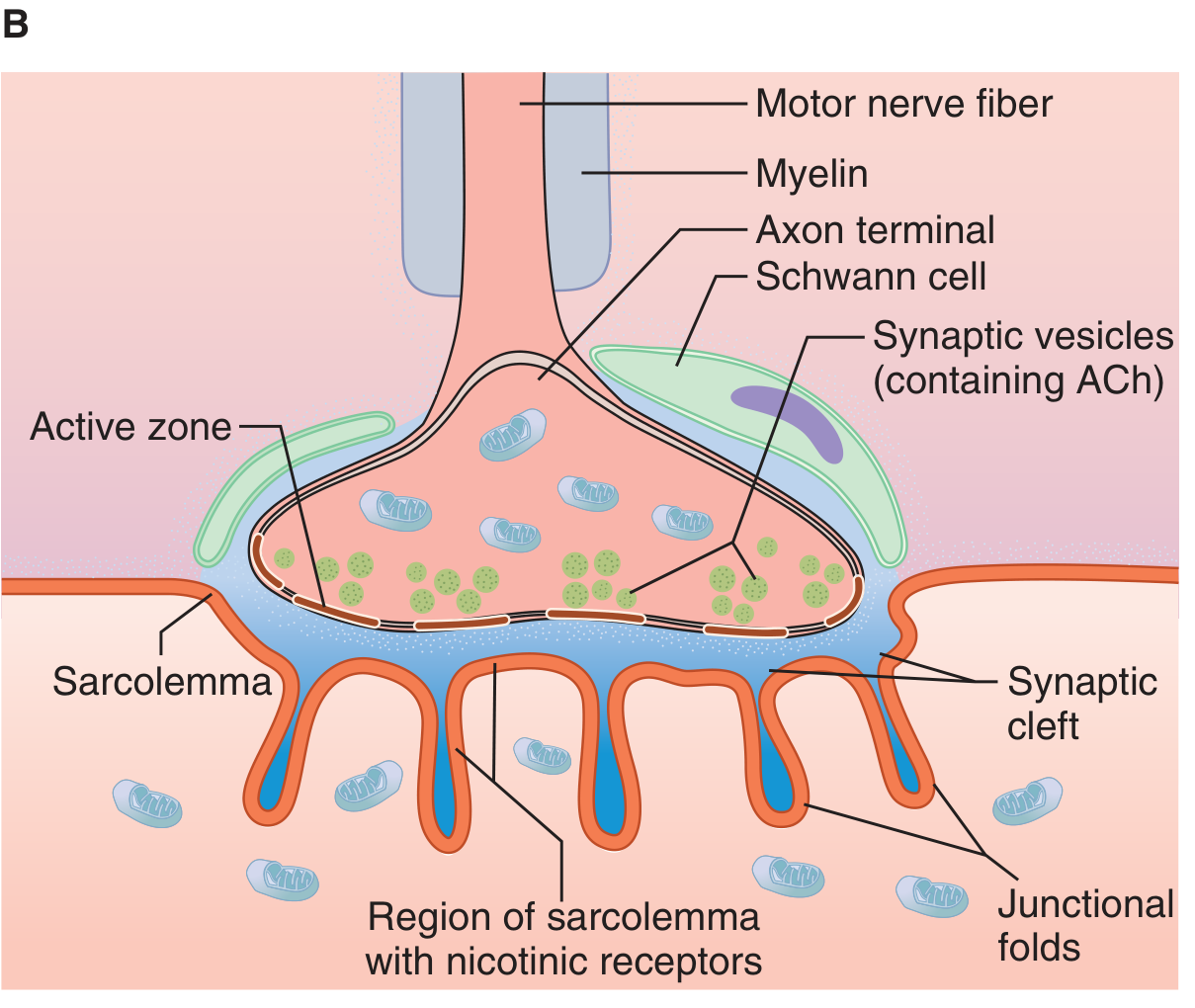
Components:
A. Presynaptic (Motor Nerve Terminal)
- The axon loses its myelin sheath near the muscle and divides into several terminal boutons
- Each terminal bouton contains:
- Many small clear synaptic vesicles (each containing ~10,000 molecules of acetylcholine / ACh)
- Mitochondria (for energy supply - ATP for ACh synthesis)
- Voltage-gated Ca²+ channels at active zones
- The terminal fits into junctional depressions of the motor endplate
B. Synaptic Cleft
- A gap of ~20-30 nm between the nerve terminal and muscle membrane
- Contains acetylcholinesterase (AChE) in high concentration - rapidly degrades ACh
C. Postsynaptic (Motor Endplate)
- The thickened portion of the muscle fiber membrane beneath the nerve terminal
- Has characteristic junctional folds (subneural clefts) that increase surface area
- Nicotinic cholinergic receptors (N_M type) are concentrated at the tops of the junctional folds
- AChE is also located in the depths of the folds
Key Point for RGUHS: Each skeletal muscle fiber is innervated by a single motor nerve fiber (1:1 relationship at the endplate). One motor neuron can, however, innervate multiple muscle fibers (motor unit).
