Endocrine pharmacology mbbs 2nd year
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have comprehensive content. Let me compile a thorough MBBS 2nd year endocrine pharmacology guide.
Endocrine Pharmacology - MBBS 2nd Year Complete Notes
Source: Katzung's Basic and Clinical Pharmacology, 16th Ed.; Goodman & Gilman's Pharmacological Basis of Therapeutics
Overview of Endocrine Pharmacology Topics (MBBS 2nd Year)
- Thyroid & Antithyroid Drugs
- Insulin & Oral Antidiabetic Drugs
- Glucocorticoids & Mineralocorticoids
- Sex Hormones & Oral Contraceptives
- Anterior Pituitary Hormones
UNIT 1: THYROID AND ANTITHYROID DRUGS
1.1 Thyroid Physiology (Quick Recap)
- The thyroid secretes T3 (triiodothyronine) and T4 (thyroxine). T4 contains 65% iodine; T3 contains 59% iodine.
- Daily iodide requirement: 150 mcg (200 mcg in pregnancy/lactation).
- T3 is the more active form; T4 is peripherally converted to T3 by deiodinase enzymes.
HPT Axis:
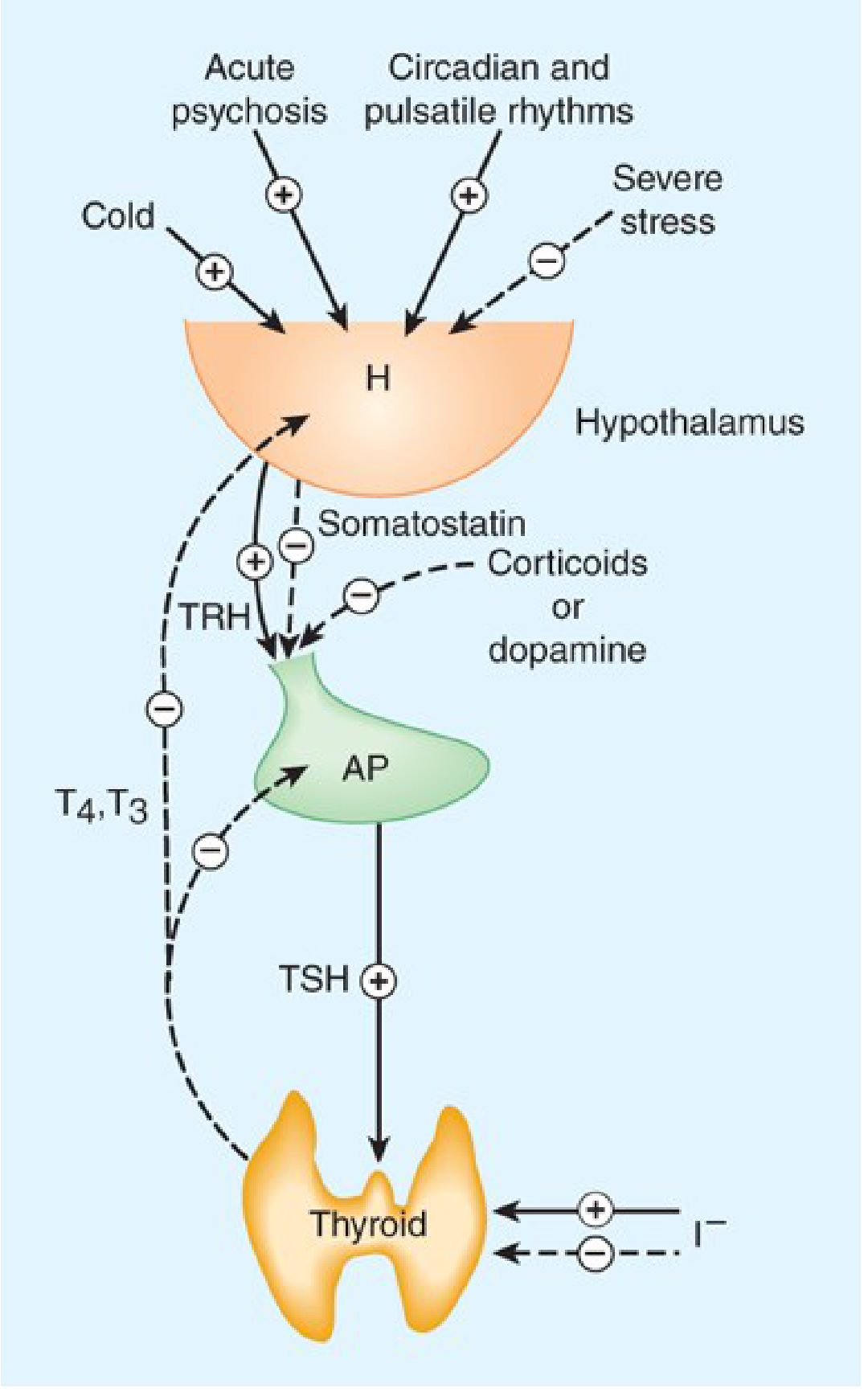
Hypothalamus secretes TRH → anterior pituitary releases TSH → thyroid produces T3/T4 → negative feedback inhibits TRH and TSH. Somatostatin and dopamine inhibit TSH release. Large doses of iodide (I⁻) inhibit T3/T4 production (Wolff-Chaikoff effect). (Katzung's Basic and Clinical Pharmacology, 16th Ed.)
