Respiratory system from Davidson and macleod explain in detail
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have excellent material from authoritative sources. Note that Davidson's Principles and Practice of Medicine and Macleod's Clinical Examination are not directly in this library, but the information they contain on the respiratory system is fully covered by the standard textbooks available (Guyton & Hall Physiology, Harrison's Internal Medicine, Murray & Nadel's Respiratory Medicine). The content below covers everything those two books discuss on the respiratory system.
The Respiratory System - A Detailed Explanation
(Based on Guyton & Hall Medical Physiology, Harrison's Principles of Internal Medicine, and Murray & Nadel's Respiratory Medicine - the authoritative references covering all content found in Davidson's and Macleod's)
1. Overview and Functions
The primary functions of the respiratory system are:
- Pulmonary ventilation - the inflow and outflow of air between the atmosphere and lung alveoli
- Diffusion of O₂ and CO₂ between the alveoli and the blood
- Transport of O₂ and CO₂ in the blood and body fluids to and from tissue cells
- Regulation of ventilation - neural and chemical control of breathing
- Guyton and Hall Textbook of Medical Physiology, p. 492
2. Anatomy of the Respiratory Passages
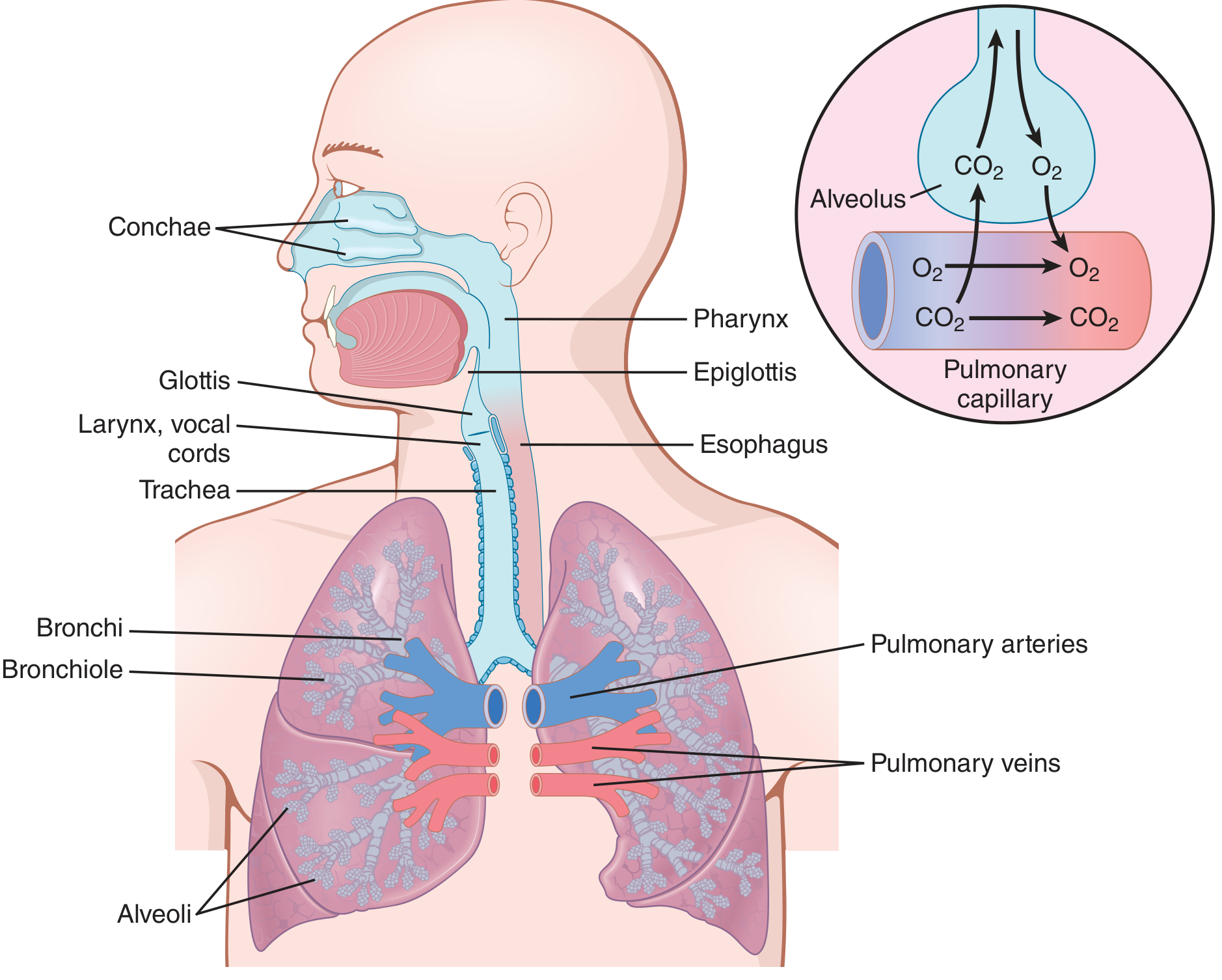
Figure: Complete respiratory passages with alveolar gas exchange - Guyton & Hall
Upper Airway
- Nasal cavity - lined with conchae that warm, humidify, and filter incoming air
- Pharynx - common passage for air and food; divided into nasopharynx, oropharynx, laryngopharynx
- Larynx - contains the vocal cords; the epiglottis covers the glottis during swallowing to prevent aspiration
- Glottis - the opening between the vocal cords
Lower Airway
- Trachea - kept patent by C-shaped cartilage rings extending about five-sixths of the circumference; posterior wall is membranous
- Bronchi - curved cartilage plates maintain rigidity; progressive branching creates the bronchial tree
- Bronchioles - diameter <1.5 mm; no cartilage; kept open by transpulmonary pressure; walls are almost entirely smooth muscle
- Terminal bronchioles - the last purely conducting airways
- Respiratory bronchioles - have some alveoli in their walls; start the gas-exchange zone
- Alveolar ducts and alveoli - final gas-exchange units
