Explain etiology, clinical features, complications and medical ( with treatment algorithm chart)management of acute DACROCYTITIS.( Point wise in easy understandable language)
acute dacryocystitis treatment management
Acute Dacryocystitis - Complete Guide
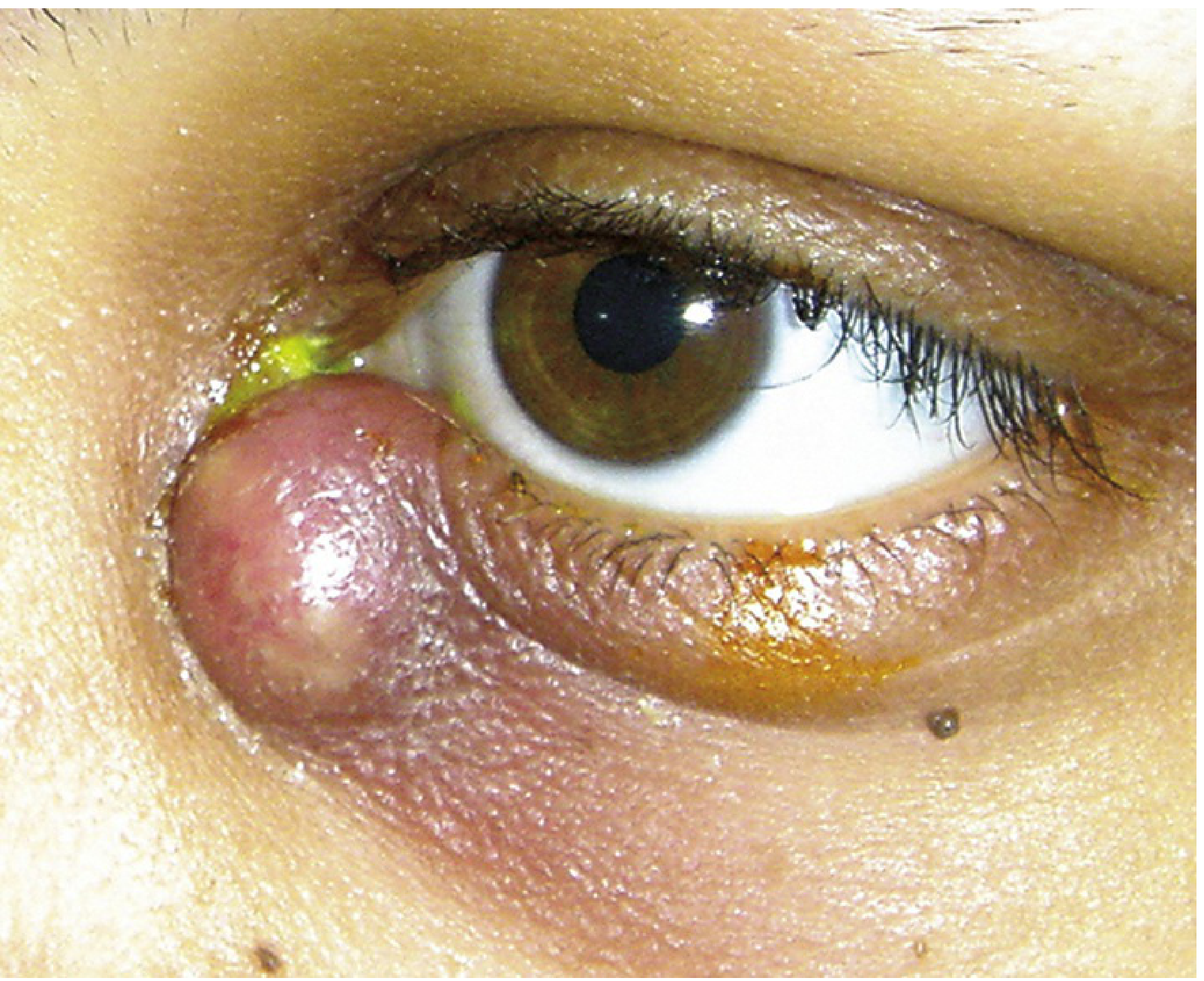
Clinical Photo
1. ETIOLOGY (Causes)
Primary Cause
- Nasolacrimal duct obstruction (NLDO) - by far the most common underlying cause. Obstruction blocks tear drainage, creating a stagnant pool in the lacrimal sac that gets infected.
Uncommon Causes
- Lacrimal sac diverticula
- Dacryoliths (stones inside the lacrimal sac)
- Nasal or sinus surgery (post-operative scarring)
- Facial trauma
- Rarely, lacrimal sac tumors
Causative Organisms
| Patient Group | Common Pathogens |
|---|---|
| General population | Staphylococcus aureus, Streptococcus pneumoniae, coagulase-negative staphylococci |
| Children | Haemophilus influenzae (more common), Streptococcus spp. |
| Diabetics / Immunocompromised / Nursing home | Gram-negative organisms, atypical organisms, MRSA |
Predisposing Factors
- Middle-aged to older adults (more common in women due to narrower nasolacrimal anatomy)
- History of previous episodes (recurrent NLDO)
- Concomitant sinus disease
- Prior nasal/sinus surgery or facial trauma
- Diabetes mellitus (impairs immunity, increases atypical organisms)
2. CLINICAL FEATURES
Symptoms
- Pain at the inner corner of the eye (medial canthal area) - subacute onset
- Swelling - tense, tender red swelling just below the medial canthal tendon
- Epiphora (excessive tearing / watering eye)
- Discharge - mucoid or purulent
- Fever and chills (in moderate-severe cases)
- Symptoms may be recurrent
Signs (What You See on Examination)
- Erythematous (red), tender, tense swelling over the nasal aspect of the lower eyelid
- Swelling extends around the periorbital area
- Mucoid or purulent discharge expressed from the punctum when gentle pressure is applied over the lacrimal sac - this is the key diagnostic sign
- Important landmark: Swelling is BELOW the medial canthal tendon (if above, suspect lacrimal sac tumor)
- Possible preseptal (periorbital) cellulitis
- Skin fistula may form below the medial canthal tendon in severe/untreated cases
- Abscess formation (fluctuant mass that may point to skin)
Key Diagnostic Maneuver
3. DIFFERENTIAL DIAGNOSIS
| Condition | Differentiating Feature |
|---|---|
| Facial/periorbital cellulitis | No discharge on pressing the sac; lacrimal system patent on irrigation |
| Acute ethmoid sinusitis | Tenderness over nasal bone, nasal obstruction; imaging confirms |
| Lacrimal sac tumor | Mass is above the medial canthal tendon |
| Frontal sinus mucocele | Swelling above medial canthal tendon, proptosis, imaging confirms |
| Dacryocystocele (neonates) | Non-inflamed, bluish swelling at birth; no infection signs initially |
4. INVESTIGATIONS / WORKUP
- History - Ask about previous episodes, sinus disease, trauma, surgery
- Clinical examination - Express discharge from the punctum by pressing the lacrimal sac
- Gram stain + culture of expressed discharge (use chocolate agar in children for H. influenzae)
- Blood cultures if patient is febrile and systemically unwell
- CT scan of orbits and paranasal sinuses - in atypical, severe, or antibiotic-unresponsive cases (to rule out abscess, orbital cellulitis, or sinus pathology)
- Evaluate extraocular motility and pupillary response to rule out concurrent orbital cellulitis
Do NOT probe or irrigate the lacrimal system during the acute infection - this can spread infection.