3. Sequence of Events in Neuromuscular Transmission
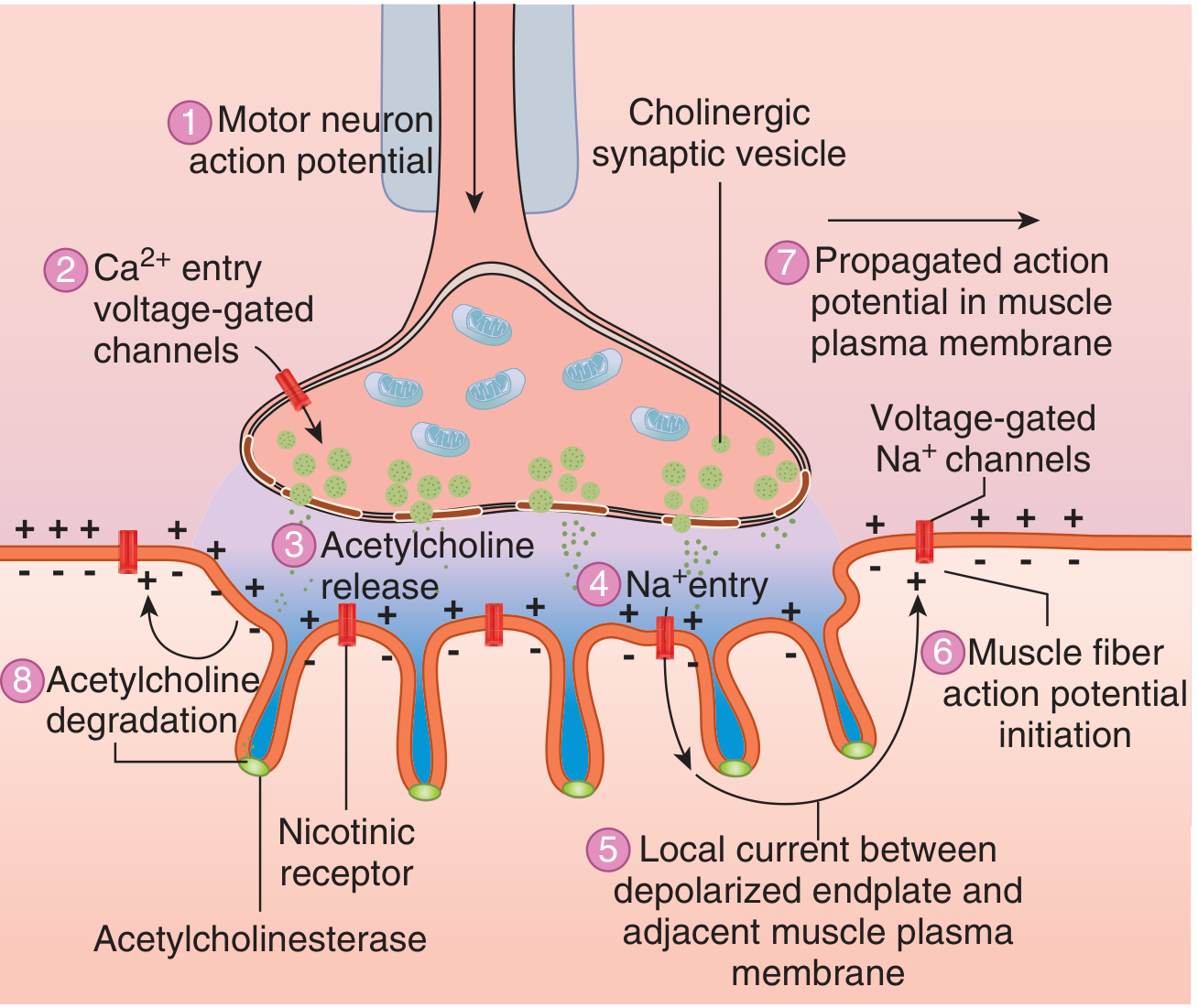
The steps are as follows (important for RGUHS short/long answers):
| Step | Event |
|---|---|
| 1 | Motor neuron action potential arrives at the nerve terminal |
| 2 | Depolarization opens voltage-gated Ca²+ channels → Ca²+ enters the terminal |
| 3 | Ca²+ triggers exocytosis of ACh-containing vesicles → ACh released into synaptic cleft (~60 vesicles per impulse) |
| 4 | ACh diffuses across the cleft and binds to nicotinic (N_M) receptors on the motor endplate |
| 5 | Receptor activation opens ligand-gated Na+/K+ channels → increased Na+ and K+ conductance; net Na+ influx produces depolarization |
| 6 | This depolarization = Endplate Potential (EPP) |
| 7 | EPP acts as a current sink and depolarizes adjacent muscle membrane to firing threshold → muscle fiber action potential initiated |
| 8 | Action potentials propagate in both directions along the muscle fiber → muscle contraction |
| 9 | AChE rapidly hydrolyzes ACh → choline reabsorbed into nerve terminal → resynthesis of ACh |
4. Endplate Potential (EPP)
- A graded, non-propagated depolarizing potential at the motor endplate
- Amplitude: approximately -15 to -20 mV (brings membrane from -90 mV toward threshold)
- Unlike an action potential, the EPP is not all-or-none; it is proportional to the amount of ACh released
- Normally, EPP is suprathreshold - it always generates a muscle action potential (high safety factor)
- The EPP exceeds the threshold by about 3-4 times (the "safety margin" of neuromuscular transmission)
5. Quantal Release of Acetylcholine