Biosynthesis steps:
- Iodide trapping via NIS (sodium/iodide symporter) - inhibited by thiocyanate, perchlorate, pertechnetate
- Iodide transport to apical membrane via pendrin (SLC26A4)
- Oxidation by thyroid peroxidase (TPO) → iodine
- Organification - iodination of tyrosine residues on thyroglobulin → MIT, DIT
- Coupling - MIT + DIT → T3; DIT + DIT → T4
- Proteolysis → release of T3 and T4 into blood
1.2 Thyroid Hormone Preparations (Hypothyroidism Treatment)
| Drug | Type | Key Points |
|---|---|---|
| Levothyroxine (T4) | Synthetic T4 | Drug of choice; t½ = 7 days; dose = 1.7 mcg/kg/day; take on empty stomach 30-60 min before meals |
| Liothyronine (T3) | Synthetic T3 | Faster onset; t½ = 1-2 days; used in myxedema coma |
| Liotrix | T4:T3 = 4:1 | Combination preparation |
| Desiccated thyroid | Animal source | Contains both T3 & T4 |
Drug interactions with levothyroxine:
- Decreased absorption: Calcium carbonate, antacids, omeprazole, iron salts, cholestyramine (separate by 4 hours)
- Increased metabolism: Rifampicin, phenytoin, carbamazepine
Clinical note: TSH is the best monitoring test. Recheck after 6-8 weeks of dose change.
1.3 Antithyroid Drugs (Hyperthyroidism Treatment)
A. Thioamides (Thiocarbamides)
Drugs: Propylthiouracil (PTU) and Methimazole (Carbimazole is a prodrug → methimazole)
Mechanism of Action:
- Inhibit thyroid peroxidase (TPO) → block organification and iodine incorporation
- Block coupling of iodotyrosines (MIT+DIT → T3, DIT+DIT → T4)
- PTU only - also inhibits peripheral conversion of T4 → T3 (deiodination)
- Do NOT block iodide uptake
Onset: Slow - 3-4 weeks (depletes stored hormone; does not release stored T4/T3)
Methimazole advantages over PTU:
- Longer half-life → once-daily dosing
- Safer hepatic profile (PTU has black box warning for severe/fatal hepatitis)
- Preferred except in 1st trimester of pregnancy and thyroid storm
PTU preferred in:
- First trimester of pregnancy (methimazole teratogenic - aplasia cutis, choanal atresia)
- Thyroid storm (also blocks T4→T3 peripheral conversion)
Adverse Effects:
- Maculopapular pruritic rash (4-6%) - most common
- Nausea, GI distress
- Agranulocytosis (0.1-0.5%) - most dangerous; patient must stop drug immediately if sore throat/fever; cross-sensitivity ~50% between PTU and methimazole
- PTU: hepatotoxicity (black box warning - rare but fatal)
- Methimazole: cholestatic jaundice, altered taste/smell
- Rare: vasculitis, lupus-like reaction, exfoliative dermatitis
B. Iodides (High-Dose Iodine)
Preparations: Lugol's solution (5% iodine + 10% KI), SSKI (saturated solution of potassium iodide)
Mechanism:
- Inhibit organification (Wolff-Chaikoff effect)
- Inhibit hormone release
- Reduce vascularity and size of hyperplastic thyroid gland
Uses:
- Pre-operative preparation for thyroidectomy (given 10-14 days before surgery)
- Thyroid storm (given 1 hour AFTER thioamides to prevent organification of excess iodine)
- Radiation emergency (KI protects thyroid from radioactive iodine uptake)
- Jod-Basedow phenomenon: excess iodide → hyperthyroidism in susceptible patients (multinodular goiter)
C. Radioactive Iodine (¹³¹I)
- Emits beta rays (mainly) + gamma rays
- Taken up by thyroid → destroys follicular cells
- Treatment of choice for Graves' disease in non-pregnant adults
- Contraindicated in pregnancy and breastfeeding
