Give me notes of Diabetes mellitus in easy language Both type 1 and type 2
🩺 Diabetes Mellitus - Easy Language Notes
What is Diabetes?
How is Diabetes Diagnosed?
| Test | Cut-off |
|---|---|
| Random blood glucose (with symptoms) | > 200 mg/dL |
| Fasting blood glucose (8-hour fast) | > 126 mg/dL |
| HbA1c (3-month average) | > 6.5% |
| 2-hour glucose after 75g oral glucose tolerance test | > 200 mg/dL |
TYPE 1 DIABETES MELLITUS
Simple Explanation
Key Facts
- Accounts for 5-10% of all diabetes cases
- Can occur at any age - not just children (up to 40% develop it after age 30)
- Absolute insulin deficiency - the pancreas makes no insulin at all
- Strong link with other autoimmune diseases: Graves' disease, Hashimoto's thyroiditis, vitiligo, celiac disease, pernicious anemia
Cause / Pathogenesis (What Goes Wrong?)
- Genetics: The major risk gene (40-50%) involves HLA class II genes (HLA-DR and HLA-DQ). If both parents have Type 1 DM, risk increases 6-fold. However, more than 75% of new Type 1 DM patients have NO family member with the condition.
- Trigger: Something (likely a virus - enterovirus) triggers the immune system to attack beta cells.
- Beta cell destruction: Immune cells infiltrate the pancreas and release inflammatory substances (TNF-alpha, interferon-gamma, interleukin-1) that kill beta cells. This happens over months to years.
- Stages:
- Stage 1: Autoantibodies present + normal blood sugar
- Stage 2: Autoantibodies present + blood sugar starting to rise
- Stage 3: Autoantibodies present + high blood sugar (symptomatic = you actually have clinical diabetes)
Classic Symptoms (Usually Appear Over Weeks)
- Polyuria - peeing a lot (sugar spills into urine, pulling water with it)
- Polydipsia - extreme thirst (losing so much water)
- Polyphagia - always hungry (cells are starving even though blood sugar is high)
- Weight loss - sudden, significant (body starts breaking fat and muscle)
- Fatigue
Dangerous Emergency: DKA (Diabetic Ketoacidosis)
- Nausea/vomiting
- Abdominal pain
- Fruity breath (smell of acetone)