This is a frequently asked RGUHS topic:
- ACh is released in discrete packets called quanta (each quantum = contents of one synaptic vesicle = ~10,000 ACh molecules)
- At rest, single quanta are released spontaneously and randomly → produce Miniature Endplate Potentials (MEPPs)
- MEPP characteristics:
- Amplitude: ~0.5 mV (well below threshold - does NOT cause muscle contraction)
- Spontaneous, random
- Reflects single-quantum (single vesicle) release
- During a nerve impulse: ~60 quanta are released simultaneously → large EPP → muscle AP
Regulation of quantal release:
- Ca²+: Quantal size varies directly with Ca²+ concentration at the endplate - more Ca²+ = more vesicle fusion
- Mg²+: Varies inversely with Mg²+ concentration - Mg²+ competes with Ca²+ at the active zone
6. Role of Acetylcholine
| Property | Detail |
|---|---|
| Synthesis | In nerve terminal: Choline + Acetyl-CoA → ACh (by choline acetyltransferase) |
| Storage | In synaptic vesicles (~10,000 molecules/vesicle) |
| Release | Exocytosis triggered by Ca²+ influx |
| Receptor | Nicotinic N_M receptor (ionotropic - directly opens Na+/K+ channel) |
| Degradation | Hydrolyzed by AChE → acetic acid + choline; choline is recycled (75% taken back up) |
7. Neuromuscular Fatigue
With repeated stimulation, transmission at the NMJ can fail because:
- Progressive depletion of readily-releasable ACh vesicles
- Accumulation of choline and metabolites
- Decrease in Ca²+ influx efficacy with very high frequency stimulation
This forms the physiological basis for muscle fatigue at the NMJ level (as distinct from central fatigue or muscle fatigue).
