Explain me my cardiac infarction.
Reading File
Finding Sources
Finding Sources
Searching PubMed
"myocardial infarction"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
I have everything I need to write a thorough, well-illustrated explanation. Let me now compose the complete answer.
Myocardial Infarction (Heart Attack) - A Complete Explanation
What Is It?
A myocardial infarction (MI) - commonly called a "heart attack" - is the death (necrosis) of heart muscle resulting from prolonged ischemia (lack of blood supply). The 2018 joint US/European cardiology task force defines it as "the presence of acute myocardial injury detected by abnormal cardiac biomarkers in the setting of evidence of acute myocardial ischemia."
- Robbins & Kumar Basic Pathology, p. 352
The Root Cause: Atherosclerosis
Your heart muscle is fed by three main coronary arteries. Over years, fatty deposits called atherosclerotic plaques build up inside their walls, narrowing the lumen. These plaques are the fundamental underlying problem in the vast majority of MIs. Risk factors that drive this process include:
- Aging (the frequency rises progressively with age)
- Male sex (though the gap narrows after menopause)
- Hypertension, diabetes, high cholesterol, smoking
- About 10% of MIs occur before age 40; 45% before age 65
How the Blockage Happens - Step by Step
Here is the typical sequence of events in a classic MI:
- An atherosclerotic plaque is suddenly disrupted - through erosion, intraplaque hemorrhage, or mechanical stress - exposing the subendothelial collagen and the necrotic contents of the plaque to flowing blood.
- Platelets adhere, aggregate, and activate, releasing thromboxane A2, ADP, and serotonin - all of which trigger further platelet clumping and arterial vasospasm.