- May worsen ophthalmopathy (15-20% risk, especially in smokers)
- Results in permanent hypothyroidism in most patients → needs levothyroxine replacement
D. Anion Inhibitors
- Perchlorate (ClO₄⁻), pertechnetate (TcO₄⁻), thiocyanate (SCN⁻)
- Competitively inhibit iodide transport (NIS)
- Potassium perchlorate used in amiodarone-induced hyperthyroidism
- Rarely used - risk of aplastic anemia
E. Beta-Blockers (Propranolol)
- Controls symptomatic relief of thyrotoxicosis (palpitations, tremor, anxiety, heat intolerance)
- Propranolol at high doses also inhibits peripheral T4 → T3 conversion
- Key role in thyroid storm management
1.4 Thyroid Storm Management
Thyroid storm is a life-threatening thyrotoxic crisis. Treatment (in order):
- Propranolol IV/oral - controls cardiovascular symptoms
- PTU (500-1000 mg loading dose, then 250 mg every 4h) - blocks synthesis AND peripheral conversion
- Iodide (SSKI/Lugol's) - given 1 hour AFTER PTU - blocks hormone release
- Hydrocortisone 50 mg IV every 6h - anti-shock + blocks T4→T3 conversion
UNIT 2: INSULIN & ANTIDIABETIC DRUGS
2.1 Insulin
Types based on duration of action:
| Type | Drug | Onset | Peak | Duration |
|---|---|---|---|---|
| Rapid-acting | Lispro, Aspart, Glulisine | 5-15 min | 1-2 h | 3-5 h |
| Short-acting | Regular insulin | 30-60 min | 2-4 h | 6-8 h |
| Intermediate | NPH (isophane) | 1-2 h | 6-10 h | 16-24 h |
| Long-acting | Glargine, Detemir | 1-4 h | None/flat | 20-24 h |
| Ultra-long | Degludec | 1-2 h | None | >42 h |
Mechanism: Binds insulin receptor (tyrosine kinase) → GLUT4 translocation to cell surface → glucose uptake in muscle/fat; inhibits gluconeogenesis and lipolysis in liver
Adverse Effects:
- Hypoglycemia (most important)
- Lipodystrophy at injection site (lipoatrophy or lipohypertrophy)
- Weight gain
- Hypokalemia (insulin drives K⁺ into cells)
Uses of insulin:
- Type 1 DM (mandatory)
- Type 2 DM (when oral agents fail)
- Diabetic ketoacidosis (regular insulin IV)
- Hyperkalemia (insulin + dextrose IV)
- Gestational diabetes
2.2 Oral Antidiabetic Drugs
A. Biguanides - Metformin
- MOA: Activates AMPK → inhibits hepatic gluconeogenesis; increases insulin sensitivity; does NOT cause hypoglycemia (anti-hyperglycemic)
- Drug of choice for Type 2 DM (especially overweight patients)
- No weight gain, may reduce weight; no hypoglycemia monotherapy
- ADRs: GI upset (most common), lactic acidosis (rare but serious - avoid in renal impairment, hepatic failure, hypoxia)
- Contraindications: eGFR <30, IV contrast studies (hold 48h)
B. Sulfonylureas
1st generation: Tolbutamide, Chlorpropamide
2nd generation: Glibenclamide (glyburide), Glipizide, Glimepiride
- MOA: Close ATP-sensitive K⁺ channels on β-cells → depolarization → Ca²⁺ influx → insulin secretion (require functional β-cells)
- ADRs: Hypoglycemia (main risk, especially with glibenclamide), weight gain
- Chlorpropamide: longest acting, antabuse-like reaction with alcohol, SIADH
C. Meglitinides (Glinides)
Drugs: Repaglinide, Nateglinide
- Similar MOA to sulfonylureas (K⁺ channel closure) but shorter-acting
- Taken before meals; control postprandial hyperglycemia
- Less hypoglycemia than sulfonylureas
D. Thiazolidinediones (Glitazones)
Drugs: Pioglitazone, Rosiglitazone
- MOA: Activate PPAR-γ nuclear receptor → improve insulin sensitivity in muscle, fat, liver