- Rapid breathing (Kussmaul breathing)
- Can lead to coma if untreated
Treatment
- Insulin is mandatory - these patients MUST take insulin to survive. The pancreas produces none.
- Goal: Keep fasting glucose 80-130 mg/dL; postprandial glucose < 180 mg/dL
- Use of continuous glucose monitors (CGM) is now standard to track levels around the clock
- Lifestyle: healthy diet, regular exercise
TYPE 2 DIABETES MELLITUS
Simple Explanation
Key Facts
- Accounts for >90% of all diabetes cases
- Usually affects adults, though increasingly seen in younger people due to obesity
- Relative insulin deficiency - some insulin is made, but not enough
- Develops gradually over years, often with a prediabetes stage first
- NOT prone to DKA, but can develop HHS (Hyperglycemic Hyperosmolar State) during illness - very high blood sugar, severe dehydration
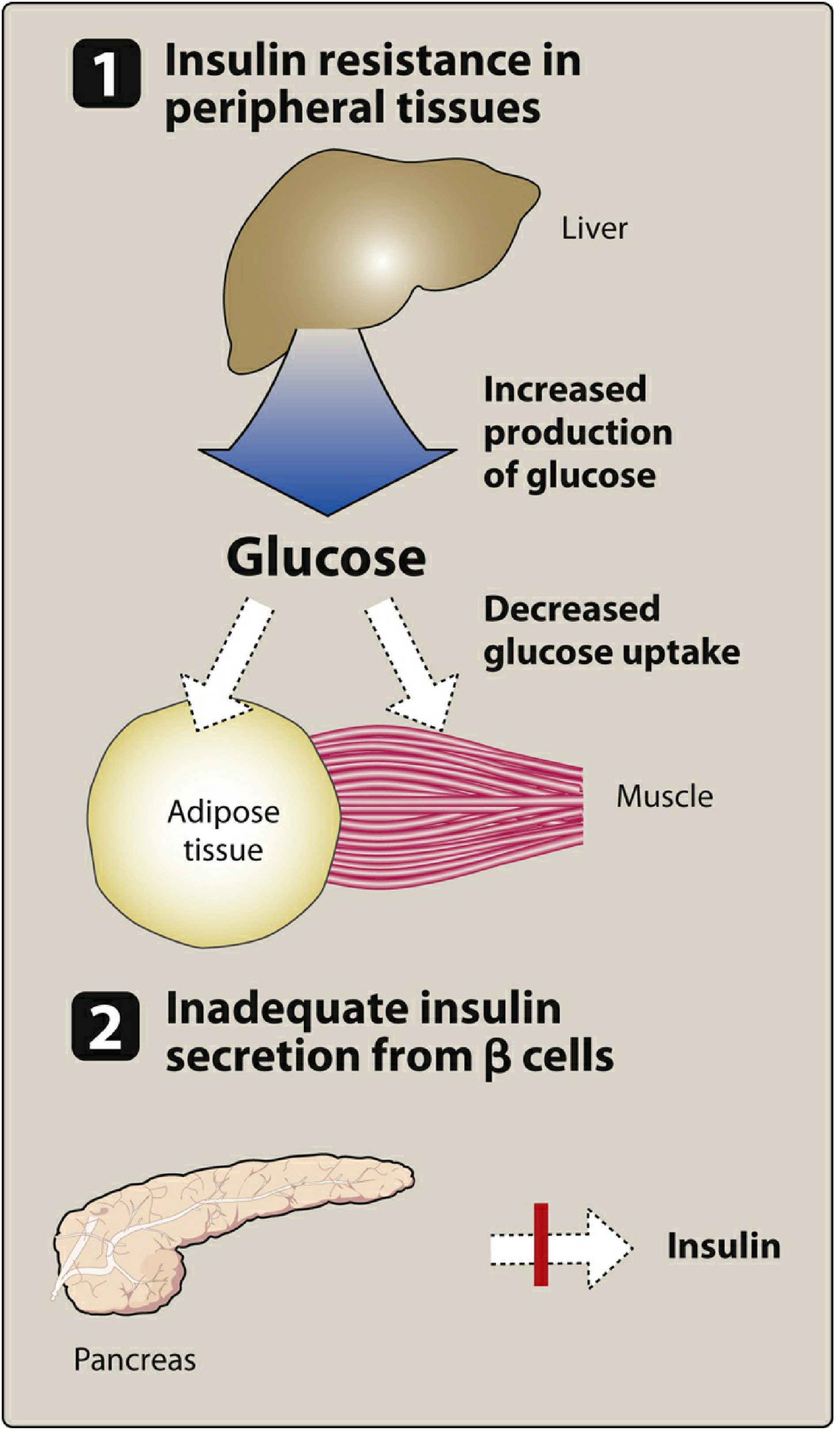
Cause / Pathogenesis (What Goes Wrong?)
- Liver keeps producing glucose even when it shouldn't
- Muscles and fat tissue don't absorb glucose properly
- Obesity is the biggest driver - approximately 80% of Type 2 diabetics are overweight or obese
- Beta cells sense glucose poorly and secrete insulin too slowly or in insufficient amounts
- Over time, beta cell mass may shrink
- Elevated glucagon levels worsen high blood sugar (glucagon normally raises blood sugar, and it's not properly suppressed)
Symptoms
- Frequent urination, excessive thirst
- Blurred vision
- Slow-healing wounds
- Frequent infections (skin, urine, gum)
- Fatigue
- Tingling/numbness in hands or feet (from early nerve damage)
Who Is at Risk?
- Overweight or obese
- Age > 45 years
- Physical inactivity
- Family history of diabetes
- High blood pressure / abnormal cholesterol
- History of gestational diabetes
- Polycystic ovary syndrome (PCOS)
- Ethnicity (South Asian, Hispanic, Black populations have higher risk)
Treatment
-
Lifestyle first - weight loss, exercise, healthy diet. These alone can normalize blood sugar in early cases. Exercise and weight loss directly reduce insulin resistance.