- Coagulation is activated by exposed tissue factor, adding to the growing clot.
- Within minutes, the enlarging thrombus completely occludes the coronary artery.
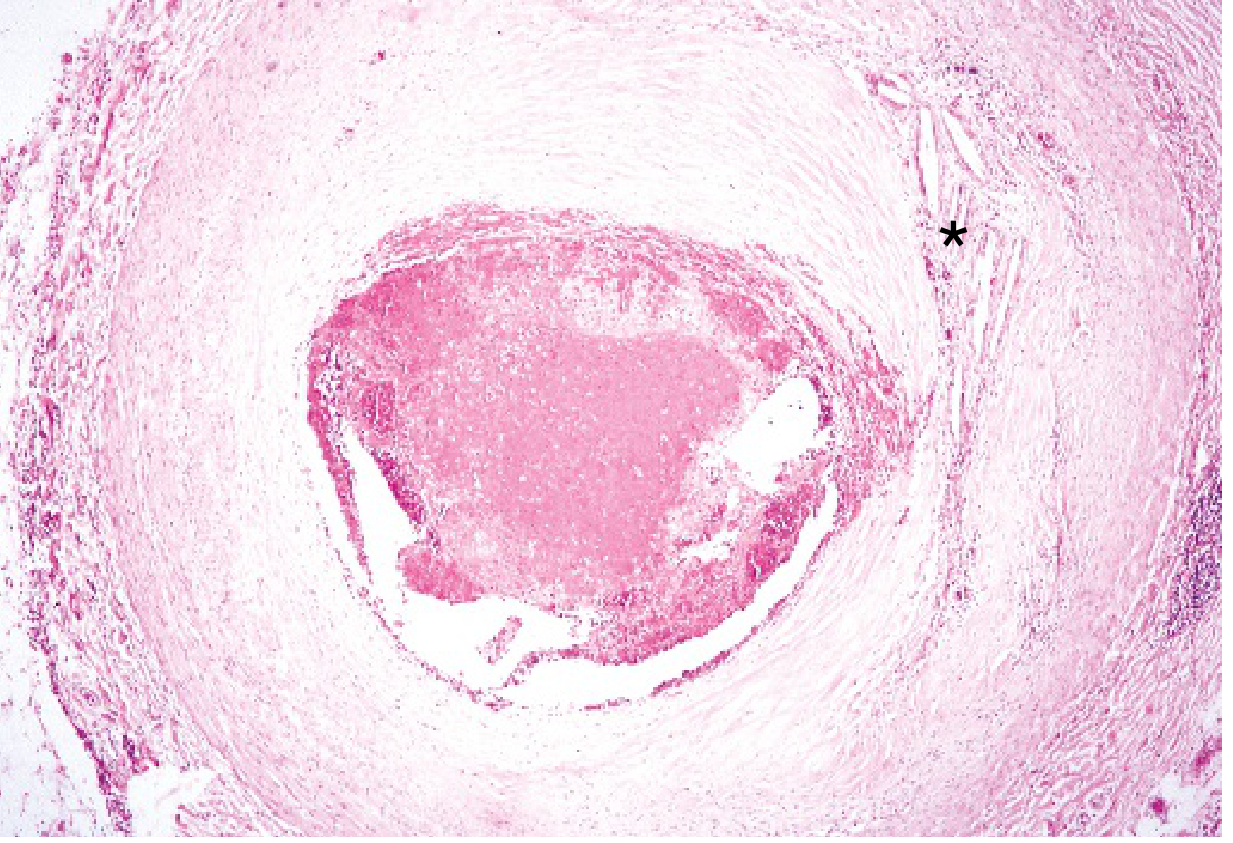
Angiography performed within 4 hours of MI onset shows coronary thrombosis in almost 90% of cases. By 12-24 hours, this drops to 60%, because some thrombi dissolve spontaneously.
- Robbins & Kumar Basic Pathology, p. 353
Below is a histological image of a coronary artery nearly occluded by a fresh thrombus:
Three Mechanisms of Plaque Failure
The Sabiston Textbook of Surgery identifies three distinct ways plaques can trigger an MI:
- Plaque Rupture - The fibrous cap over the plaque tears, exposing its lipid core directly to blood. This most commonly causes STEMI (full-thickness, complete blockage).
- Plaque Erosion - The outer endothelial layer wears away without full rupture, exposing clot-promoting substances. Often causes NSTEMI (partial blockage).
- Calcified Nodule - Hard calcified deposits break through the fibrous cap into the artery lumen.
- Sabiston Textbook of Surgery, p. 2484
What Happens to the Heart Muscle
The progression of damage after coronary occlusion:
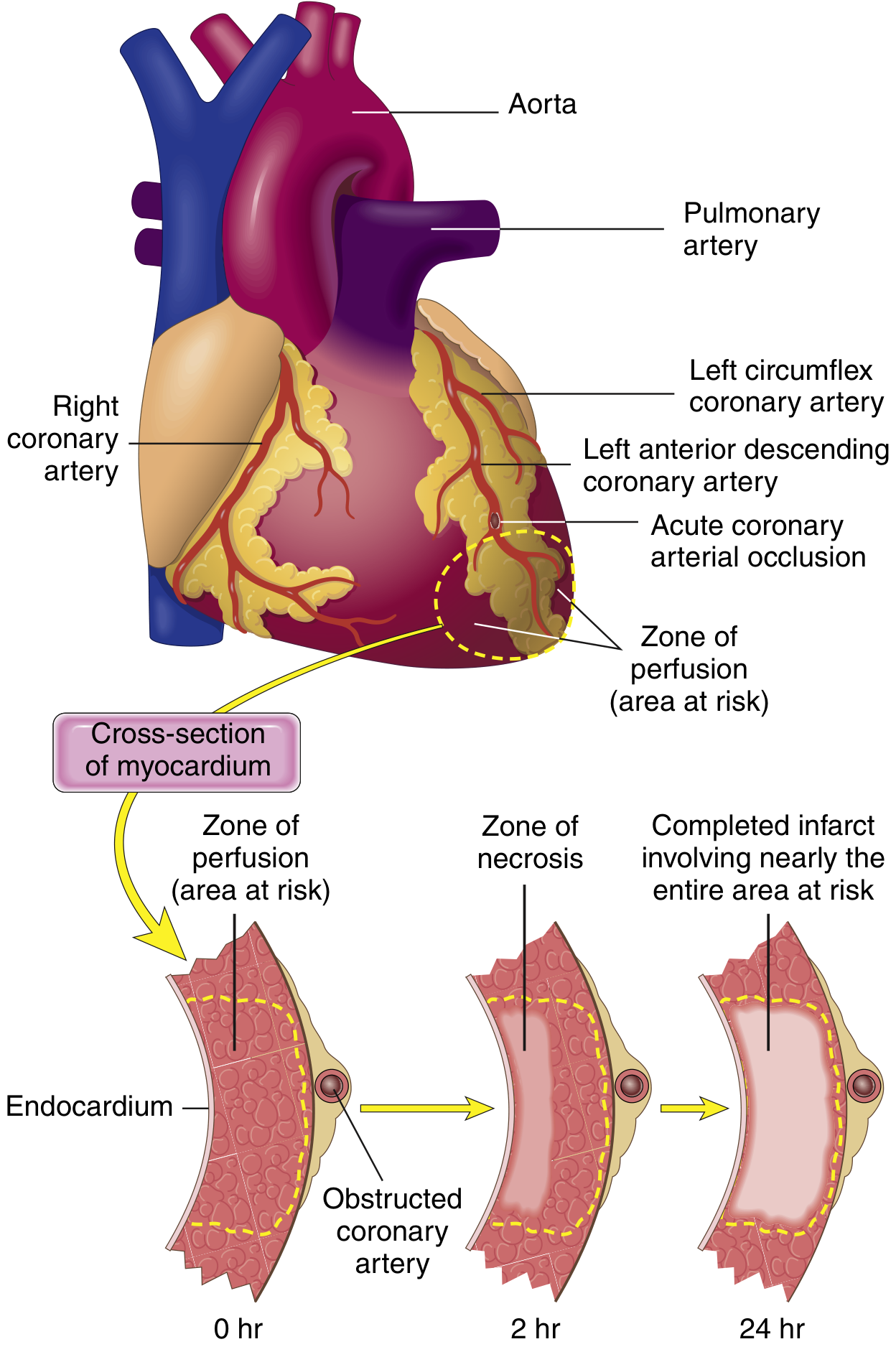
Timeline of cellular death:
- Within seconds: Aerobic metabolism stops, ATP drops, lactic acid accumulates
- Within minutes: Contractility is lost (reversible at this stage)
- 20-40 minutes: Irreversible damage begins - coagulative necrosis of myocytes
- 3-6 hours: The infarct achieves its full extent without intervention
The narrow zone of myocardium immediately beneath the endocardium is paradoxically spared - it can be oxygenated by diffusion directly from the blood inside the ventricle.