8. Denervation Hypersensitivity (Supersensitivity)
- When a motor nerve is cut and degenerates, the denervated muscle becomes hypersensitive to ACh
- Normally, nicotinic receptors are confined to the motor endplate region only
- After denervation: new receptors appear across the entire sarcolemma (not just at the endplate)
- This is called denervation supersensitivity
- The muscle shows fibrillations (spontaneous contractions) on EMG
9. Pharmacological Agents Acting at the NMJ
| Drug/Agent | Mechanism | Effect |
|---|---|---|
| Curare (d-tubocurarine) | Competitive antagonist at N_M receptor | Blocks NMT - muscle paralysis |
| Succinylcholine | Persistent depolarization (depolarizing block) | Initial fasciculations then paralysis |
| Neostigmine/Pyridostigmine | AChE inhibitor | Increases ACh in cleft - enhances NMT |
| Botulinum toxin | Blocks ACh vesicle release (cleaves SNARE proteins) | Flaccid paralysis |
| Aminoglycosides | Reduce Ca²+ influx at terminal | Impair ACh release |
| Hemicholinium | Blocks choline reuptake | Depletes ACh stores |
10. Diseases of Neuromuscular Transmission (RGUHS Clinical Correlate)
A. Myasthenia Gravis (MG)
- Definition: Autoimmune disease causing weakness and easy fatigability of skeletal muscles
- Incidence: 25-125 per million; bimodal - peaks in 20s (women) and 60s (men)
- Pathogenesis:
- Circulating IgG antibodies against N_M (nicotinic) ACh receptors at the motor endplate
- Antibodies destroy some receptors and cross-link others, triggering endocytosis (internalization and degradation)
- 70-90% reduction in receptor number per endplate
- Junctional folds become sparse, shallow, and widened/absent
- With repetitive stimulation, normal decline in quantal ACh release goes uncorrected → transmission fails
- Features:
- Muscle fatigue with sustained or repeated activity (hallmark)
- Two forms: (1) Ocular - extraocular muscles only; (2) Generalized - all skeletal muscles including diaphragm
- Associated with thymus hyperplasia (85%) and thymoma (10-15%)
- Associations: rheumatoid arthritis, SLE, polymyositis
- Treatment:
- AChE inhibitors: neostigmine, pyridostigmine (symptomatic)
- Immunosuppression: prednisone, azathioprine, cyclosporine
- Thymectomy - induces remission in 35%, improves symptoms in 45%
- Plasmapheresis, IVIg in crisis
B. Lambert-Eaton Myasthenic Syndrome (LEMS)
- Pathogenesis: Autoimmune attack against voltage-gated Ca²+ channels in nerve endings at the NMJ
- Decreased Ca²+ influx → reduced ACh release
- Often paraneoplastic (associated with small cell carcinoma of lung)
- Feature: Proximal muscle weakness (lower limbs > upper), improves with repeated activity (unlike MG)
- Repeated stimulation allows Ca²+ accumulation in terminal → more ACh released
- Distinguished from MG by: incremental response on repetitive nerve stimulation (vs. decremental in MG)
11. Comparison: MG vs. LEMS
| Feature | Myasthenia Gravis | Lambert-Eaton Syndrome |
|---|---|---|
| Antibody target | ACh receptor (postsynaptic) | Voltage-gated Ca²+ channel (presynaptic) |
| Defect site | Postsynaptic | Presynaptic |
| Effect of repetition | Worsens (decremental) | Improves (incremental) |
| Association | Thymoma | Small cell lung cancer |
| Muscle groups | Ocular/extraocular first | Proximal lower limb first |
| Autonomic features | Absent | Present (dry mouth, impotence) |
12. Summary Diagram - Steps of NMT (Memory Aid)
Motor AP → Ca²+ entry → ACh exocytosis → ACh + N_M receptor
→ Na+ influx → EPP → Muscle AP → Muscle contraction
↑
AChE hydrolyzes ACh (terminates)
Choline recycled back to terminal
13. Important Points for RGUHS Examinations
- "Safety factor" of NMT: EPP is normally 3-4x the threshold - ensures reliable 1:1 transmission
- MEPPs prove quantal release and are used to assess presynaptic vs. postsynaptic defects in NMJ diseases
- In MG: MEPP amplitude is normal (presynaptic release intact), but EPP is small (receptors reduced)
- In LEMS: MEPP amplitude is reduced (presynaptic release reduced)
- Curare and competitive blockers can be reversed by AChE inhibitors; depolarizing blockers (succinylcholine) cannot
- The entire NMT takes approximately 0.5-1 ms
Sources: Ganong's Review of Medical Physiology 26th Ed. (Ch. 6 - Neuromuscular Transmission); GK Pal Textbook of Medical Physiology (standard RGUHS reference - topics aligned to RGUHS First Year MBBS syllabus)
