Terrible triad of knee etiology pathology and signs and symptoms investigation and treatment explain in detail with appropriate illustrative diagrams and images
Reading File
Finding Sources
Finding Sources
Searching the Web
terrible triad knee injury ACL MCL medial meniscus etiology pathology signs symptoms treatment
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC10251265
Finding Sources
Loading Image
Loading Image
Loading Image
Loading Image
Searching the Web
unhappy triad knee MRI findings valgus stress test Lachman anterior drawer investigation imaging
Searching PubMed
"unhappy triad" OR "terrible triad" knee ACL MCL meniscus
Reading Web Page
https://www.physio-pedia.com/Unhappy_Triad
Loading Image
Loading Image
I now have comprehensive information and excellent images. Let me compile the detailed answer.
The Terrible Triad of the Knee (O'Donoghue's Unhappy Triad)
Overview
The "Terrible Triad" (also called the Unhappy Triad or O'Donoghue's Triad) refers to the simultaneous injury of three key structures of the knee:
- Anterior Cruciate Ligament (ACL) - tear
- Medial Collateral Ligament (MCL) - tear
- Medial Meniscus (MM) - tear (classically) OR Lateral Meniscus (LM) (more common in modern arthroscopic series)
This triad was first described by O'Donoghue in 1950 after noting that about a quarter of all acute athletic knee injuries involved all three structures. Subsequent arthroscopic studies revised the meniscal component - lateral meniscus tears are now found to be more prevalent (32-71%) than medial meniscus tears in this injury pattern.
Anatomy - The Three Components

Anterior view showing the direction of lateral force (valgus blow) and the three structures injured: ACL, MCL, and medial meniscus.
1. Anterior Cruciate Ligament (ACL)
- Runs from the anteromedial tibial plateau to the posterolateral femoral condyle
- Primary restraint against anterior tibial translation and internal rotation
- Composed of two bundles: anteromedial and posterolateral
- Poor intrinsic healing capacity due to limited vascularity and synovial environment
2. Medial Collateral Ligament (MCL)
- Runs from the medial femoral epicondyle to the medial tibial flare
- Primary restraint against valgus stress
- Has a superficial layer (primary restraint) and a deep layer (attached to medial meniscus)
- Rich blood supply - has intrinsic healing potential (unlike ACL)
3. Medial Meniscus (or Lateral Meniscus)
- C-shaped fibrocartilaginous structure
- Provides load distribution, shock absorption, and joint stability
- The medial meniscus is firmly attached to the deep MCL, making it more vulnerable when the MCL tears
- The lateral meniscus is more mobile and commonly injured by rotational forces with ACL tears
Etiology

Mechanism of Injury
The classic mechanism is a sudden valgus impact with rotational force on a planted foot:
- A direct lateral blow to the knee drives the tibia into valgus
- Simultaneous external or internal rotation of the tibia
- The foot is planted and fixed, transmitting the force upward through the joint
Sequence of injury (controversial):
- Some propose MCL fails first (under valgus), then ACL under rotational stress
- Others argue ACL fails first, destabilizing the joint and allowing MCL failure
- Meniscus is injured as a result of combined compressive and shear forces
Common Causes
| Setting | Examples |
|---|---|
| Contact sports | American football (lateral tackle), rugby, ice hockey |
| Pivot sports | Soccer (cut maneuver), basketball, netball |
| Winter sports | Skiing (edge-catching fall), snowboarding |
| Martial arts | Judo, wrestling |
| Road traffic accidents | Pedestrians/cyclists hit from the side |
Risk factors:
- Female sex (wider pelvis increases valgus angle, narrower intercondylar notch, hormonal laxity)