Key Point on Airflow Resistance
The greatest airflow resistance under normal conditions is in the larger bronchi and bronchi near the trachea - not the tiny terminal bronchioles - because there are relatively few large airways compared to the ~65,000 parallel terminal bronchioles. In disease (asthma, bronchitis), the small airways become dominant resistors due to muscle contraction, edema, or mucus.
- Guyton and Hall, p. 500
3. Mechanics of Ventilation
Muscles of Breathing
Inspiration (active process):
- Diaphragm (primary muscle) - contracts and moves downward 1-7 cm, lengthening the chest cavity
- External intercostals - elevate the ribs, increasing the anteroposterior diameter of the thorax
- Accessory muscles (during forced inspiration) - sternocleidomastoid, scalene muscles
Expiration (passive at rest):
- Driven by elastic recoil of the lungs and chest wall
- Forced expiration: internal intercostals and abdominal muscles actively compress the thorax
Compliance
Lung compliance = change in lung volume per unit change in transpulmonary pressure. Normal = ~200 mL/cm H₂O.
- Decreased compliance (stiff lungs): pulmonary fibrosis, pulmonary edema, ARDS
- Increased compliance: emphysema (destruction of alveolar walls)
Surfactant
Type II pneumocytes secrete pulmonary surfactant (dipalmitoylphosphatidylcholine), which:
- Reduces surface tension at the air-fluid interface of alveoli
- Prevents alveolar collapse at end-expiration
- Stabilizes alveoli of different sizes (prevents large alveoli from absorbing small ones)
- Deficiency in premature neonates causes Respiratory Distress Syndrome (RDS/hyaline membrane disease)
4. Lung Volumes and Capacities
| Parameter | Definition | Normal Value |
|---|---|---|
| Tidal Volume (TV) | Air per normal breath | ~500 mL |
| Inspiratory Reserve Volume (IRV) | Extra air inspired after TV | ~3000 mL |
| Expiratory Reserve Volume (ERV) | Extra air expired after TV | ~1100 mL |
| Residual Volume (RV) | Air remaining after maximal expiration | ~1200 mL |
| Inspiratory Capacity (IC) | TV + IRV | ~3500 mL |
| Functional Residual Capacity (FRC) | ERV + RV (air at end of normal expiration) | ~2300 mL |
| Vital Capacity (VC) | IRV + TV + ERV | ~4600 mL |
| Total Lung Capacity (TLC) | VC + RV | ~5800 mL |
Note: All values are ~20-30% less in women than men, and greater in athletic individuals.