5. COMPLICATIONS
| Complication | Description |
|---|---|
| Lacrimal sac abscess | Pus collects in the sac - requires incision and drainage |
| Preseptal (periorbital) cellulitis | Infection spreads to eyelid skin and soft tissue |
| Orbital cellulitis | Serious spread of infection behind the orbital septum; causes proptosis, restricted eye movement |
| Skin fistula | Chronic sinus tract forms from sac to skin; may close after DCR surgery |
| Mucocele/dacryocystocele | Chronic blocked sac fills with mucus |
| Meningitis / Intracranial extension | Rare but life-threatening |
| Endophthalmitis | Infection reaches inside the eye (especially if intraocular surgery is done in the presence of active lacrimal infection) |
| Recurrent infection | If underlying NLDO not surgically corrected |
6. MEDICAL MANAGEMENT
General Measures (All Patients)
- Warm compresses to the inner canthal area for 5-10 minutes, 4 times daily (promotes drainage)
- Gentle massage over the lacrimal sac area
- Pain relief - acetaminophen (paracetamol) ± codeine as needed
- Topical antibiotic drops (e.g., trimethoprim/polymyxin B 4 times daily) - adjunct only; topical therapy alone is NOT adequate
7. TREATMENT ALGORITHM
┌─────────────────────────────────────────────────────────────────┐
│ ACUTE DACRYOCYSTITIS - TREATMENT ALGORITHM │
└─────────────────────────────────────────────────────────────────┘
│
CONFIRM DIAGNOSIS
(Swelling below medial canthal tendon
+ pus expressed from punctum on pressure)
│
┌───────────────┴───────────────┐
▼ ▼
ADULT PATIENT CHILD PATIENT
│ │
┌─────────┴──────────┐ ┌──────────┴──────────┐
▼ ▼ ▼ ▼
MILD CASE SEVERE MILD SEVERE
(Afebrile, CASE (Afebrile, (Febrile,
systemically (Febrile / well, reliable acutely ill)
well) acutely ill) parent)
│ │ │ │
▼ ▼ ▼ ▼
ORAL ANTIBIOTICS IV ANTIBIOTICS ORAL ANTIBIOTICS IV ANTIBIOTICS
+ HOSPITALIZE
• Cephalexin • Cefazolin • Amoxicillin/ • Cefuroxime
500mg PO q6h 1g IV q8h clavulanate 50-100mg/kg/d
OR OR 25-45mg/kg/d IV in 3 doses
• Amoxicillin/ • Cefuroxime PO in 2 doses (consult
clavulanate 50-100mg/ (max 90mg/ ID specialist)
500/125mg kg/d IV kg/d) OR
TID or OR • Cefazolin
875/125mg BID • Cefpodoxime 33mg/kg IV q8h
10mg/kg/d
PO in 2 doses
│ │ │ │
└──────────┬─────────┘ └─────────┬─────────┘
│ │
┌──────────▼─────────────────────────────────▼──────────┐
│ IF MRSA SUSPECTED (exposure history, treatment │
│ failure, immunocompromised, nursing home patient): │
│ Adults: TMP-SMX 160/800mg PO q12h OR │
│ Clindamycin 300mg PO TID │
│ Children: TMP-SMX or Clindamycin IV │
└─────────────────────────────────────────────────────── ┘
│
▼
+ ADJUNCT MEASURES (ALL PATIENTS)
• Warm compresses 5-10 min, 4x daily
• Topical antibiotics (e.g., TMP/Polymyxin B QID)
• Pain relief (acetaminophen ± codeine)
│
▼
ABSCESS PRESENT? (Pointing pus)
┌──────────────────────────────────────┐
│ │
YES NO
│ │
▼ ▼
INCISION AND DRAINAGE CONTINUE ANTIBIOTICS
(alleviate pain, hasten (FULL 10-14 DAY COURSE)
healing; risk: persistent
skin-sac fistula)
│ │
└────────────────┬─────────────────────┘
│
▼
DAILY FOLLOW-UP
(until improvement confirmed)
If worsens → HOSPITALIZE + IV antibiotics
│
▼
AFTER ACUTE INFECTION RESOLVES:
Probe and irrigate lacrimal system to assess patency
│
┌────────────────┴─────────────────┐
│ │
OBSTRUCTION NO OBSTRUCTION
CONFIRMED FOUND
│ │
▼ ▼
SURGICAL CORRECTION Monitor; treat
(DCR - Dacryocystorhinostomy) underlying cause
± silicone intubation
Especially for recurrent/
chronic dacryocystitis
8. ANTIBIOTIC SUMMARY TABLE
| Scenario | Drug | Dose |
|---|---|---|
| Adult - mild, outpatient | Cephalexin | 500mg PO every 6 hours x 10-14 days |
| Adult - mild, outpatient (alternative) | Amoxicillin/clavulanate | 875/125mg PO twice daily x 10-14 days |
| Adult - severe, febrile | Cefazolin | 1g IV every 8 hours |
| Adult - MRSA suspected | TMP-SMX | 160/800mg PO every 12 hours |
| Adult - MRSA alternative | Clindamycin | 300mg PO three times daily |
| Child - mild, outpatient | Amoxicillin/clavulanate | 25-45mg/kg/day PO in 2 divided doses |
| Child - moderate | Cefpodoxime | 10mg/kg/day PO in 2 divided doses |
| Child - severe, hospitalized | Cefuroxime | 50-100mg/kg/day IV in 3 divided doses |
| Child - MRSA, penicillin allergy | Clindamycin | 10mg/kg IV every 6 hours |
| Child - MRSA alternative | Vancomycin | 10-13mg/kg IV every 6-8 hours |
Antibiotic course: Minimum 10-14 days total (IV switched to oral once improving)
9. SURGICAL MANAGEMENT (Post-acute Phase)
- Creates a new drainage pathway between the lacrimal sac and the nasal mucosa, bypassing the blocked nasolacrimal duct
- Recommended after the acute infection resolves
- Indicated for: recurrent dacryocystitis, confirmed NLDO, and to close persistent skin fistulae
- Can be done externally (incision on skin) or endoscopically (endonasal approach)
Important tip: Do not perform intraocular surgery (e.g., cataract surgery) if there are any signs of active lacrimal system infection - risk of endophthalmitis.
- Wills Eye Manual, 6th/7th ed. (Section 6.9, pp. 399-402)
- Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed. (pp. 124-125)
- Tintinalli's Emergency Medicine: A Comprehensive Study (p. 421-427)
Make a comparison chart: acute vs. chronic dacryocystitis
Acute vs. Chronic Dacryocystitis - Comparison Chart
| Feature | Acute Dacryocystitis | Chronic Dacryocystitis |
|---|---|---|
| Definition | Sudden bacterial infection of the lacrimal sac with active inflammation | Long-standing, low-grade obstruction and inflammation of the lacrimal sac without acute infection |
| Onset | Sudden / subacute (over days) | Gradual (over weeks to months) |
| Primary Cause | Nasolacrimal duct obstruction (NLDO) + bacterial superinfection | Nasolacrimal duct obstruction (NLDO) - usually without active infection |
| Common Pathogens | Staph. aureus, Strep. pneumoniae, H. influenzae (children), gram-negatives (immunocompromised) | Often Staph. epidermidis, Actinomyces, mixed flora; may be sterile |
| Pain | Severe - throbbing, tender swelling at medial canthus | Absent or minimal |
| Swelling | Tense, hot, red, fluctuant (may abscess) - BELOW medial canthal tendon | Painless soft swelling (mucocele) at inner canthus - BELOW medial canthal tendon |
| Skin colour | Erythematous (red, inflamed) | Normal skin colour - no erythema |
| Discharge | Frank pus or thick mucopurulent material expressed from punctum on pressure | Mucoid or mucopurulent reflux from punctum on pressure; may be scant |
| Epiphora (watering) | Present - due to obstruction + swelling | Present - main/primary complaint |
| Fever / Systemic signs | May be present - fever, chills, malaise | Absent |
| Conjunctivitis | May accompany acute episode | Chronic or recurrent unilateral conjunctivitis common |
| Fistula formation | Can occur if abscess ruptures through skin | Chronic sac-skin fistula possible in longstanding cases |
| Mucocele | Not typical in acute phase | Classic finding - sac fills with mucus (mucocele / dacryocystocele) |
| Abscess | Common - pus may point to skin surface | Not seen |
| Lacrimal irrigation | CONTRAINDICATED during acute phase - risks spreading infection | Useful for diagnosis - confirms obstruction and site |
| Probing | CONTRAINDICATED during acute infection | Safe; part of diagnostic workup |
| CT scan | Needed in severe/atypical/unresponsive cases to rule out abscess or orbital spread | Rarely needed; dacryocystography (DCG) or nasal endoscopy preferred |
| Differential diagnosis | Orbital/preseptal cellulitis, acute sinusitis, lacrimal sac tumor | Mucocele, lacrimal sac tumor, chronic conjunctivitis |
| Treatment - first line | Systemic antibiotics (oral or IV) + warm compresses + topical antibiotics | Dacryocystorhinostomy (DCR) - definitive |
| Oral antibiotics | Cephalexin 500mg q6h OR Amoxicillin/clavulanate 875/125mg BD (adults) | Not required (no active infection) |