- ADRs: Weight gain, fluid retention/edema, heart failure (contraindicated in heart failure), fractures, bladder cancer risk (pioglitazone)
- Rosiglitazone: increased cardiovascular risk (withdrawn in many countries)
E. Alpha-Glucosidase Inhibitors
Drugs: Acarbose, Miglitol
- MOA: Inhibit intestinal alpha-glucosidase → delay carbohydrate digestion/absorption → reduce postprandial hyperglycemia
- ADRs: GI - flatulence, bloating, diarrhea (most common reason for discontinuation)
- No hypoglycemia monotherapy; if hypoglycemia occurs with combination therapy → treat with glucose (NOT sucrose)
F. DPP-4 Inhibitors (Gliptins)
Drugs: Sitagliptin, Vildagliptin, Saxagliptin, Alogliptin
- MOA: Inhibit dipeptidyl peptidase-4 → prevent GLP-1 degradation → increased insulin secretion (glucose-dependent) + decreased glucagon
- Weight-neutral; low hypoglycemia risk
- ADRs: Nasopharyngitis, urinary tract infections, rare pancreatitis
G. GLP-1 Receptor Agonists
Drugs: Exenatide, Liraglutide, Semaglutide, Dulaglutide
- MOA: Mimic GLP-1 → stimulate insulin secretion (glucose-dependent), suppress glucagon, slow gastric emptying, reduce appetite
- Weight loss benefit; cardiovascular benefit (liraglutide, semaglutide)
- ADRs: Nausea, vomiting (most common); rare pancreatitis; thyroid C-cell tumors in animals
- Given by subcutaneous injection (semaglutide also available orally)
H. SGLT-2 Inhibitors (Gliflozins)
Drugs: Dapagliflozin, Empagliflozin, Canagliflozin
- MOA: Inhibit SGLT-2 in proximal tubule → block glucose reabsorption → glycosuria
- Weight loss, BP reduction; cardiovascular and renal protection
- ADRs: Genital mycotic infections, UTI, polyuria; Euglycemic DKA (rare); Fournier's gangrene; do NOT use in eGFR <30
Summary Table: Oral Antidiabetics
| Drug Class | MOA | Hypoglycemia | Weight | Key ADR |
|---|---|---|---|---|
| Metformin | ↓ gluconeogenesis | No | ↓ | Lactic acidosis |
| Sulfonylureas | ↑ insulin secretion | Yes | ↑ | Hypoglycemia |
| Glitazones | PPAR-γ agonist | No | ↑↑ | Edema, fractures |
| Acarbose | ↓ CHO absorption | No | Neutral | Flatulence |
| DPP-4i | ↑ GLP-1 | No | Neutral | Nasopharyngitis |
| GLP-1 agonists | ↑ insulin, ↓ glucagon | No | ↓ | Nausea/vomiting |
| SGLT-2i | Glycosuria | No | ↓ | Genital infections |
UNIT 3: GLUCOCORTICOIDS & MINERALOCORTICOIDS
3.1 Glucocorticoids
Natural: Cortisol (hydrocortisone), Corticosterone
Synthetic: Prednisolone, Methylprednisolone, Dexamethasone, Betamethasone, Triamcinolone, Budesonide
Relative Potency Table:
| Drug | Glucocorticoid | Mineralocorticoid | Duration | Dose equiv. |
|---|---|---|---|---|
| Hydrocortisone | 1 | 1 | Short | 20 mg |
| Prednisolone | 4 | 0.8 | Intermediate | 5 mg |
| Methylprednisolone | 5 | 0.5 | Intermediate | 4 mg |
| Dexamethasone | 25-30 | 0 | Long | 0.75 mg |
| Betamethasone | 25-30 | 0 | Long | 0.6 mg |
| Fludrocortisone | 10 | 125-150 | - | (mineralocorticoid) |
Mechanism of Action:
- Diffuse through cell membrane → bind cytoplasmic glucocorticoid receptor (GR)
- GR-steroid complex → translocates to nucleus → binds GRE (glucocorticoid response elements) → gene transcription
- Anti-inflammatory: inhibit phospholipase A₂ (via lipocortin/annexin) → ↓ arachidonic acid → ↓ prostaglandins, leukotrienes
- Immunosuppressive: inhibit NF-κB, IL-1, IL-2, TNF-α; reduce T-cell proliferation; reduce neutrophil migration