The subendocardial layer is the most vulnerable region - it has the highest oxygen consumption and its blood vessels are squeezed shut during each heartbeat contraction.
- Guyton and Hall Textbook of Medical Physiology, p. 271
Which Artery is Blocked, and What Dies?
The location of the MI depends on which artery is occluded:
| Artery | Frequency | Area Affected |
|---|---|---|
| Left Anterior Descending (LAD) | 40-50% | Anterior LV wall, anterior 2/3 of septum, apex |
| Right Coronary Artery (RCA) | 30-40% | Right ventricle, inferior/posterior LV wall |
| Left Circumflex (LCX) | 15-20% | Lateral left ventricle |
- Robbins & Kumar Basic Pathology, p. 355
Types of MI (Fourth Universal Definition)
| Type | Cause |
|---|---|
| Type 1 (Spontaneous) | Plaque rupture/erosion → thrombus → ischemia |
| Type 2 (Ischemic Imbalance) | Supply/demand mismatch - spasm, anemia, arrhythmia, hypotension without thrombosis |
| Type 3 (Sudden Death) | Fatal, no biomarkers obtained in time |
| Type 4a (PCI-related) | Troponin rise within 48h of a coronary angioplasty procedure |
| Type 4b (Stent Thrombosis) | Clot forming inside a previously placed stent |
| Type 5 (CABG-related) | Troponin rise within 48h of bypass surgery |
- Sabiston Textbook of Surgery, p. 2485-2486
Symptoms
The classic presentation includes:
- Substernal chest pain described as pressure, tightness, or squeezing - often radiating to the neck, jaw, or left arm
- Dyspnea (difficulty breathing) from increased cardiac workload and potential pulmonary congestion
- Palpitations and dizziness from arrhythmias
- Diaphoresis (cold sweating), nausea, vomiting
Important: Women are more likely to have atypical symptoms - fatigue, indigestion, abdominal pain - without classic chest pressure. Older patients may also present atypically.