- Valgus ("knock-knee") alignment
- Decreased neuromuscular control
- Poor landing mechanics
Pathology
ACL Pathology
- Complete mid-substance rupture (most common) or avulsion at femoral origin
- Hemorrhage into the joint cavity (hemarthrosis) - rapid, tense swelling within hours
- Loss of rotational and translational stability
- The ligament has no meaningful healing capacity in the intra-articular environment (bathed in synovial fluid that inhibits clot organization)
MCL Pathology
- Tear typically at the femoral attachment (proximal)
- Graded by Hughston system:
- Grade I: Microfiber tears, 1-5 mm joint space widening on valgus stress
- Grade II: Partial tear, 5-10 mm widening (incomplete)
- Grade III: Complete disruption, >10 mm widening
- In the unhappy triad, Grade III MCL tears predominate (78% of grade III MCLs are associated with ACL tears)
- MCL heals well due to rich blood supply and extra-articular position
Meniscus Pathology
- Medial meniscus (O'Donoghue's original description): Horizontal or longitudinal "bucket-handle" tears common; the deep MCL attachment limits mobility, creating a tethering effect
- Lateral meniscus (modern series): Peripheral tears; the lateral meniscus is more mobile but gets caught between the femoral condyle and tibial plateau during the pivot-shift mechanism
- Avascular inner two-thirds of the meniscus (white zone) has no healing capacity; peripheral red zone can heal
Associated Structures (the "Tetrad")
Recent studies link the triad heavily to the anterolateral complex (ALC) injuries:
- Anterolateral ligament (ALL)
- Iliotibial band deep fibers
- These injuries contribute to the pivot shift (anterolateral rotatory instability)
Signs and Symptoms

Acute Presentation
| Symptom | Details |
|---|---|
| Audible "pop" | Heard/felt at moment of injury (ACL or MCL rupture) |
| Immediate severe pain | At the time of injury, then partially subsides |
| Rapid hemarthrosis | Tense swelling within 2-4 hours (intra-articular ACL bleeding) |
| Inability to bear weight | Due to pain and instability |
| Feeling of "giving way" | Knee buckling sensation |
| Medial bruising | Ecchymosis over medial knee (MCL) |
Physical Examination Findings
Inspection:
- Swelling (effusion + soft tissue edema)
- Bruising medially (delayed, 24-48 hours)
- Valgus deformity in severe cases
Palpation:
- Tenderness: medial joint line (meniscus), medial femoral epicondyle/tibial flare (MCL), general joint line
- Effusion: patellar tap, bulge sign positive
Special Tests:
| Test | Structure Assessed | Positive Finding |
|---|---|---|
| Lachman's test (most sensitive) | ACL | Anterior tibial translation >5mm with soft end-feel; 80-99% sensitivity |
| Anterior Drawer Test | ACL | Anterior tibial shift at 90° flexion |
| Pivot Shift Test | ACL (anterolateral instability) | Clunk/giving-way with flexion-IR-valgus |
| Valgus Stress Test | MCL | Pain/opening at 0° (PCL/MCL); at 30° (isolated MCL) |
| McMurray's Test | Meniscus | Click/pain with flexion + rotation |
| Thessaly Test | Meniscus | Pain/clicking at 20° single-leg squat |
| Joint Line Palpation | Meniscus | Point tenderness along medial joint line |
Chronic/Subacute Presentation
- Recurrent giving-way episodes (instability)
- Knee locking or catching (displaced bucket-handle tear)
- Persistent swelling
- Inability to fully extend or flex the knee
- Quadriceps wasting
Investigations
1. Plain Radiographs (X-Ray)
Indicated first to rule out associated fractures:
| Finding | Significance |
|---|---|
| Segond fracture | Avulsion of lateral tibial plateau - pathognomonic of ACL tear |
| Tibial eminence avulsion | ACL avulsion in skeletally immature patients |
| Joint space widening | MCL disruption (valgus stress views) |