Effects:
- Carbohydrate: ↑ gluconeogenesis, insulin resistance → hyperglycemia
- Protein: catabolic (muscle wasting, skin thinning)
- Fat: redistribution → central obesity (buffalo hump, moon face, truncal obesity)
- Calcium: ↓ intestinal Ca absorption, ↑ renal Ca excretion → osteoporosis
- Immune: anti-inflammatory, immunosuppressive
Uses:
- Replacement therapy: Addison's disease, CAH (congenital adrenal hyperplasia)
- Anti-inflammatory: asthma, COPD, rheumatoid arthritis, IBD
- Immunosuppression: organ transplant, SLE
- Cerebral edema (dexamethasone)
- Antenatal: betamethasone/dexamethasone for fetal lung maturity (preterm labor)
- Thyroid storm (hydrocortisone)
- Septic shock (hydrocortisone)
- Dexamethasone suppression test (diagnosis of Cushing's syndrome)
- Allergy/anaphylaxis (adjunct)
ADRs (MBBS high-yield):
- HPA axis suppression (never stop abruptly - taper gradually)
- Cushing-like syndrome: moon face, buffalo hump, striae, obesity
- Hyperglycemia / precipitates DM
- Osteoporosis (long-term use)
- Peptic ulcer (combined with NSAIDs = very high risk)
- Growth retardation in children
- Cataracts, glaucoma
- Psychiatric effects: euphoria, psychosis
- Opportunistic infections
- Hypertension, hypokalemia, sodium/water retention (mineralocorticoid effects)
Contraindications: Active infections (TB, fungal), uncontrolled DM, active peptic ulcer, psychosis, osteoporosis (relative)
3.2 Mineralocorticoids
Fludrocortisone - main drug used clinically
- MOA: Acts on mineralocorticoid receptor in renal collecting duct → ↑ Na⁺ reabsorption, ↑ K⁺ excretion, ↑ H⁺ excretion
- Use: Addison's disease (primary adrenal insufficiency) - combined with hydrocortisone; orthostatic hypotension
Spironolactone, Eplerenone - Mineralocorticoid receptor ANTAGONISTS
- Used in: hyperaldosteronism (Conn's syndrome), heart failure, hypertension
- Spironolactone ADRs: gynecomastia, menstrual irregularities (anti-androgen effect)
- Eplerenone: more selective, less anti-androgen effects
UNIT 4: SEX HORMONES & ORAL CONTRACEPTIVES
4.1 Estrogens
Natural: Estradiol (most potent), Estrone, Estriol (pregnancy)
Synthetic: Ethinyl estradiol, Mestranol
MOA: Bind nuclear estrogen receptor (ERα, ERβ) → gene transcription
Uses:
- Hormone replacement therapy (menopause)
- Oral contraceptives (combined with progestin)
- Dysfunctional uterine bleeding
- Osteoporosis prevention
- Hypogonadism
ADRs: Nausea, breast tenderness, thromboembolism (DVT/PE), endometrial hyperplasia/cancer (unopposed estrogen), cervical erosion
4.2 Progestins
Natural: Progesterone
Synthetic: Norethisterone, Levonorgestrel, Medroxyprogesterone (MPA), Desogestrel, Norgestimate
MOA: Bind progesterone receptor → prepare endometrium for implantation, maintain pregnancy
Uses:
- Combined OCP, Progestin-only pill (POP/"mini-pill")
- Threatened/habitual abortion
- Endometriosis, endometrial carcinoma
- Contraception (DMPA injections, Norplant implants, Mirena IUD)
4.3 Oral Contraceptives
Combined OCP (COCP): Estrogen (ethinyl estradiol) + Progestin
Mechanisms of contraception:
- Inhibit ovulation (suppress LH surge via negative feedback on GnRH/LH/FSH)
- Thicken cervical mucus (sperm-hostile)
- Thin endometrium (unfavorable for implantation)
- Impair tubal motility
ADRs:
- Nausea, breast tenderness, breakthrough bleeding