- Sabiston Textbook of Surgery, p. 2486
The ECG Changes Explained
Three electrical abnormalities occur in the infarcted area, all producing the same result:
| Electrical Defect | Direction of Current | ECG Result |
|---|---|---|
| Rapid repolarization (K+ channels open) | Out of infarct | ST elevation |
| Decreased resting membrane potential | Into infarct | TQ depression (recorded as ST elevation) |
| Delayed depolarization | Out of infarct | ST elevation |
-
Acute MI hallmark: ST-segment elevation in leads overlying the infarct
-
After days/weeks: ST normalizes; the dead tissue becomes electrically silent and a Q wave develops (indicating permanent full-thickness scar)
-
Ganong's Review of Medical Physiology, p. 534
Why People Die from MI
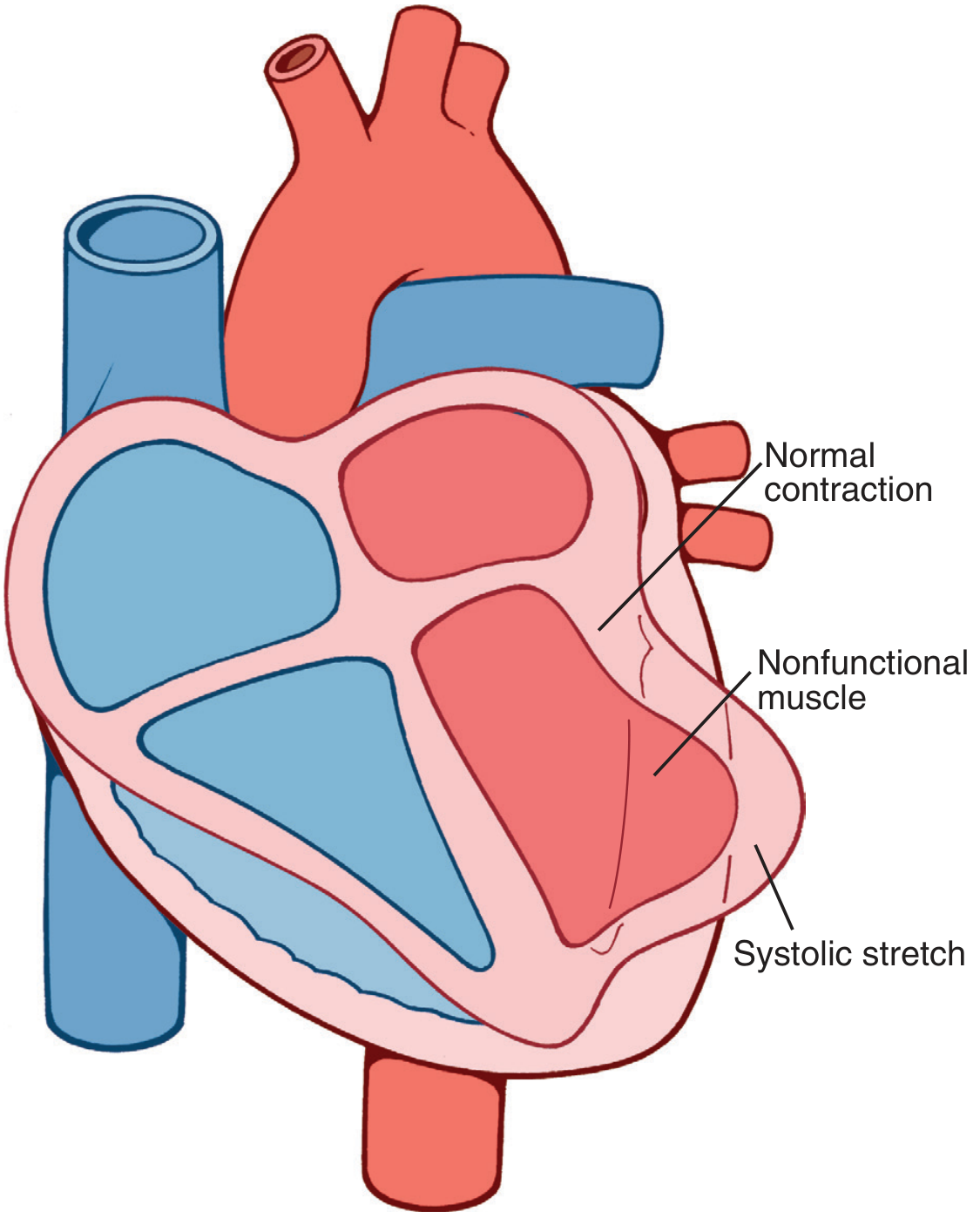
The four main mechanisms of death, from Guyton & Hall:
- Decreased cardiac output / Cardiogenic shock: The infarcted area cannot contract. Worse, when healthy muscle contracts, the dead/stunned area bulges outward - this is called systolic stretch - wasting precious pumping energy.
- Pulmonary edema: Backed-up blood floods the lungs when the left ventricle fails.
- Ventricular fibrillation: Ischemic tissue is electrically unstable; lethal arrhythmias are the most common cause of death (responsible for 80-90% of early deaths).
- Cardiac rupture: The necrotic wall can physically tear, causing sudden catastrophic collapse.
- Guyton and Hall Textbook of Medical Physiology, p. 271-272
The Morphological Timeline (What the Heart Looks Like Over Time)
| Time After MI | Gross Appearance | Microscopic Features |
|---|---|---|
| < 12 hours | Not visible to the naked eye | Wavy fibers, early coagulative necrosis |