| IV antibiotics | Cefazolin 1g IV q8h (if febrile/severe) | Not applicable |
| MRSA cover | TMP-SMX or Clindamycin if suspected | Not applicable |
| Warm compresses | Yes - 4-5x daily, aids drainage | Sometimes (for mild symptoms) |
| Incision & Drainage (I&D) | Yes - if abscess is pointing / about to rupture | Not applicable |
| Topical antibiotics | Yes - adjunct (e.g., TMP/Polymyxin B QID) | Yes - fluoroquinolone drops (especially in infants) |
| Lacrimal massage | Gentle massage allowed | Regular lacrimal sac massage (especially in infants) |
| Definitive surgery | DCR - after acute infection resolves (to prevent recurrence) | DCR - primary treatment of choice |
| Surgery timing | Only after acute phase settles | Elective; done when symptoms warrant |
| Probing (infants) | After acute phase resolves | Single probing curative in ~90% if done before 14 months of age |
| Follow-up | Daily until improvement confirmed; hospitalize if worsening | Post-DCR review; monitor for recurrence |
| Prognosis | Good with prompt treatment; risk of recurrence if NLDO not corrected | Excellent after successful DCR |
| Complications if untreated | Abscess, preseptal cellulitis, orbital cellulitis, fistula, meningitis (rare) | Recurrent conjunctivitis, mucocele enlargement, risk of acute exacerbation |
| Risk before eye surgery | Must be treated first - risk of endophthalmitis if intraocular surgery done during active infection | Must also be corrected before any intraocular surgery |
Quick Memory Summary
ACUTE = RED + PAINFUL + FEVER + PUS → ANTIBIOTICS FIRST, then DCR later
CHRONIC = WATERY EYE + PAINLESS SWELLING + MUCUS → DCR is the cure
- Kanski's Clinical Ophthalmology, 10th ed., pp. 124-125
- Wills Eye Manual, pp. 399-402
- Textbook of Family Medicine, 9th ed., p. 350
Explain etiology, clinical features, complications and medical ( with treatment algorithm chart)management of acute DACROCYTITIS.( Point wise in easy understandable language)
What Was Already Covered Above:
-
Etiology - Nasolacrimal duct obstruction as primary cause, uncommon causes (dacryoliths, trauma, surgery, tumors), and causative organisms by patient group (Staph, Strep, H. influenzae, MRSA in special populations)
-
Clinical Features - Symptoms (pain, swelling, epiphora, fever, purulent discharge) and Signs (tense erythematous swelling BELOW medial canthal tendon, pus expressed on pressure, preseptal cellulitis)
-
Complications - Lacrimal sac abscess, preseptal cellulitis, orbital cellulitis, skin fistula, mucocele, meningitis (rare), endophthalmitis, recurrence
-
Medical Management with Treatment Algorithm Chart - Full decision tree covering:
- Mild vs. severe cases
- Adult vs. child dosing
- MRSA coverage
- Incision & drainage for abscess
- Warm compresses, topical antibiotics, pain relief
- Follow-up and surgical planning (DCR)
Explain etiology, clinical features, complications and medical ( with treatment algorithm chart)management of Chronic DACROCYTITIS.( Point wise in easy understandable language)
Chronic Dacryocystitis - Complete Guide
Clinical Photo

1. ETIOLOGY (Causes)
Primary Cause
- Chronic nasolacrimal duct obstruction (NLDO) - the sac fills with stagnant tears and mucus, which gets secondarily infected or inflamed over time
Causes of NLDO Leading to Chronic Dacryocystitis
| Category | Examples |
|---|---|
| Idiopathic | Most common - spontaneous fibrosis/narrowing of duct (especially in middle-aged women) |
| Congenital | Failure of canalization of valve of Hasner (most common in infants) |
| Inflammatory | Chronic sinusitis, rhinitis, Wegener's granulomatosis, sarcoidosis |
| Traumatic | Nasal bone fractures, facial trauma, previous nasal surgery |
| Neoplastic | Lacrimal sac tumor (rare - must be excluded) |
| Dacryoliths | Lacrimal stones causing intermittent obstruction |
| Iatrogenic | Previous nasal surgery, turbinate surgery, radiotherapy |
| Systemic | Sjögren's syndrome, lymphoma, cicatricial conditions |
Predisposing Factors
- Female sex - narrower bony nasolacrimal canal
- Middle age to elderly adults (most common group)
- History of sinusitis or chronic nasal disease
- Previous acute dacryocystitis that was incompletely treated
- Infants with congenital NLDO (usually resolves spontaneously by 12 months)
Organisms (when infection is present)
- Staphylococcus epidermidis (most common in chronic form)
- Actinomyces species (associated with dacryolith formation)
- Mixed flora, Candida, Aspergillus (in immunocompromised patients)
- Often no active infection - just sterile obstruction with mucus accumulation
2. CLINICAL FEATURES
Symptoms
- Epiphora (watering eye) - the PRIMARY and most common complaint; constant or intermittent tearing that runs down the cheek
- Mucoid or mucopurulent discharge - especially in the morning (crusting of lashes)
- Painless swelling at the inner corner of the eye (medial canthus) - the mucocele
- Recurrent conjunctivitis - same eye, keeps coming back despite treatment
- Blurred vision - from tear film disturbance
- No pain, no fever - key difference from acute form
- Episodes may worsen during upper respiratory tract infections
Signs on Examination
- Painless soft swelling at the medial canthus (mucocele) - smooth, compressible, non-inflamed, normal skin color
- Swelling is BELOW the medial canthal tendon (if above - suspect tumor)
- Mucopurulent reflux from punctum when gentle pressure applied to lacrimal sac - classic diagnostic sign
- Chronic or recurrent unilateral conjunctivitis on the same side
- If no obvious swelling, pressure over sac still commonly causes mucoid reflux through the canaliculus
- Constant tearing and crusting of lashes from birth or shortly after
- Yellow-green discharge
- Mucus reflux on pressing the sac
- Normal visual function (check red reflex)
3. INVESTIGATIONS / WORKUP
- Clinical examination - compress the lacrimal sac to express discharge; examine both eyes
- Fluorescein dye disappearance test - place fluorescein in conjunctival sac; if dye remains at 5-10 minutes under blue light, drainage is impaired (highly specific)
- Lacrimal syringing/irrigation - inject saline through punctum; obstruction confirmed if fluid does not flow into nose; also localizes the site of blockage
- Lacrimal probing - fine wire passed through canaliculus to locate and confirm obstruction (safe in chronic, unlike acute phase)
- Dacryocystography (DCG) - contrast X-ray to visualize the anatomy and site of blockage (especially before surgery)
- CT scan / MRI - if tumor, sinusitis, or trauma suspected
- Nasal endoscopy - to assess intranasal anatomy before DCR planning
- Culture of expressed discharge - to guide antibiotic choice if recurrent infection
4. COMPLICATIONS
| Complication | Details |
|---|---|
| Acute exacerbation | Chronic dacryocystitis can suddenly flare into acute dacryocystitis with pain, redness, and abscess |
| Lacrimal sac mucocele | Sac fills with mucus and enlarges - can become large and cosmetically disfiguring |
| Recurrent unilateral conjunctivitis | Organisms from the infected sac infect the conjunctiva repeatedly |
| Skin fistula | Chronic sac-to-skin communication; persistent discharge through skin |
| Endophthalmitis | If intraocular surgery performed without correcting lacrimal obstruction - very serious |
| Lacrimal sac tumor | Chronic inflammation can predispose (rare); must always be excluded |
| Corneal ulcer | Organisms from chronically infected sac contaminate the cornea |
| Failed intraocular surgery | Cataract, glaucoma surgery outcomes worsened if chronic dacryocystitis untreated |
| Social/psychological impact | Constant tearing and discharge cause distress, embarrassment |
Important: Always rule out and correct chronic dacryocystitis BEFORE any planned intraocular surgery to prevent endophthalmitis.