- Thromboembolic disease (DVT, PE, stroke) - estrogen component
- Hypertension
- Headache, migraine
- Decreased libido
- Chloasma (skin pigmentation)
Absolute Contraindications: History of DVT/PE, stroke, ischemic heart disease, breast cancer, migraine with aura, age >35 + smoker, active liver disease, pregnancy
Emergency Contraception:
- Levonorgestrel (Plan B): 1.5 mg single dose within 72 hours (up to 120 h)
- Ulipristal acetate (EllaOne): within 120 h; progesterone receptor modulator
- Copper IUD: within 5 days - most effective emergency contraception
4.4 Androgens & Antiandrogens
Testosterone & derivatives: Testosterone cypionate, Oxandrolone, Stanozolol (anabolic steroids)
- Uses: Male hypogonadism, anemia, catabolic states, delayed puberty
- ADRs: Virilization in females, hepatotoxicity (17α-alkylated forms), polycythemia
Antiandrogens:
- Finasteride: 5-alpha reductase inhibitor → blocks DHT → BPH, male-pattern baldness
- Spironolactone: Mineralocorticoid/androgen antagonist → hirsutism, PCOS
- Flutamide, Bicalutamide: Androgen receptor blockers → prostate cancer
- Cyproterone acetate: Antiandrogen → hirsutism, precocious puberty
UNIT 5: ANTERIOR PITUITARY HORMONES
Clinically Important Preparations
| Hormone | Drug Used | Indication |
|---|---|---|
| GH (Growth Hormone) | Somatropin | GH deficiency, Turner's syndrome, CKD-related short stature |
| GH inhibitor | Octreotide (somatostatin analog) | Acromegaly, carcinoid, VIPoma |
| FSH/LH | Gonadotropins (FSH, hMG) | Infertility |
| GnRH agonists | Leuprolide, Goserelin | Prostate cancer, endometriosis, precocious puberty (continuous use = suppression) |
| GnRH antagonists | Cetrorelix, Ganirelix | Infertility (IVF protocols) |
| Prolactin inhibitors | Bromocriptine, Cabergoline | Prolactinoma, hyperprolactinemia |
| TSH analog | Thyrotropin alfa | Thyroid cancer follow-up |
| ACTH | Cosyntropin (synthetic) | Adrenal insufficiency diagnosis |
| Vasopressin/ADH | Desmopressin (DDAVP) | Diabetes insipidus, nocturnal enuresis, hemophilia A/VWD |
| Oxytocin | Syntocinon | Labor induction, PPH prevention |
Key Points on Bromocriptine:
- Dopamine D2 agonist → inhibits prolactin secretion
- Used in: prolactinoma, hyperprolactinemia, Parkinson's disease, type 2 DM (novel use), acromegaly
- ADRs: Nausea, postural hypotension, nasal congestion
HIGH-YIELD EXAM POINTS
Compare Methimazole vs. PTU
| Feature | Methimazole | PTU |
|---|---|---|
| Dosing | Once daily | 3-4 times daily |
| Peripheral T4→T3 inhibition | No | Yes |
| Preferred in pregnancy | 2nd/3rd trimester | 1st trimester |
| Hepatotoxicity | Cholestatic jaundice | Severe hepatitis (Black Box) |
| Teratogenicity | Aplasia cutis, choanal atresia | Relatively safer |
| Preferred in thyroid storm | No | Yes |
Wolff-Chaikoff Effect vs. Jod-Basedow Phenomenon
| Feature | Wolff-Chaikoff | Jod-Basedow |
|---|---|---|
| What happens | High iodide → inhibits organification → hypothyroidism | High iodide → hyperthyroidism |
| Who is susceptible | Normal thyroid / Hashimoto's | Multinodular goiter, Graves' |
| Duration | Transient (gland escapes in 2 weeks) | Persistent |
Drugs Causing Thyroid Dysfunction
- Amiodarone: Contains 37% iodine → both hypo and hyperthyroidism; also inhibits T4→T3 conversion
- Lithium: Inhibits hormone release → hypothyroidism, goiter