| 12-24 hours | Pallor/dark mottling | Loss of nuclei, contraction band necrosis |
| 1-3 days | Pale yellow center with hyperemic border | Neutrophil infiltration |
| 3-7 days | Soft, yellow-tan; maximum softening | Macrophage invasion, phagocytosis of dead cells |
| 1-3 weeks | Gelatinous red-gray rim | Granulation tissue with new blood vessels |
| > 2 months | Firm, white scar | Dense fibrous scar - permanent |
Myocardial necrosis proceeds to scar formation with no significant regeneration - heart muscle cells, once dead, are replaced by fibrous scar tissue.
- Robbins & Kumar Basic Pathology, p. 356
The Critical Time Window
This is why speed matters. The phrase "time is muscle" exists because:
- Irreversible cell death begins at 20-40 minutes of ischemia
- An infarct achieves its full size in 3-6 hours
- Reperfusion (either by thrombolysis or angioplasty) within this window can dramatically reduce the amount of muscle that dies
- Even after timely reperfusion, the rescued muscle can remain dysfunctional for days ("stunned myocardium") before recovering
Recent Evidence Worth Noting
A 2025 meta-analysis (PMID 39298680) found that beta-blockers for secondary prevention after MI may not be as universally beneficial in patients without reduced ejection fraction or heart failure as previously thought - a significant update to traditional practice.
Sources:
- Robbins & Kumar Basic Pathology (Elsevier)
- Guyton and Hall Textbook of Medical Physiology
- Ganong's Review of Medical Physiology, 26th Ed.
- Sabiston Textbook of Surgery, Biological Basis of Modern Surgical Practice
- Braunwald's Heart Disease, A Textbook of Cardiovascular Medicine
This is a shared conversation. Sign in to Orris to start your own chat.