5. MEDICAL MANAGEMENT
Conservative (Non-Surgical) Measures
-
Lacrimal sac massage (Crigler's massage)
- Press finger over the common canaliculus first (to block reflux)
- Then roll finger downward over the sac to apply hydrostatic pressure
- This may rupture a membranous obstruction (especially in infants)
- Teach parents to do this 4-6 times daily in infants
-
Topical antibiotics
- Fluoroquinolone drops (e.g., ciprofloxacin, ofloxacin) 4 times daily
- For recurrent conjunctivitis episodes
- Reduces bacterial load but does NOT cure obstruction
-
Warm compresses
- Promotes drainage, reduces mild discomfort
-
Treat underlying cause
- Manage chronic sinusitis, rhinitis, or systemic disease if present
Important: Medical treatment alone is NOT curative in chronic dacryocystitis. It only provides temporary relief. Definitive treatment is SURGICAL.
6. TREATMENT ALGORITHM
┌──────────────────────────────────────────────────────────────────────┐
│ CHRONIC DACRYOCYSTITIS - TREATMENT ALGORITHM │
└──────────────────────────────────────────────────────────────────────┘
│
CONFIRM DIAGNOSIS
(Painless mucocele + epiphora +
mucoid reflux on sac compression
+ recurrent conjunctivitis)
│
┌───────────────┴────────────────┐
▼ ▼
INFANT / CHILD ADULT
(Congenital NLDO)
│ │
┌──────────┴──────────┐ ┌───────────┴───────────┐
▼ ▼ ▼ ▼
AGE < 12 MONTHS AGE 12-14 RULE OUT SYSTEMIC
MONTHS TUMOR FIRST CAUSE?
│ │ (CT/MRI if (Wegener's,
▼ ▼ mass above sarcoidosis,
CONSERVATIVE PROBING medial lymphoma)
MANAGEMENT (single canthal │
• Lacrimal sac probe tendon) ▼
massage curative TREAT UNDERLYING
4-6x daily in ~90%) CONDITION FIRST
• Topical antibiotics │
(fluoroquinolone QID) │
• Wait for spontaneous │
resolution │
(~80-90% resolve │
by 12 months) │
│ │
▼ │
IF NOT RESOLVED │
by 12-14 months: │
Refer for probing │
± irrigation │
│ │
└──────────┬──────────────┘
│
▼
IF PROBING FAILS or ADULT WITH CONFIRMED NLDO
│
▼
┌──────────────────────────────────────┐
│ DACRYOCYSTORHINOSTOMY (DCR) │
│ (DEFINITIVE SURGICAL TREATMENT) │
└──────────────────────────────────────┘
│
┌──────────┴─────────┐
▼ ▼
EXTERNAL DCR ENDOSCOPIC DCR
(Traditional (Endonasal approach
skin incision) - no external scar)
│ │
└──────────┬─────────┘
│
▼
± SILICONE TUBE INTUBATION
(Bicanalicular tube placed to stent
the new opening; removed after 3-6 months)
│
▼
POST-DCR CARE:
• Topical antibiotics + steroids post-op
• Nasal decongestants to reduce swelling
• Avoid nose blowing for 2 weeks
• Silicone tube removal at 3-6 months
• Follow-up to confirm patency
│
▼
IF DCR FAILS (Recurrent symptoms):
→ REVISION DCR
→ Investigate for dacryolith, canalicular
stenosis, or tumor
→ Consider Jones tube (bypass procedure)
7. DACRYOCYSTORHINOSTOMY (DCR) - Explained Simply
- DCR = Dacryocysto-Rhino-Stomy
- "Dacryocysto" = lacrimal sac | "Rhino" = nose | "Stomy" = new opening
- A new drainage hole is made directly between the lacrimal sac and the nose, bypassing the blocked nasolacrimal duct
| Feature | External DCR | Endoscopic DCR |
|---|---|---|
| Approach | Small incision on skin near inner canthus | Through the nose - no skin cut |
| Scar | Small scar (usually hides well) | No external scar |
| Success rate | ~90-95% | ~85-90% |
| Preferred when | Lacrimal sac tumor suspected, revision cases | Cosmetically sensitive patients |
| Recovery | 2-3 weeks | Slightly faster |
- Tears can now bypass the blocked duct and drain directly into the nasal cavity
- Eliminates the stagnant pool of tears/mucus in the lacrimal sac
- Cures epiphora, mucocele, and recurrent conjunctivitis
8. MEDICAL TREATMENT SUMMARY TABLE
| Situation | Treatment | Notes |
|---|---|---|
| Infant, age < 12 months | Lacrimal massage + topical fluoroquinolone drops | 80-90% resolve spontaneously |
| Infant, not resolved by 12-14 months | Probing ± irrigation | Single probe curative in ~90% if done before 14 months |
| Recurrent conjunctivitis episodes | Topical fluoroquinolone (ciprofloxacin/ofloxacin) QID | Short courses; not curative |
| Mucocele / confirmed NLDO in adults | Refer for DCR | Definitive treatment |
| Recurrent acute flares | Short course oral antibiotics + DCR planning | Amoxicillin/clavulanate or cephalexin |
| Pre-intraocular surgery | DCR FIRST before any eye operation | Prevents endophthalmitis |
| Failed first DCR | Revision DCR or Jones tube | Rule out dacryolith or tumor |
Quick Memory Summary
CHRONIC DACRYOCYSTITIS = PAINLESS WATERY EYE + MUCUS ON PRESSURE
↓
CONSERVATIVE (massage, drops) = temporary only
↓
DEFINITIVE CURE = DCR (new hole into nose)
- Kanski's Clinical Ophthalmology, 10th ed., pp. 124-125
- Wills Eye Manual, 7th ed., pp. 399-402
- Cummings Otolaryngology: Head and Neck Surgery (Endoscopic DCR chapter, p. 965)
- Textbook of Family Medicine, 9th ed., p. 350
Dacrocystorhinostomy ( Dcr) Its indication, contraindications, type of anaesthesia used, major surgical steps, post operative care , complications and their management in brief ( with respect of chronic DACROCYTITIS surgery)
Dacryocystorhinostomy (DCR) - Complete Surgical Guide
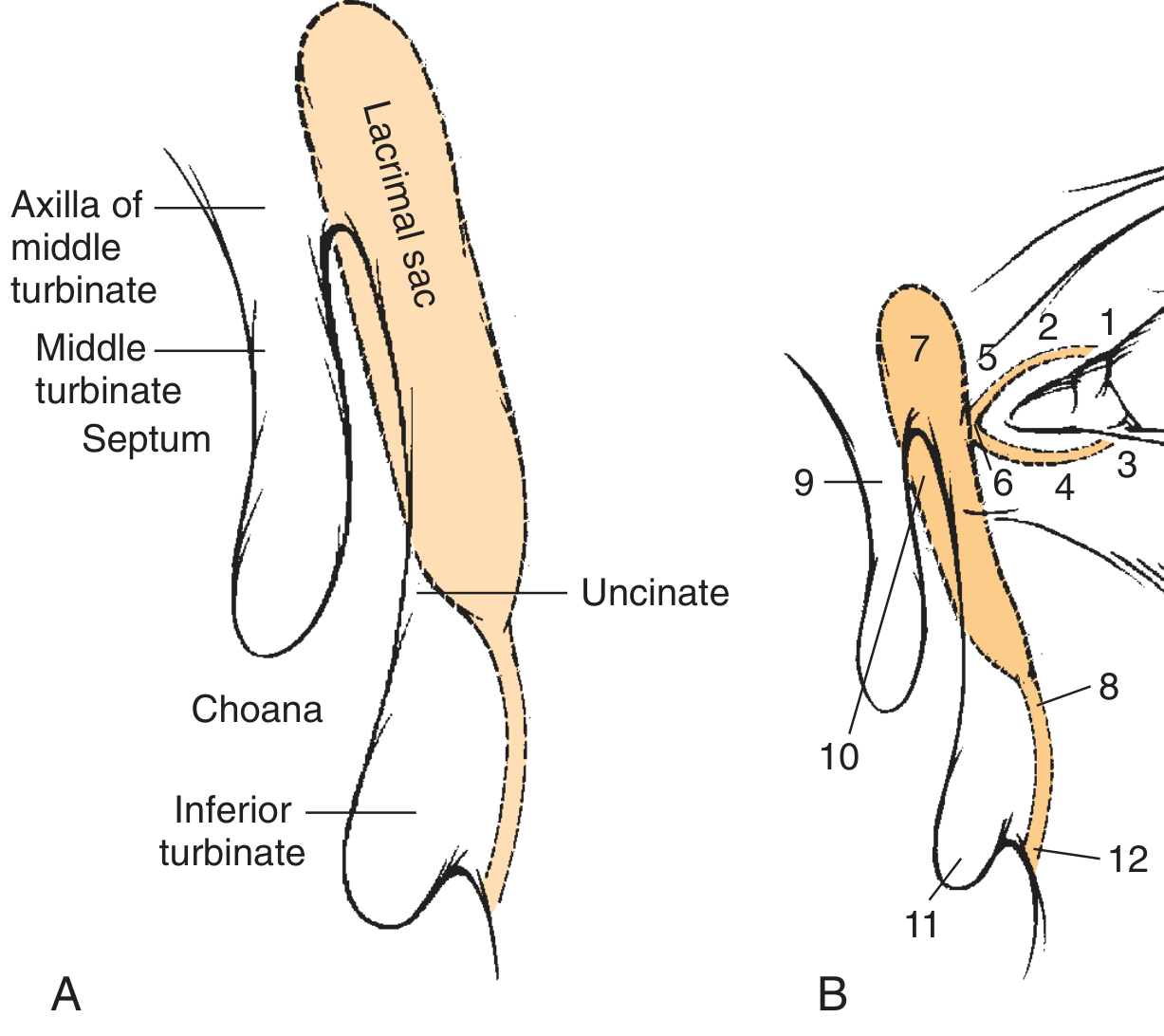
Anatomy Relevant to DCR
1. INDICATIONS
Primary Indications (Do DCR for these)
- Chronic dacryocystitis with confirmed nasolacrimal duct obstruction (NLDO) - the main indication
- Recurrent acute dacryocystitis - to prevent further episodes
- Mucocele of the lacrimal sac
- Symptomatic epiphora (persistent watering eye) due to NLDO causing significant distress
- Lacrimal sac fistula - DCR closes the fistula by restoring normal drainage
- Dacryolithiasis (lacrimal stones) with obstruction
- Before planned intraocular surgery (e.g., cataract) when chronic dacryocystitis/NLDO is present - to prevent endophthalmitis
- Failed probing in children (after second probing failure)
- Post-traumatic NLDO - after nasal/facial fractures
- Iatrogenic NLDO - after nasal/sinus surgery