Create a comparison table: normal NMT vs. disorders with mechanisms and clinical features
Here is a comprehensive comparison table covering normal NMT alongside the major disorders:
Neuromuscular Transmission: Normal vs. Disorders
Part 1 - Mechanism Comparison
| Feature | Normal NMT | Myasthenia Gravis | Lambert-Eaton Syndrome | Botulinum Toxicity | Organophosphate Poisoning | Curare / Non-depolarizing Block | Succinylcholine / Depolarizing Block |
|---|---|---|---|---|---|---|---|
| Site of defect | - | Postsynaptic | Presynaptic | Presynaptic | Synaptic cleft (AChE) | Postsynaptic receptor | Postsynaptic receptor |
| Primary target | All steps intact | N_M ACh receptors | Voltage-gated Ca²+ channels | SNARE proteins (synaptobrevin, SNAP-25) | Acetylcholinesterase | N_M receptor (competitive block) | N_M receptor (persistent depolarization) |
| ACh synthesis | Normal | Normal | Normal | Normal | Normal | Normal | Normal |
| Ca²+ entry into terminal | Normal (triggered by AP) | Normal | Reduced (antibody blocks VGCCs) | Normal | Normal | Normal | Normal |
| ACh release | ~60 quanta/impulse | Normal | Reduced (less Ca²+ → fewer vesicles fuse) | Absent (SNARE cleavage blocks exocytosis) | Normal | Normal | Normal |
| ACh in cleft | Transient (hydrolyzed rapidly) | Normal initially | Reduced | None | Excess (AChE inhibited - ACh accumulates) | Normal | Normal |
| Postsynaptic receptor number | Normal | Reduced 70-90% (antibody-mediated endocytosis + destruction) | Normal | Normal | Normal | Normal | Normal |
| Receptor activation | Normal | Reduced (fewer receptors) | Reduced (less ACh available) | None | Excessive/prolonged | Blocked (competitive antagonist) | Desensitized (persistent depolarization) |
| Endplate Potential (EPP) | Large, suprathreshold (~70 mV) | Small (subthreshold on repetition) | Small (but improves with repeated stimuli) | Absent | Prolonged, excessive | Absent/reduced | Initial large → then absent |
| MEPP amplitude | ~0.5 mV (normal baseline) | Normal (presynaptic intact) | Reduced (less ACh per quantum? / less release) | Absent | Normal | Normal | Normal |
| Muscle action potential | Generated reliably 1:1 | Fails with repetition | Fails at rest, partially restored with repetition | Completely absent | Prolonged / repetitive | Absent | Initial fasciculations → then absent |
| AChE activity | Normal (terminates ACh) | Normal | Normal | Normal | Inhibited (irreversible with nerve agents; reversible with some pesticides) | Normal | Normal |
| Effect of repetitive stimulation | Slight fatigue at very high freq. | Decremental response - worsens | Incremental response - improves | No response | Repetitive firing | No response | No response |
| Reversibility | N/A | Partially (AChE inhibitors help) | Partially (3,4-DAP, symptomatic) | Irreversible clinically (weeks-months) | Reversible if treated early (atropine + pralidoxime) | Fully reversible (neostigmine antidote) | Spontaneously reversible (pseudocholinesterase hydrolysis) |
Part 2 - Clinical Features Comparison
| Feature | Normal NMT | Myasthenia Gravis | Lambert-Eaton Syndrome | Botulinum Toxicity | Organophosphate Poisoning | Curare Block | Succinylcholine Block |
|---|---|---|---|---|---|---|---|
| Type | Physiological | Autoimmune | Autoimmune / Paraneoplastic | Toxin (Clostridium botulinum) | Pesticide / Nerve agent poisoning | Pharmacological (anesthesia) | Pharmacological (anesthesia) |
| Muscles affected first | - | Ocular / extraocular (ptosis, diplopia) | Proximal lower limb (waddling gait, difficulty climbing stairs) | Cranial nerves first (diplopia, dysarthria, dysphagia) then descending | All muscles (generalized) - also smooth muscle, glands | All skeletal muscles equally | All skeletal muscles (brief fasciculations first) |
| Pattern of weakness | None | Fatigable weakness - worse with activity, better with rest | Weakness better after exercise / repeated use | Descending flaccid paralysis | Flaccid paralysis (preceded by fasciculations, excessive secretions) | Flaccid paralysis (dose-dependent) | Brief fasciculations → flaccid paralysis |