-
Oral medications (when lifestyle isn't enough):
- Metformin - first choice; reduces liver glucose production
- Sulfonylureas - stimulate beta cells to release more insulin
- SGLT2 inhibitors (e.g., empagliflozin) - remove excess glucose through urine; also protect the heart and kidneys
- GLP-1 agonists (e.g., semaglutide) - injectable; stimulate insulin, suppress appetite, cause weight loss
- DPP-4 inhibitors, thiazolidinediones, others
-
Insulin - added as the disease progresses and beta cells fail further
COMPARISON TABLE: TYPE 1 vs TYPE 2
| Feature | Type 1 | Type 2 |
|---|---|---|
| % of diabetes cases | 5-10% | >90% |
| Usual age of onset | Any age (often young) | Usually adult (rising in younger) |
| Cause | Autoimmune destruction of beta cells | Insulin resistance + beta cell failure |
| Body weight | Usually normal/thin | Usually overweight/obese |
| Insulin production | None (absolute deficiency) | Some (relative deficiency) |
| Autoantibodies | Present (anti-islet, anti-insulin) | Absent |
| Genetic link | HLA-DR/DQ genes | Polygenic + lifestyle |
| Dangerous emergency | DKA | HHS |
| Treatment | Insulin MUST be given | Lifestyle + oral drugs, insulin later |
| Onset of symptoms | Acute (weeks) | Gradual (years, often asymptomatic) |
CHRONIC COMPLICATIONS (Both Types)
Microvascular Complications (Small blood vessel damage - specific to diabetes)
| Complication | What it affects | Result |
|---|---|---|
| Diabetic Retinopathy | Eyes | Leading cause of blindness in adults |
| Diabetic Nephropathy | Kidneys | Leading cause of kidney failure/dialysis |
| Diabetic Neuropathy | Nerves | Tingling, pain, numbness, foot ulcers, amputations |
Macrovascular Complications (Large blood vessel damage - atherosclerosis)
- Heart attack (MI) - most common cause of death in diabetics
- Stroke
- Peripheral artery disease (poor circulation in limbs)
Key fact: Tight glucose control (HbA1c < 7%) reduces the risk of retinopathy progression by 76% (DCCT trial). In the US, diabetes is the #1 cause of blindness in adults, #1 cause of kidney failure requiring dialysis, and most common cause of non-traumatic lower limb amputation.
QUICK MEMORY TRICKS
- Polyuria (lots of pee)
- Polydipsia (lots of thirst)
- Polyphagia (lots of hunger)
-
- Unexplained weight loss
- Small: Retino, Nephro, Neuro-pathy
- Big: Heart attack, Stroke, Peripheral vascular disease
Give pathophysiology in flow chart form
A clean medical flowchart showing the pathophysiology of Type 1 and Type 2 Diabetes Mellitus side by side on a white background. LEFT SIDE - TYPE 1 DIABETES: Box 1: "Genetic Susceptibility (HLA-DR/DQ genes)" → Arrow down → Box 2: "Environmental Trigger (Virus / Unknown)" → Arrow down → Box 3: "Autoimmune Response — T cells & antibodies attack beta cells" → Arrow down → Box 4: "Beta Cell Destruction (Insulitis)" → Arrow down → Box 5: "ABSOLUTE Insulin Deficiency (Zero insulin)" → Arrow down → Box 6: "Cells cannot take up glucose" → Two arrows: one going right to "Hyperglycemia (High blood sugar)" and one going down to "Body burns fat → Ketone bodies" → Arrow from ketones down to Red box: "DIABETIC KETOACIDOSIS (DKA) — Medical Emergency" RIGHT SIDE - TYPE 2 DIABETES: Box 1: "Genetic Predisposition + Obesity + Sedentary lifestyle" → Arrow down → Box 2: "Insulin Resistance — Liver, Muscle, Adipose tissue cells IGNORE insulin" → Arrow down with parallel box: "Liver keeps producing glucose (not suppressed)" → Arrow down → Box 3: "Pancreas compensates — secretes MORE insulin" → Arrow down → Box 4: "Beta cell exhaustion over years — secretion gradually falls" → Arrow down → Box 5: "RELATIVE Insulin Deficiency" → Arrow down → Box 6: "Hyperglycemia (High blood sugar)" → Arrow down to Orange box: "Hyperosmolar Hyperglycemic State (HHS) — if severe" Both sides converge at bottom to shared box: "CHRONIC HYPERGLYCEMIA" → Three branches labeled: (1) Microvascular — Retinopathy, Nephropathy, Neuropathy | (2) Macrovascular — Heart attack, Stroke, PVD | (3) Other — Poor wound healing, Infections Use color coding: Blue for Type 1 pathway, Green for Type 2 pathway, Red for DKA, Orange for HHS, Purple for shared complications. Clean arrows, readable fonts, medical diagram style.