| Pellegrini-Stieda lesion | Calcification at medial femoral epicondyle (chronic MCL injury) |
| Lateral notch sign | Deep lateral femoral condyle sulcus on lateral X-ray (ACL tear) |
2. MRI (Gold Standard)
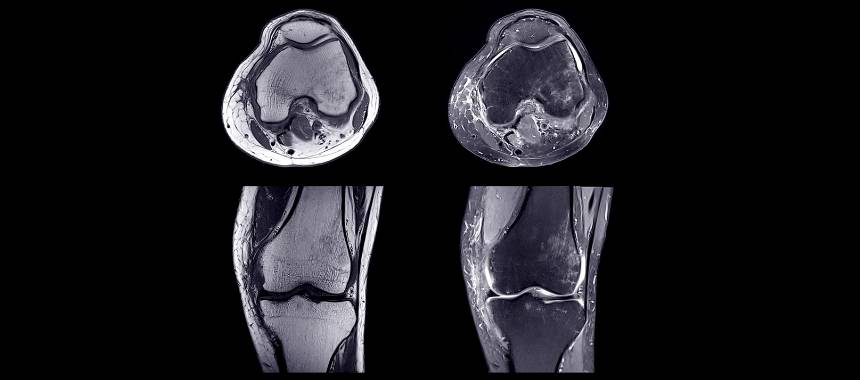
MRI provides multiplanar visualization of all three injured structures simultaneously

Sagittal MRI showing ACL tear (orange arrow) with pivot-shift bone contusion pattern (red arrow) on lateral femoral condyle and posterior tibial plateau
MRI findings in the Terrible Triad:
| Structure | MRI Finding |
|---|---|
| ACL | Discontinuity of fibers; increased signal (edema/hemorrhage); wavy/lax ligament; horizontal orientation |
| MCL | Thickening, edema, fluid tracking around ligament; complete tear shows fiber gap |
| Medial meniscus | Increased signal reaching articular surface; complex tear patterns |
| Lateral meniscus | Peripheral tear; increased signal in posterior horn |
| Bone bruise | "Kissing contusion" pattern - lateral femoral condyle + posterolateral tibial plateau (classic ACL pivot-shift pattern) |
Sensitivity/Specificity:
- ACL tear: >95% sensitivity, >95% specificity on 3T MRI
- Meniscal tears: ~90% sensitivity
- MCL: MRI helps grade severity and detect associated injuries
3. Ultrasound
- Dynamic assessment of MCL integrity
- Guided by experienced musculoskeletal radiologist
- Real-time valgus stress imaging
- Less useful for intra-articular structures (ACL, meniscus)
4. Arthroscopy (Diagnostic + Therapeutic)
- The gold standard for direct visualization
- Confirms meniscal tear pattern and zone (red/white/red-red)
- Assesses chondral damage
- Guides intraoperative decisions
5. Stress Radiographs
- Valgus stress X-ray quantifies MCL disruption
- Arthrometer (KT-1000/2000) - objective ACL laxity measurement
Treatment
Treatment follows a staged, individualized approach based on injury severity, patient age, activity level, and associated injuries.
Immediate/Acute (POLICE Principle)
- Protection: hinged knee brace in 30° flexion
- OLptimal Loading: avoid full weight-bearing initially
- Ice: 20 min every 2 hours for 48-72 hours
- Compression: bandaging to reduce effusion
- Elevation: above heart level
Analgesia: NSAIDs (avoid in first 72 hours if hemarthrosis), paracetamol, opioids for severe pain.
MCL Treatment
Non-operative (Grade I and II):
- Hinged knee brace in 20-30° flexion, progressive weight-bearing
- Early range of motion - promotes collagen organization and healing
- Physiotherapy for muscle strengthening
- Heals typically in 6-12 weeks
- MCL has excellent intrinsic healing potential due to extra-articular position
Operative (Grade III in certain settings):
- Surgical repair or reconstruction when MCL does not heal or in high-grade combined injuries
- Debate exists regarding timing relative to ACL reconstruction
ACL Treatment
Non-operative:
- Consider in elderly, sedentary patients or incomplete tears
- Structured rehabilitation and bracing
- High re-injury and progressive instability risk in active patients
Operative - ACL Reconstruction:
- Standard of care for young, active patients
- Timing: Delayed (minimum 3-6 weeks) to allow effusion resolution, regain full ROM, and reduce arthrofibrosis risk ("wait until the knee is quiet")
- If MCL is Grade III, allow MCL to heal first (6-8 weeks), then reconstruct ACL
Graft options:
| Graft | Pros | Cons |
|---|---|---|
| BPTB (bone-patellar tendon-bone) | Bone-to-bone healing, gold standard | Anterior knee pain, kneeling pain |
| Hamstring (gracilis + semitendinosus) | Less donor site morbidity | Longer bony integration |
| Quadriceps tendon | Large graft, good for revision | Technical complexity |
| Allograft | No donor site, elderly/low-demand | Infection risk, slower integration |