2. CONTRAINDICATIONS
Absolute Contraindications
- Active acute dacryocystitis - infection must be fully treated first with antibiotics before any surgery
- Lacrimal sac tumor - DCR alone is not appropriate; requires tumor excision
- Bleeding disorders not corrected preoperatively
- Obstruction proximal to common canaliculus (canalicular block) - DCR bypasses the duct but not a canalicular blockage; requires canaliculoplasty or Jones tube instead
Relative Contraindications
- Nasal pathology - severe septal deviation, polyps, or active rhinitis may complicate surgery (septal correction may be done at same time)
- Previous DCR failure with scarred sac - small scarred residual sac may limit marsupialization; outcomes compromised
- Systemic conditions - uncontrolled diabetes, anticoagulant therapy, severe hypertension (must be optimized before surgery)
- Wegener's granulomatosis, sarcoidosis - underlying disease must be controlled first
- Medial canthal tumor above the medial canthal tendon - suspect lacrimal sac neoplasm; biopsy first
3. TYPE OF ANAESTHESIA
External DCR
| Patient Group | Anaesthesia Used |
|---|---|
| Adults (most cases) | Local anaesthesia + sedation (preferred) |
| Anxious patients / children | General anaesthesia |
| Complex revision cases | General anaesthesia |
- Infiltration: 1% lidocaine with 1:100,000 epinephrine injected at the medial canthal area and around the lacrimal sac
- Nerve blocks: Infratrochlear nerve block and anterior ethmoidal nerve block
- Nasal packing: Ribbon gauze soaked in 4% cocaine or xylometazoline + lidocaine placed in nasal cavity for mucosal vasoconstriction and anaesthesia
- Advantage of LA: Avoids general anaesthesia risks; patient can cooperate; better vasoconstriction
Endoscopic DCR
- General anaesthesia is standard and preferred
- Controlled hypotension is used intraoperatively (reduces cardiac output to minimize bleeding)
- Local injections (1% lidocaine with 1:100,000 epinephrine) into nasal mucosa supplemented
- Head elevated 30 degrees to reduce venous congestion
- Topical vasoconstrictors (1:1000 epinephrine neuropatties) placed periodically during surgery
4. MAJOR SURGICAL STEPS
A. EXTERNAL DCR (Traditional Open Approach)
STEP 1: SKIN INCISION
• Curvilinear incision ~11mm long, 2-3mm medial to inner canthus
• Incision over lacrimal sac area, parallel to medial orbital rim
• Avoids angular vessels and medial canthal tendon
STEP 2: DISSECTION TO LACRIMAL SAC
• Divide orbicularis oculi muscle
• Retract medial canthal tendon (may be reflected or cut and repaired)
• Expose the periosteum of the lacrimal fossa
STEP 3: LACRIMAL SAC EXPOSURE
• Incise periosteum along lacrimal fossa
• Elevate periosteum with Freer elevator
• Expose the lacrimal sac in the lacrimal fossa
STEP 4: OSTEOTOMY (Bone Removal)
• Create a bony window in the medial wall of lacrimal fossa
• Remove the lacrimal bone and frontal process of maxilla
using bone punch (Kerrison punch) or hammer and gouge
• Window size: ~15mm x 15mm (minimum)
• Expose the nasal mucosa beneath
STEP 5: NASAL MUCOSAL FLAPS
• Incise the nasal mucosa to create anterior and posterior flaps
STEP 6: LACRIMAL SAC OPENING
• Dilate the punctum with punctum dilator
• Pass Bowman probe through canaliculus to tent the sac
• Incise the lacrimal sac vertically to create anterior (H-flap)
and posterior flaps
STEP 7: ANASTOMOSIS (Flap Suturing)
• Suture posterior flap of lacrimal sac to posterior nasal mucosal flap
(2-3 absorbable sutures, e.g., 5-0 Vicryl)
• Anterior flap anastomosis performed similarly
• This creates the new drainage ostium
STEP 8: SILICONE INTUBATION (if needed)
• Pass silicone bicanalicular tube (O'Donoghue tubes) through
superior and inferior canaliculi into the new opening
• Secure in nasal cavity without tension (prevents cheese-wiring)
• Left in for 3-6 months (up to 9 months if canalicular stenosis)
STEP 9: WOUND CLOSURE
• Close periosteum and orbicularis muscle in layers
• Skin closed with interrupted 6-0 nylon or absorbable sutures
• Light pressure dressing applied
B. ENDOSCOPIC DCR (Endonasal Approach - No External Scar)
STEP 1: PREPARATION
• Patient under GA, head raised 30°, controlled hypotension
• 4% cocaine/xylometazoline nasal packing for decongestion
• 1% lidocaine + epinephrine injected into nasal mucosa
• Septoplasty performed if septum obstructs visualization (~50% cases)
STEP 2: MUCOSAL FLAP ELEVATION
• 30° endoscope introduced into nasal cavity
• Posteriorly pedicled mucoperiosteal flap raised using
No.15 blade + Freer elevator
• Flap elevated from lacrimal bone up to axilla of middle turbinate
STEP 3: BONE REMOVAL (Critical step)
• Frontal process of maxilla removed with forward-biting bone
punch (Hajek-Koeffler or Kerrison rongeur)
• DCR drill bit used to "saucerize" remaining bone
• Entire lacrimal sac must be exposed - it should sit
"proud" (protruding) over saucerized bone
• Posterior lacrimal bone removed with round knife
STEP 4: CANNULATION
• Punctum dilated; Bowman probe (size 00) passed through
inferior canaliculus into lacrimal sac
• Probe tip must be clearly VISIBLE tenting the medial sac wall
(if entire sac moves without tip visible = probe in canaliculus, NOT sac)
STEP 5: MARSUPIALIZATION (Opening the sac)
• Spear knife used to incise sac vertically top to bottom
• Anterior and posterior sac flaps created and laid flat
• Flaps should lie open without tension - confirms adequate bone removal
STEP 6: FLAP REINSERTION
• Nasal mucosal flap trimmed to fit opened lacrimal sac
• Flaps apposed to provide mucosal-to-mucosal healing
• Minimizes granulation tissue formation
STEP 7: SILICONE INTUBATION (if canalicular stenosis)
• O'Donoghue tubes passed if common canaliculus is tight
• Secured with GelFoam + silicone tubing + titanium clips
• Left in situ 4-6 weeks (or 6-9 months if canalicular stenosis)
STEP 8: NASAL PACK