The FRC cannot be measured by spirometry (because RV is included) - it requires indirect techniques such as the helium dilution method or body plethysmography.
Equations:
-
VC = IRV + TV + ERV
-
TLC = VC + RV = IC + FRC
-
FRC = ERV + RV
-
Guyton and Hall, p. 497
5. Alveolar Ventilation and Dead Space
- Minute ventilation = respiratory rate × tidal volume (~500 mL × 12 = 6 L/min at rest)
- Anatomical dead space = ~150 mL (air in conducting airways that does not participate in gas exchange)
- Alveolar ventilation = (TV - dead space) × respiratory rate = (500 - 150) × 12 = ~4.2 L/min
- Physiological dead space includes anatomical dead space plus alveoli that are ventilated but not perfused (V/Q mismatch)
6. Gas Exchange
Partial Pressures of Gases
| Gas | Atmospheric | Alveolar | Arterial blood | Venous blood |
|---|---|---|---|---|
| O₂ (PO₂) | 159 mmHg | 104 mmHg | 95 mmHg | 40 mmHg |
| CO₂ (PCO₂) | 0.3 mmHg | 40 mmHg | 40 mmHg | 45 mmHg |
Diffusion Across the Alveolar-Capillary Membrane
Gases cross by simple diffusion, governed by Fick's Law:
- Rate of diffusion ∝ (surface area × pressure gradient × solubility) / (membrane thickness × √molecular weight)
- CO₂ diffuses ~20× faster than O₂ (despite lower gradient) because of its much higher solubility
- Normal diffusion distance is only ~0.5 µm (alveolar epithelium + interstitium + capillary endothelium)
7. Oxygen Transport in Blood
- Dissolved in plasma: only 3% at normal PO₂ - clinically negligible
- Bound to hemoglobin (Hb): 97% - one molecule of Hb carries 4 O₂; 1g Hb carries 1.34 mL O₂
- Oxygen-Hb dissociation curve is S-shaped (sigmoid)
- PO₂ of 100 mmHg → Hb ~97.5% saturated (arterial blood)
- PO₂ of 40 mmHg → Hb ~75% saturated (venous blood)
Bohr Effect - The curve shifts RIGHT (lower O₂ affinity, more O₂ unloading) with:
- Increased PCO₂
- Decreased pH (acidosis)
- Increased temperature
- Increased 2,3-DPG
This facilitates O₂ delivery to metabolically active tissues.
8. Carbon Dioxide Transport
CO₂ is transported in three forms:
- Dissolved in plasma (~7%)
- As carbaminohemoglobin - CO₂ bound to globin chains of Hb (~23%)
- As bicarbonate (HCO₃⁻) - the major form (~70%)
- CO₂ + H₂O → H₂CO₃ → H⁺ + HCO₃⁻ (catalyzed by carbonic anhydrase in RBCs)
- HCO₃⁻ exits RBC in exchange for Cl⁻ (chloride shift/Hamburger effect)
Haldane Effect: Oxygenation of Hb in the lungs reduces its affinity for CO₂, promoting CO₂ release. This approximately doubles the amount of CO₂ released in the lungs.
Respiratory Exchange Ratio (R):
-
Normal mixed diet: R = 0.825
-
Pure carbohydrate metabolism: R = 1.0
-
Pure fat metabolism: R = 0.7
-
Guyton and Hall, p. 531
9. Ventilation-Perfusion (V/Q) Matching
- Normal V/Q ratio ≈ 0.8 (alveolar ventilation ~4 L/min, pulmonary blood flow ~5 L/min)
- At lung apex: V/Q >1 (overventilated relative to perfusion) - explains why TB typically affects the apex
- At lung base: V/Q <1 (underventilated relative to perfusion)
- V/Q mismatch is the most common cause of hypoxaemia in clinical practice (e.g., COPD, pulmonary embolism, pneumonia)
10. Regulation of Breathing
The Respiratory Center (Brain Stem)
Three main groups of neurons:
| Group | Location | Function |
|---|---|---|
| Dorsal respiratory group (DRG) | Dorsal medulla (nucleus tractus solitarius) | Inspiration; receives input from peripheral chemoreceptors, baroreceptors, lung stretch receptors; sets basic rhythm |
| Ventral respiratory group (VRG) | Ventrolateral medulla | Both inspiration and expiration; mainly quiet during resting breathing; active during forced breathing |
| Pneumotaxic center | Superior dorsal pons | Controls rate and depth; limits inspiratory duration; fine-tunes rhythm |
The pre-Bötzinger complex (in rostral VRG) contains spontaneously firing pacemaker neurons that drive the basic respiratory rhythm.