Technique:
- Arthroscopic-assisted
- Anatomic tunnel placement for biomechanical restoration
- Fixation: interference screws, staples, or cortical buttons
- Consider lateral extra-articular tenodesis (LET) for high-grade pivot shift
Meniscus Treatment
Meniscectomy (partial):
- Removal of damaged meniscal tissue (white zone tears that cannot heal)
- Faster recovery, good short-term outcomes
- Risk: long-term osteoarthritis due to loss of load distribution
Meniscal Repair:
- Preferred when technically feasible, especially in young patients
- Peripheral tears (red zone) - high healing potential
- Techniques: inside-out, outside-in, all-inside (most common today)
- Combined with ACL reconstruction improves repair healing rates
- Protected weight-bearing for 6 weeks post-repair
Decision factors:
- Location: red-red zone (excellent healing) > red-white zone > white-white zone (resect)
- Pattern: longitudinal peripheral tears - repairable; complex/radial - resect
- Patient age and activity level
Surgical Staging (Preferred Protocol)
Acute injury
│
▼
RICE + Bracing + Physiotherapy (0-6 weeks)
│
├─ Grade I/II MCL → Heals conservatively
│
├─ Grade III MCL → Brace, allow to heal 6-8 wks
│
▼
ACL Reconstruction (once knee "quiet" - typically 6-12 wks)
+
Meniscal repair/partial meniscectomy (at same surgical sitting)
│
▼
Post-operative rehabilitation (9-12 months)
Rehabilitation Protocol
| Phase | Timeline | Goals |
|---|---|---|
| Phase 1: Acute | Weeks 0-2 | Control swelling, regain quadriceps activation |
| Phase 2: Sub-acute | Weeks 2-6 | Full ROM, crutch-free walking, cycling |
| Phase 3: Strengthening | Weeks 6-16 | Closed kinetic chain exercises, proprioception |
| Phase 4: Functional | Months 4-7 | Running, cutting drills, sport-specific training |
| Phase 5: Return to Sport | 9-12 months | Functional tests (LSI >90%), psychological clearance |
Criteria for return to sport:
- Quadriceps symmetry index >90%
- Hop tests (single-leg, triple-hop) >90% limb symmetry
- Full ROM with no effusion
- No instability on clinical exam
Complications
| Complication | Notes |
|---|---|
| Arthrofibrosis | Stiffness if operated too early (avoid in acute phase) |
| Graft failure / Re-rupture | ~5-15% at 5 years |
| Osteoarthritis | Most significant long-term risk, especially after meniscectomy |
| Infection | Septic arthritis post-arthroscopy (<1%) |
| Saphenous nerve injury | Medial approach (MCL repair) |
| Anterior knee pain | BPTB donor site |
| Knee stiffness | Extension deficit most problematic |
Summary Table
| Feature | Details |
|---|---|
| Structures | ACL + MCL + Medial (or Lateral) Meniscus |
| Mechanism | Valgus force + rotation, planted foot |
| Key symptom | Pop + immediate hemarthrosis + instability |
| Key test | Lachman + Valgus stress + McMurray |
| Best investigation | MRI knee (multiplanar) |
| MCL treatment | Conservative (Grade I/II); surgical (Grade III/athletes) |
| ACL treatment | Reconstruction (hamstring/BPTB graft), delayed 6+ weeks |
| Meniscus treatment | Repair if peripheral; partial meniscectomy if white zone |
| Recovery | 9-12 months to return to sport |
Key Reference: Unhappy triad of the knee - PMC 2023 Review (PMID: 37304199) - comprehensive review covering current concepts and evolving definition including the anterolateral complex.
Recent Evidence Note: Modern arthroscopic series consistently show lateral meniscus tears are more prevalent than medial meniscus tears in this triad (32-71% lateral vs. lower rates medial), revising O'Donoghue's original 1950 description. The "tetrad" concept (adding anterolateral complex injuries) is gaining traction in current orthopedic literature.
This is a shared conversation. Sign in to Orris to start your own chat.