• Light absorbable nasal pack or gel foam placed
• Standard nasal pack removed at 24-48 hours
5. COMPARISON: EXTERNAL vs. ENDOSCOPIC DCR
| Feature | External DCR | Endoscopic DCR |
|---|---|---|
| Approach | Skin incision at medial canthus | Through the nose, no incision |
| Scar | Small skin scar (fades well) | No external scar |
| Anaesthesia | LA + sedation (usually) | GA (usually) |
| Success rate (5-year) | ~94% | ~92% |
| Immediate success | 65-100% | 84-94% |
| Tumour biopsy possible | Yes - excellent | Limited |
| Learning curve | Shorter | Longer (needs rhinology skills) |
| Concomitant nasal surgery | Difficult | Easy - can fix septum/polyps simultaneously |
| Lacrimal pump preserved | Yes | Yes |
| Laser DCR (variant) | - | ~38% at 5 years (inferior) |
6. POST-OPERATIVE CARE
Immediate (Day 0-1)
- Ice pack to medial canthal area - reduces swelling and bruising
- Nasal pack removal at 24-48 hours (if non-absorbable pack used)
- Head elevated 30-45 degrees - reduces oedema
- Observe for bleeding - nasal bleeding is the most common early complication
Medications (Post-op Routine)
- Topical antibiotic-steroid drops (e.g., chloramphenicol + dexamethasone) 4 times daily for 2-4 weeks - reduces infection and scarring
- Nasal decongestant drops/spray (e.g., xylometazoline) twice daily for 1-2 weeks - reduces mucosal oedema around new ostium
- Oral antibiotics - broad spectrum for 5-7 days (e.g., amoxicillin/clavulanate or cephalexin)
- Oral analgesics (paracetamol/ibuprofen) for pain
- Topical nasal steroid spray after 2 weeks - reduces scarring and synechiae
Activity Restrictions
- No nose blowing for 2 weeks - risk of surgical emphysema, dislodging clots
- Avoid swimming for 2-4 weeks
- Avoid heavy lifting and strenuous activity for 2 weeks
- Sleep with head elevated for 1-2 weeks
Silicone Tube Care
- Check tubes are in correct position at first follow-up
- Tubes removed at 3-6 months (up to 9 months if canalicular stenosis was present)
- Tube removal is a quick, painless outpatient procedure
- Instruct patient: if tube extrudes prematurely, do NOT pull - seek review urgently
Follow-Up Schedule
- 1 week - check wound healing, skin suture removal (external DCR), assess bleeding
- 4-6 weeks - nasal endoscopy to check ostium patency, remove crusts/synechiae
- 3-6 months - silicone tube removal + lacrimal irrigation to confirm patency
- 6-12 months - final assessment; fluorescein dye disappearance test
7. COMPLICATIONS AND MANAGEMENT
INTRAOPERATIVE COMPLICATIONS
| Complication | Cause | Management |
|---|---|---|
| Haemorrhage | Angular artery/vein injury, ethmoidal artery | Bipolar cautery; nasal packing; controlled hypotension |
| Canalicular damage | Incorrect probe placement; knife slip | Repair with fine sutures; silicone intubation |
| Medial canthal tendon injury | Careless dissection | Re-attach and repair with sutures |
| Orbital fat prolapse | Periorbital fat herniation | Gentle reduction; avoid entry into orbit |
| CSF leak | Very rare; drilling too superiorly | Stop surgery; neurosurgical consult |
| Nasal septal perforation | Endoscopic septal injury | Repair primarily or later |
EARLY POST-OPERATIVE COMPLICATIONS (Days-Weeks)
| Complication | Features | Management |
|---|---|---|
| Post-op bleeding | Most common early complication; nasal bleed | Ice pack; nasal packing; if severe - return to theatre |
| Wound infection | Redness, discharge at skin incision | Oral antibiotics; wound care |
| Skin suture granuloma | Small nodule at incision | Remove suture; resolves spontaneously |
| Silicone tube extrusion | Tube slips out of punctum | Urgent repositioning or removal |
| Cheese-wiring | Tube cuts through punctum if too tight | Reposition tube tension-free; punctoplasty if needed |
| Nasal synechiae | Adhesions in nasal cavity occluding ostium | Endoscopic lysis under LA at 4-6 week review |
LATE / LONG-TERM COMPLICATIONS
| Complication | Features | Management |
|---|---|---|
| DCR failure (most important) | Recurrence of epiphora/discharge | See revision DCR below |
| Ostium closure (fibrosis) | New opening scars shut | Most common reason for DCR failure |
| Persistent fistula | Pre-existing sac-skin fistula doesn't close | Revision DCR; fistula excision |
| Visible scar | External DCR scar at medial canthus | Usually fades; Z-plasty if problematic |
| Medial canthal webbing | Scarring causes skin band at inner canthus | Z-plasty revision |
| Lacrimal pump failure | Orbicularis weakness; epiphora without obstruction | Cannot correct with DCR; Jones tube may help |
| Recurrent granuloma | Intranasal granulation tissue occludes ostium | Endoscopic debridement + nasal steroids |
| Canalicular stenosis | Common canaliculus narrows post-op | Silicone intubation; canaliculoplasty |
REVISION DCR - When and How
- Symptomatic recurrence after initially successful DCR
- Failed primary DCR (persistent epiphora from day 1)
- Review original DCG to assess residual sac size
- Nasal endoscopy to identify cause of failure (ostium closed, scarred, granuloma)
- If sac tissue is adequate - revision with wider marsupialization
- If sac is small/scarred - outcomes are poorer; tailored nasal flap approach
- Jones tube (bypass tube) - if canalicular system is also compromised; glass tube inserted from medial canthus directly into nose, bypassing entire lacrimal system
8. SUCCESS RATES SUMMARY
| Procedure | Immediate Success | 5-Year Success |
|---|---|---|
| Endoscopic DCR | 84-94% | 92% |
| External DCR | 65-100% | 94% |
| Laser-assisted DCR | 47-100% | 38% (inferior) |
| Revision DCR | ~80% (if adequate sac) | Variable |
Anatomic obstruction (like chronic dacryocystitis/NLDO) achieves 95-97% success with proper technique. Functional obstruction has similar anatomical success but only ~81% are symptom-free (lacrimal pump anomalies persist).