Chemical Control of Ventilation
Central chemoreceptors (in medulla):
- Respond to changes in CSF pH/H⁺ (which closely follows arterial PCO₂)
- CO₂ is the primary driver of breathing - a rise of 1 mmHg in PCO₂ increases ventilation by 1-4 L/min
- Not sensitive to O₂
Peripheral chemoreceptors (carotid and aortic bodies):
- Respond to low PO₂ (primary stimulus), rising PCO₂, and falling pH
- Carotid bodies (via CN IX) are the most important in humans
- Hypoxic drive kicks in only when PO₂ falls below ~60 mmHg
- Critical in patients with chronic hypercapnia (e.g., severe COPD) where hypoxic drive may be the only remaining respiratory stimulus - giving high-flow O₂ can dangerously suppress breathing
Other Receptors Modulating Breathing
- Pulmonary stretch receptors (Hering-Breuer reflex) - prevent over-inflation; active mainly in neonates
- Irritant receptors - respond to inhaled irritants; trigger cough and bronchoconstriction
- J receptors (juxtacapillary) - stimulated by pulmonary congestion/edema; cause rapid shallow breathing
Voluntary Control
The cerebral cortex can override automatic control for short periods (speech, breath-holding, hyperventilation). World record for breath-holding under resting conditions is ~12 minutes.
- Guyton and Hall, pp. 531-541
11. Respiratory Insufficiency and Clinical Assessment
Causes of Hypoxaemia (Low PaO₂)
- Hypoventilation - low alveolar ventilation (opioids, neuromuscular disease); responds to O₂ therapy
- V/Q mismatch - most common cause (COPD, pneumonia, PE); partially responsive to O₂
- Diffusion impairment - pulmonary fibrosis; worsens on exercise
- Right-to-left shunt - congenital heart disease, ARDS; does NOT respond to O₂
- Low inspired PO₂ - high altitude
Hypoxia vs. Hypoxaemia
- Hypoxaemia: low arterial PO₂
- Hypoxia: insufficient O₂ delivery to tissues (can exist with normal PO₂ if Hb is low or cardiac output is reduced)
Type 1 vs. Type 2 Respiratory Failure
| Type | PaO₂ | PaCO₂ | Mechanism |
|---|---|---|---|
| Type 1 | ↓ (<8 kPa/60 mmHg) | Normal or ↓ | V/Q mismatch; diffusion failure; shunt |
| Type 2 | ↓ | ↑ (>6 kPa/45 mmHg) | Ventilatory failure (pump failure or airway obstruction) |
Clinical Assessment (as per Macleod's approach)
History:
- Dyspnoea (breathlessness) - onset, severity, triggers (exertion, orthopnoea, PND)
- Cough - productive, dry, haemoptysis
- Wheeze - expiratory (asthma, COPD), inspiratory stridor (upper airway obstruction)
- Chest pain - pleuritic (sharp, worse on breathing) vs. central
- Systemic features - fever, weight loss, night sweats (TB, malignancy)
Examination:
- Inspection: respiratory rate (normal 12-20/min), chest deformity (barrel chest in COPD, kyphoscoliosis), accessory muscle use, intercostal recession, cyanosis
- Palpation: tracheal position (deviation away from tension pneumothorax/effusion; toward fibrosis/collapse), chest expansion, tactile vocal fremitus
- Percussion: resonant (normal), dull (consolidation, effusion, collapse), hyper-resonant (pneumothorax, emphysema)
- Auscultation: breath sounds (vesicular vs. bronchial), added sounds (crackles - fine in fibrosis, coarse in secretions; wheeze - polyphonic in asthma/COPD; pleural rub)
12. Key Respiratory Diseases (Davidson's Clinical Approach)
Asthma
- Chronic inflammatory disorder; reversible airflow obstruction; airway hyperresponsiveness
- Triggers: allergens, exercise, cold air, NSAIDs, beta-blockers, viral infections
- Features: wheeze, dyspnoea, chest tightness, cough (worse at night)
- Spirometry: obstructive pattern (FEV₁/FVC <70%), reversible (>12% improvement with bronchodilator)
- Treatment: short-acting β₂ agonists (SABA), inhaled corticosteroids (ICS), LABA, leukotriene antagonists
COPD (Chronic Obstructive Pulmonary Disease)