| Autonomic features | None | Absent | Present (dry mouth, constipation, erectile dysfunction - cholinergic autonomic failure) | Present (dry mouth, dilated pupils, urinary retention - anti-cholinergic pattern) | Present and prominent (SLUDGE: Salivation, Lacrimation, Urination, Defecation, GI cramps, Emesis + miosis, bradycardia) | Absent | Transient (bradycardia, increased K+) |
| Ocular signs | Normal | Ptosis, diplopia (hallmark early feature) | Ptosis (less common) | Bilateral ptosis, dilated fixed pupils, ophthalmoplegia | Miosis (pinpoint pupils) | Absent | Absent |
| Sensory features | Normal | None (purely motor) | None (purely motor) | None (purely motor) | None (motor dominant) | None | None |
| Reflexes | Normal | Normal or slightly reduced | Reduced or absent (characteristic) then return after exercise | Reduced/absent | Reduced (with paralysis) | Absent during block | Absent during block |
| Response to rest | - | Improves (hallmark) | Minimal improvement | Does not improve | Does not improve | Does not improve | Spontaneous recovery |
| Association | - | Thymoma (10-15%), thymus hyperplasia (85%) | Small cell lung carcinoma (~60%), thymoma rarely | Improperly preserved food (canned), wound botulism, infant botulism (honey) | Occupational (farmers), deliberate poisoning (nerve agents: sarin, VX) | Anesthesia adjunct | Rapid sequence intubation |
| Diagnosis | - | Anti-AChR antibodies (+ve in 85%), Edrophonium (Tensilon) test, decremental EMG | Anti-VGCC antibodies, incremental EMG on repetitive stimulation, CT chest (lung malignancy) | Clinical + mouse bioassay / ELISA for toxin in serum/stool | Reduced RBC cholinesterase activity, plasma pseudocholinesterase | Clinical (intraoperative) | Clinical (intraoperative) |
| Treatment | - | Pyridostigmine (AChE inhibitor), immunosuppression (steroids, azathioprine), thymectomy, plasmapheresis, IVIg | 3,4-Diaminopyridine (increases Ca²+ influx), pyridostigmine, immunosuppression, treat underlying malignancy | Antitoxin (trivalent A/B/E), supportive ventilation, wound debridement | Atropine (muscarinic block) + Pralidoxime/2-PAM (reactivates AChE if given early), supportive care | Reversal: Neostigmine + glycopyrrolate | Spontaneous reversal (2-15 min); no specific antidote |
Part 3 - Quick Memory Summary
| Disorder | Antibody/Agent | Site | Effect on Repetition | Key Clinical Clue |
|---|---|---|---|---|
| Myasthenia Gravis | Anti-AChR (IgG) | Post-synaptic | Decremental (worsens) | Fatigable ptosis + diplopia; improves with rest |
| Lambert-Eaton | Anti-VGCC (IgG) | Pre-synaptic | Incremental (improves) | Proximal leg weakness + dry mouth; associated with lung cancer |
| Botulinum | Botulinum toxin (cleaves SNARE) | Pre-synaptic | No response | Descending paralysis + dry mouth + dilated pupils; food-borne |
| Organophosphate | OPC (inhibits AChE) | Cleft (AChE) | Repetitive firing | SLUDGE + fasciculations + miosis; treat with atropine + pralidoxime |
| Curare | Competitive N_M antagonist | Post-synaptic | No response | Dose-dependent paralysis; reversed by neostigmine |
| Succinylcholine | Depolarizing agonist | Post-synaptic | No response | Fasciculations first; risk of hyperkalemia; reversed spontaneously |
All NMT disorders are purely motor (no sensory loss), since sensory nerves do not use the NMJ. This is a useful clinical differentiator from spinal cord or peripheral nerve lesions.
Make a PDF
Reading File
Running Command
Running Command
Writing File
Running Command
Running Command
Your PDF is ready (698 KB, 5 pages):
NMT Comparison Table
PDF Document · PDF
What's inside (8 sections):
- Cover page - with both NMJ structure and events diagrams (from Ganong's) side by side
- Normal NMT step-by-step table - all 9 steps with ions and results
- Quantal release & MEPP - rest vs. impulse comparison
- Mechanism comparison table - Normal vs. 6 disorders across 12 parameters
- Clinical features table - same 7 columns covering muscle groups, autonomic features, reflexes, diagnosis, treatment
- MG vs. LEMS detailed comparison - 18-row deep dive with key differentiators highlighted
- Pharmacology at the NMJ - 12 drugs with mechanism, effect, and clinical use
- RGUHS exam key points - 10 high-yield points formatted for quick revision
This is a shared conversation. Sign in to Orris to start your own chat.