QUICK SURGERY SUMMARY FLOWCHART
CHRONIC DACRYOCYSTITIS WITH CONFIRMED NLDO
↓
Treat any active infection first
↓
Pre-op workup: DCG, nasal endoscopy,
Jones tests, CT if needed
↓
Choose approach:
┌──────────────┬────────────────────┐
│ External DCR │ Endoscopic DCR │
│ (LA/sedation)│ (GA preferred) │
└──────────────┴────────────────────┘
↓
Surgery: Bone removal → Sac exposure
→ Open sac → Anastomose to nasal mucosa
→ Silicone tube if needed
↓
Post-op: Antibiotic-steroid drops +
nasal decongestant + no nose blowing
↓
Follow-up: Tube removal at 3-6 months
↓
Check patency: Irrigation + fluorescein test
↓
SUCCESS (~92-97%) or REVISION DCR
- Cummings Otolaryngology: Head and Neck Surgery, 7th ed. (Chapter 49 - Endoscopic DCR, pp. 964-970)
- Kanski's Clinical Ophthalmology, 10th ed., pp. 124-125
- Wills Eye Manual, 7th ed., pp. 399-402
Dacrocystectomy ( Dct) Its indication, contraindications, type of anaesthesia used, major surgical steps, post operative care , complications and their management in brief ( with respect of chronic DACROCYTITIS surgery
dacryocystectomy surgical steps indications complications chronic dacryocystitis lacrimal sac excision
https://openophthalmologyjournal.com/VOLUME/14/PAGE/25/FULLT…
https://emedicine.medscape.com/article/1210688-treatment
Dacryocystectomy (DCT) - Complete Surgical Guide
What is Dacryocystectomy?
Key difference from DCR: DCR bypasses the blocked duct and preserves the sac to create a new drainage path. DCT removes the sac entirely. After DCT, there is no lacrimal sac - tears still drain partly through canalicular capillary action and evaporation, and epiphora (watering) may persist to a variable degree.
1. INDICATIONS
Primary Indication
- Lacrimal sac tumor (neoplasm) - the most important and classic indication; complete sac excision with histopathology is required
Indications Specific to Chronic Dacryocystitis
- Recurrent dacryocystitis - more than 2 episodes in 6 months or more than 3 in one year, especially when DCR is not feasible
- Chronic dacryocystitis with failed or refused DCR - patients unfit or unwilling for DCR
- Frail elderly patients (75 years and older) with high anaesthetic/bleeding risk who cannot tolerate DCR
- Patients on long-term anticoagulant therapy where DCR carries high haemorrhagic risk
- Chronic discharging lacrimal sac fistula - fistulous tract and sac excised together
- Lacrimal sac mucocele that is large, expanding, or secondarily infected and unfit for DCR
- Nasal or facial malformations that make intranasal access for DCR technically impossible (e.g., severe septal deformity, absent nasal anatomy)
- Risk of post-DCR nasocutaneous fistula (e.g., in irradiated tissue)
- Wegener's granulomatosis / vasculitis with NLDO - DCR fails due to disease recurrence; DCT removes the infected sac
- NLDO with dry eye, ocular cicatricial pemphigoid, Crohn's disease, systemic lupus - DCT is a viable alternative when DCR is inadvisable
- Patients with recurrent dacryocystitis after failed DCR - DCT removes residual infected sac tissue
- Anxious or medically unfit patients unable to tolerate prolonged surgery in supine position
2. CONTRAINDICATIONS
Absolute Contraindications
- Active acute dacryocystitis - acute infection must be treated with antibiotics first; surgery only after infection settles
- Uncorrected bleeding diathesis (coagulation disorders not optimized)
- Unfit for any surgery due to extreme systemic illness
Relative Contraindications
- Bilateral NLDO - removing both lacrimal sacs leads to severe, permanent bilateral epiphora; consider DCR instead
- Young patients who desire tear drainage - DCT eliminates the lacrimal sac permanently; epiphora will persist; DCR is strongly preferred in younger patients
- Isolated canalicular block without sac disease - sac is healthy; no indication to excise it
- Patient preference for drainage restoration - DCT does NOT restore lacrimal drainage; patients must be counselled that watering may continue
- Lacrimal sac tumor with orbital extension - DCT alone is not sufficient; orbital exenteration may be required
3. PRE-OPERATIVE ASSESSMENT
- Full history and slit-lamp examination
- Dacryocystography (DCG) or CT scan to assess sac anatomy
- Rule out lacrimal sac tumor - note if mass is above medial canthal tendon
- Routine bloods: CBC, coagulation profile, blood glucose
- Stop anticoagulants as per protocol (discuss with physician)
- Consent patient: inform that epiphora will likely persist as no new drainage pathway is created; also discuss scar
4. TYPE OF ANAESTHESIA
Standard for Most Cases
- Shorter procedure than DCR, so LA is well tolerated
- Especially preferred in elderly/frail patients (main target group for DCT)
Local Anaesthesia Technique
- Infiltration anaesthesia:
- 1-2 mL of 2% lidocaine with 1:100,000 adrenaline (epinephrine) injected into the medial canthal area, over the lacrimal sac, and along the planned incision line
- Adrenaline provides vasoconstriction, reducing bleeding
- Nerve blocks:
- Infratrochlear nerve block (superomedial orbital rim)
- Anterior ethmoidal nerve block if needed
- No nasal packing needed (unlike DCR - the nasal cavity is NOT entered during DCT)
General Anaesthesia - Used when:
- Patient request / high anxiety
- Children
- Planned additional procedures simultaneously
- Suspected lacrimal sac tumor (wider dissection may be needed)
5. MAJOR SURGICAL STEPS
PRE-OPERATIVE SETUP
• Patient supine, head slightly elevated
• Skin prepped and draped
• Puncta dilated with punctum dilator
• LA infiltrated as described above
• Monitor vital signs throughout (especially in elderly)
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
STEP 1: SKIN INCISION
• Curvilinear incision approximately 10-15 mm long
• Placed 2-3 mm medial to the inner canthus
(same position as external DCR incision)
• Direction: parallel to medial orbital rim
• Depth: through skin and subcutaneous tissue only
• AVOID: angular vessels (lie 8mm medial to inner canthus)
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
STEP 2: DISSECTION TO LACRIMAL SAC
• Divide orbicularis oculi muscle in line with the incision
• Identify and protect the angular vessels
(ligate or cauterise if encountered)
• Incise and reflect the periosteum (periorbita)
over the anterior lacrimal crest
• Expose the lacrimal sac lying in the lacrimal fossa
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
STEP 3: CANALICULAR IDENTIFICATION
• Pass a Bowman probe (size 0 or 00) through the
inferior or superior canaliculus into the lacrimal sac
• This tents the medial wall of the sac and helps identify it
• The probe also guides safe canalicular division
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
STEP 4: LACRIMAL SAC DISSECTION
• Using fine scissors (Westcott or Stevens tenotomy scissors)
and fine-toothed forceps, carefully dissect the lacrimal sac
free from its attachments on all sides
• Dissect medially (lacrimal fossa bone), laterally
(periorbita), superiorly (fundus of sac), and inferiorly
(neck of sac at nasolacrimal duct junction)
• Keep dissection close to sac wall to protect periorbita
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
STEP 5: DIVISION OF CANALICULI
• Divide the common canaliculus (or superior and inferior
canaliculi separately if they enter separately) as close
to the sac as possible
• Preserve maximum canalicular length for patient comfort
and possible future Jones tube if needed
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
STEP 6: DIVISION OF NASOLACRIMAL DUCT
• At the inferior end of the sac (neck), divide and
ligate / cauterise the nasolacrimal duct stump
• The nasal mucosa is NOT opened (this is the
critical difference from DCR - nasal cavity not entered)
• Haemostasis secured with bipolar cautery
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
STEP 7: COMPLETE SAC EXCISION
• Entire lacrimal sac is now completely freed and excised
• The sac is removed as a single specimen
• If tumor suspected: send for FROZEN SECTION
and HISTOPATHOLOGY (routine in all cases)
• If fistula present: excise the fistulous tract in continuity
with the sac (en bloc excision)
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
STEP 8: HAEMOSTASIS AND DEAD SPACE