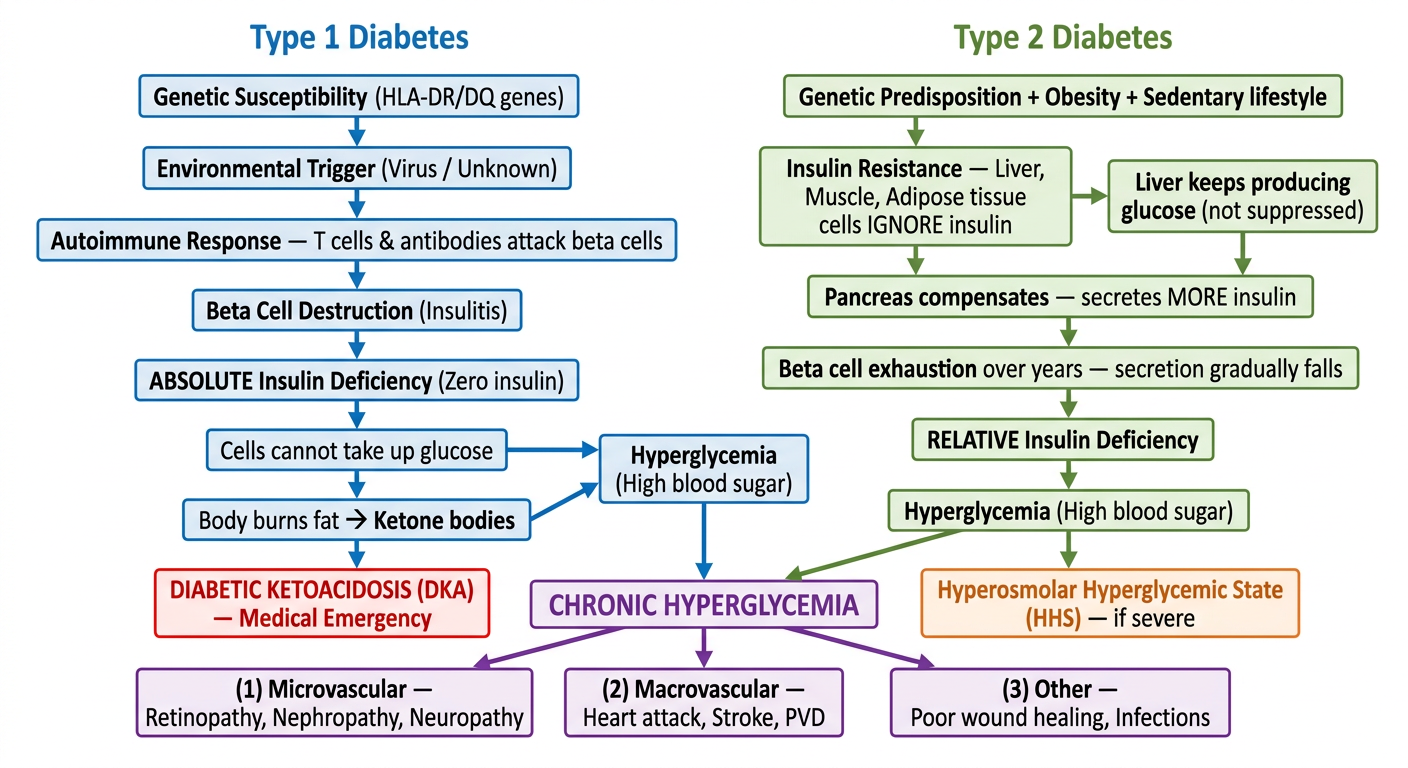
Type 1 (Blue Pathway)
Type 2 (Green Pathway)
Shared End Result (Purple)
- Small vessels - retinopathy, nephropathy, neuropathy
- Large vessels - heart attack, stroke, peripheral vascular disease
- General - infections, poor wound healing
- Type 1 → DKA (due to ketone production from zero insulin)
- Type 2 → HHS (due to severe dehydration from very high blood sugar, but enough insulin to prevent ketosis)