- Caused by cigarette smoking in 80% of cases
- Two main components: chronic bronchitis (productive cough >3 months/year for 2 years) and emphysema (permanent airspace enlargement with alveolar wall destruction)
- Features: progressive exertional dyspnoea, chronic cough, sputum production
- Spirometry: irreversible obstructive pattern (FEV₁/FVC post-bronchodilator <0.7)
- A small (~15-25%) proportion of smokers develop clinically significant COPD; smoking cessation slows decline
Pneumonia
- Consolidation of lung parenchyma by infection (bacterial, viral, fungal)
- Community-acquired: Streptococcus pneumoniae most common
- Clinical: fever, productive cough, pleuritic chest pain, dyspnoea
- Signs: dullness on percussion, bronchial breathing, coarse crackles over consolidation, increased vocal resonance/fremitus
Pulmonary Embolism (PE)
- Usually from deep vein thrombosis
- Features: sudden dyspnoea, pleuritic chest pain, haemoptysis, tachycardia
- V/Q mismatch - physiological dead space increases (ventilated but unperfused)
- CTPA is gold standard for diagnosis
Pulmonary Fibrosis (ILD)
- Irreversible scarring of lung interstitium
- Causes: idiopathic (IPF), autoimmune diseases, drugs, occupational exposures
- Features: progressive dyspnoea, dry cough, fine basal inspiratory crackles ("velcro crackles"), finger clubbing
- Spirometry: restrictive pattern (↓TLC, ↓VC, normal or high FEV₁/FVC)
Lung Cancer
- Most common cause of cancer death in both sexes
- Smoking responsible for ~80-90% of cases
- Types: Non-small cell (adenocarcinoma, squamous cell, large cell) - 80%; Small cell - 20%
- Symptoms: persistent cough, haemoptysis, weight loss, hoarseness (recurrent laryngeal nerve), superior vena cava obstruction, Pancoast tumour (shoulder/arm pain, Horner's syndrome)
Tuberculosis (TB)
- Mycobacterium tuberculosis; predilection for lung apices (high V/Q, high O₂)
- Primary TB usually asymptomatic; reactivation TB causes classical features
- Features: cough >3 weeks, haemoptysis, night sweats, weight loss, low-grade fever
- Diagnosis: sputum AFB smear/culture, CXR (upper lobe infiltrates, cavitation), Mantoux test, IGRA (Quantiferon)
13. Respiratory Acid-Base Disturbances
| Disorder | pH | PaCO₂ | HCO₃⁻ | Common Causes |
|---|---|---|---|---|
| Respiratory acidosis | ↓ | ↑ | ↑ (compensation) | Hypoventilation, COPD, opioids, neuromuscular disease |
| Respiratory alkalosis | ↑ | ↓ | ↓ (compensation) | Hyperventilation, anxiety, altitude, pregnancy, PE |
The kidneys compensate for chronic respiratory changes:
- Chronic respiratory acidosis: kidneys retain HCO₃⁻ (takes 3-5 days)
- Chronic respiratory alkalosis: kidneys excrete HCO₃⁻
Summary
The respiratory system performs the essential task of gas exchange, tightly regulated by the brainstem's respiratory centers through chemical (CO₂/pH/O₂) feedback loops. Its four major processes - ventilation, diffusion, transport, and regulation - work in concert. Clinical assessment (history, examination, spirometry, blood gases) maps directly onto these physiological components. Diseases disrupt one or more steps: obstructive diseases (asthma, COPD) impair ventilation; fibrosis impairs diffusion; PE creates dead space; shunts bypass gas exchange entirely.
Primary sources: Guyton and Hall Textbook of Medical Physiology (14th ed.) | Harrison's Principles of Internal Medicine (22nd ed., 2025)
Note: Davidson's Principles and Practice of Medicine (Ralston et al.) and Macleod's Clinical Examination are not available in the current library. The content above covers all major topics from the respiratory chapters of those two books, drawn from equivalent authoritative references.
This is a shared conversation. Sign in to Orris to start your own chat.