• Thorough haemostasis with bipolar cautery
• Bone wax applied to exposed lacrimal fossa bone edge
if oozing
• Dead space obliterated by approximating soft tissues
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
STEP 9: OPTIONAL - SILICONE TUBE INTUBATION
• In selected cases (recurrent dacryocystitis + epiphora),
permanent silicone intubation of residual canaliculi
can be performed (as per recent DCT + intubation technique)
• This provides some residual drainage via the canaliculi
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
STEP 10: WOUND CLOSURE
• Periosteum closed with 5-0 absorbable suture (Vicryl)
• Orbicularis muscle closed with interrupted 5-0 Vicryl
• Skin closed with interrupted 6-0 nylon or fast-absorbing
Vicryl sutures
• Light pressure dressing applied
• Total operative time: approximately 20-45 minutes
(shorter than DCR)
6. COMPARISON: DCT vs. DCR
| Feature | Dacryocystectomy (DCT) | Dacryocystorhinostomy (DCR) |
|---|---|---|
| What is done | Sac REMOVED | Sac preserved, new nasal opening created |
| Epiphora after surgery | Persists (to variable degree) | Resolved in ~92-97% |
| Nasal cavity entered | NO | YES |
| Surgery time | Shorter (~30 min) | Longer (~60-90 min) |
| Preferred anaesthesia | LA + sedation | GA (endoscopic) or LA (external) |
| Best for | Frail/elderly, tumor, failed DCR | Younger patients, active drainage desired |
| Scar | Small medial canthal scar | Same scar (external) or no scar (endoscopic) |
| Risk of haemorrhage | Lower (no bony work, no nasal entry) | Higher |
7. POST-OPERATIVE CARE
Immediate (Day 0-1)
- Pressure dressing over the medial canthal area - reduces haematoma and oedema; removed at 24-48 hours
- Ice pack applied intermittently for first 24 hours - reduces swelling and bruising
- Observe for bleeding - most common early complication
- Head elevated 30-45 degrees when resting
Medications
- Topical antibiotic eye drops (e.g., chloramphenicol 0.5% or moxifloxacin) 4 times daily for 1-2 weeks
- Topical antibiotic-steroid ointment on wound (e.g., chloramphenicol ointment) to prevent infection and reduce scarring
- Oral antibiotics for 5-7 days (e.g., cefalexin 500mg QID or amoxicillin/clavulanate 625mg BD) - especially important in infected/chronic cases
- Oral analgesics - paracetamol ± ibuprofen for pain (usually mild)
- No nasal decongestants needed (nasal cavity not entered, unlike DCR)
Activity and Wound Care
- Keep wound dry for 48 hours
- No nose blowing vigorously for 1-2 weeks (prevents subcutaneous emphysema)
- No swimming for 2 weeks
- Skin suture removal at 5-7 days (if non-absorbable sutures used)
- Avoid heavy lifting for 1-2 weeks
Histopathology
- Review histopathology result at first follow-up (1 week) - MANDATORY to exclude tumor
Follow-Up Schedule
- 1 week - wound check, suture removal, histopathology review
- 4-6 weeks - assess healing, residual epiphora level
- 3 months - long-term review; counsel patient regarding persistent epiphora
- If silicone tube placed - review tube position at 6 months
8. COMPLICATIONS AND MANAGEMENT
INTRAOPERATIVE COMPLICATIONS
| Complication | Details | Management |
|---|---|---|
| Haemorrhage (most common) | Angular artery or vein injury; vessels lie close to incision | Identify and ligate/bipolar cauterise angular vessels; pressure; bone wax on bony edges |
| Periorbita (orbital septum) violation | Accidental entry into orbital fat | Avoid excessive dissection; gentle technique; close periorbita immediately |
| Orbital haematoma | Bleeding into orbital space (rare) | Immediate wound decompression; lateral canthotomy if vision threatened |
| Canalicular damage | Over-zealous dissection of the canaliculi | Preserve as much canaliculus as possible; silicone intubation to maintain patency |
| Incomplete sac excision | Small remnant of sac wall left behind | Will lead to recurrent dacryocystitis; careful dissection close to sac wall |
| Nasal mucosal entry | Accidental opening of nasal cavity | Pack with absorbable material; monitor for fistula |
EARLY POST-OPERATIVE COMPLICATIONS (Days-Weeks)
| Complication | Features | Management |
|---|---|---|
| Wound haematoma | Swelling, bruising at incision site | Pressure bandage; aspiration if large; observation usually sufficient |
| Wound infection | Erythema, discharge, pain at incision | Oral antibiotics; wound swab and culture; drainage if abscess forms |
| Wound dehiscence | Skin edges separate | Re-suture; wound care |
| Preseptal cellulitis | Surrounding eyelid infection | Oral or IV antibiotics |
| Orbital cellulitis (rare) | Proptosis, restricted eye movement, pain | Immediate IV antibiotics; CT scan; ophthalmology review |
LATE / LONG-TERM COMPLICATIONS
| Complication | Features | Management |
|---|---|---|
| Persistent epiphora | Most common long-term issue - expected after DCT as no drainage restored | Counsel patient preoperatively; lubricant drops for ocular surface; Jones tube if intolerable |
| Recurrent dacryocystitis | If sac excision was INCOMPLETE; residual sac re-infects | Revision surgery to remove residual sac tissue |
| Skin scar / keloid | Medial canthal scar becomes hypertrophic | Steroid injections (triamcinolone); Z-plasty revision; silicone gel sheets |
| Medial canthal webbing | Skin tethering at inner canthus | Z-plasty revision surgery |
| Visual loss (very rare) | Orbital haematoma compressing optic nerve | Lateral canthotomy + cantholysis; emergency orbital decompression if needed |
| Pyogenic granuloma | Granulation tissue at wound site | Topical steroids; excision if persistent |
| Nasocutaneous fistula | If nasal cavity inadvertently entered during surgery | Conservative management; revision surgery if persistent |
| Facial scar / cheloid | Visible scar at inner canthus | Steroid injections; scar revision |
9. OUTCOME AND PATIENT COUNSELLING
What to tell patients BEFORE DCT:
- Epiphora (watering eye) will persist after surgery - this is expected and permanent, because no new drainage pathway is created. Patients must clearly understand this before consenting.
- Surgery aims to cure recurrent infection and discharge - NOT to cure watering
- Small scar will be present at the medial canthal area (same as DCR scar)
- If epiphora is severe and intolerable after recovery, a Jones tube (glass bypass tube) can be considered as a salvage procedure
Success of DCT in Chronic Dacryocystitis:
- Excellent at eliminating recurrent infection (primary goal)
- Epiphora reduction: satisfactory in most patients (tear drainage partly maintained through canalicular capillary action and evaporation)
- Overall well-tolerated, especially in elderly/frail patients
- Complication rate lower than DCR in high-risk patients
10. DCT TREATMENT ALGORITHM (CHRONIC DACRYOCYSTITIS CONTEXT)
CHRONIC DACRYOCYSTITIS
│
▼
IS DCR FEASIBLE AND APPROPRIATE?
│
┌────┴──────────────┐
│ YES │ NO (any of below)
▼ ▼
DO DCR CONSIDER DCT IF:
(preferred) • Lacrimal sac TUMOR
• Frail/elderly (>75 yrs), high surgical risk
• On anticoagulants, high bleeding risk
• Recurrent dacryocystitis (>2/6mths) post-DCR
• Nasal malformation preventing DCR
• Wegener's/vasculitis with NLDO
• Chronic skin fistula
• Patient refuses DCR
│
▼
TREAT ACTIVE INFECTION FIRST
(Antibiotics until infection settles)
│
▼
PRE-OP WORKUP
(CT/DCG, bloods, consent)
│
▼
ANAESTHESIA: LA + sedation
(GA for frail/anxious/tumor cases)
│
▼
DCT SURGERY:
Incision → Expose sac →
Identify canaliculi →
Dissect sac free →
Divide canaliculi + duct →
Excise sac completely →
Send for histopathology →
± Silicone intubation →
Close wound
│
▼
POST-OP CARE:
Pressure dressing + antibiotics
+ topical drops + wound care
│
▼
FOLLOW-UP AT 1 WEEK:
Check wound + review histopathology
│
┌──────────┴──────────┐
▼ ▼
TUMOR on BENIGN chronic
histology dacryocystitis
│ │
▼ ▼
ONCOLOGY Monitor epiphora
REFERRAL If intolerable:
(Wide excision / → Consider Jones tube
radiotherapy)
- Open Ophthalmology Journal: Dacryocystectomy with Lacrimal Silicone Intubation in Challenging Patients (Vol.14, p.25)
- Dacryocystectomy as treatment of chronic dacryocystitis in frail elderly patients - Nature Eye Journal
- eMedscape: Dacryocystitis Treatment & Management
- Kanski's Clinical Ophthalmology, 10th ed.
- Wills Eye Manual, 7th ed.