- Interferon-alpha: Autoimmune thyroiditis
- Tyrosine kinase inhibitors: Hypothyroidism
Quick Memory Aids
- "PTU first in thyroid storm" - P for Propranolol, T for thioamide (PTU), U for Umbilical (iodide 1 hour AFTER), hydrocortisone
- Sulfonylureas need beta cells - do not work in Type 1 DM
- Metformin = weight neutral/loss, no hypoglycemia - first choice T2DM
- SGLT2i = glucose excreted in urine = glycosuria (treat genital infections proactively)
- GLP-1 agonists = "lose weight, protect heart"
- Dexamethasone = most potent glucocorticoid, zero mineralocorticoid activity, crosses placenta, fetal lung maturity
- Fludrocortisone = pure mineralocorticoid for Addison's
- Levonorgestrel emergency contraception within 72 hours; Copper IUD most effective (up to 5 days)
- Finasteride = 5-alpha reductase inhibitor → reduces DHT → BPH + male pattern baldness
Sources: Katzung's Basic and Clinical Pharmacology, 16th Ed. | Goodman & Gilman's The Pharmacological Basis of Therapeutics | Lippincott Illustrated Reviews: Pharmacology
Teach me in very easy English and covering all important topics from taking reference from kd tripathi
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have very rich content. Let me compile the complete, easy-English KD Tripathi-style notes:
🧬 ENDOCRINE PHARMACOLOGY
MBBS 2nd Year - Easy English Notes (KD Tripathi Style)
References: Katzung's Basic & Clinical Pharmacology 16th Ed., Lippincott Illustrated Reviews: Pharmacology, Goodman & Gilman's
💡 How to use these notes: Think of the endocrine system as a boss and worker system. The brain (hypothalamus + pituitary) is the boss. The glands (thyroid, adrenal, pancreas) are the workers. Drugs either mimic, block, or modify this communication.
CHAPTER 1: THYROID & ANTITHYROID DRUGS
🔑 First, Understand the System Simply
Think of the thyroid gland like a factory that makes energy fuel (T3 and T4 hormones).
- The brain sends orders via TRH (from hypothalamus) → TSH (from pituitary) → Thyroid makes T3 & T4
- T3 and T4 then go back and tell the brain "enough, stop ordering" - this is called negative feedback
The hypothalamus-pituitary-thyroid axis. TRH stimulates TSH, which stimulates T3/T4 production. T3/T4 feedback inhibits both. Somatostatin and dopamine also inhibit TSH. Large iodide (I⁻) blocks thyroid hormone production. - Katzung's Basic and Clinical Pharmacology, 16th Ed.
How Thyroid Makes Hormones (Step-by-Step - VERY IMPORTANT for Exams)
Imagine iodine as the raw material the factory needs:
| Step | What Happens | Drug that Blocks This Step |
|---|---|---|
| 1. Iodide trapping | Iodide enters thyroid via NIS pump | Perchlorate, thiocyanate |
| 2. Oxidation | TPO enzyme converts iodide → active iodine | Thioamides (PTU, Methimazole) |
| 3. Organification | Iodine attached to tyrosine → MIT, DIT | Thioamides, high-dose iodide |
| 4. Coupling | MIT + DIT → T3; DIT + DIT → T4 | Thioamides |
| 5. Release | T3/T4 released into blood | High-dose iodide (Wolff-Chaikoff) |
| 6. T4 → T3 conversion | In peripheral tissues (liver, kidney) | PTU, propranolol, steroids, amiodarone |
PART A: DRUGS FOR HYPOTHYROIDISM (Under-active thyroid)
Patient is "slow" - tired, weight gain, cold intolerance, constipation, slow pulse
The solution is simple: Give them thyroid hormone!
| Drug | What it is | Key Points |
|---|---|---|
| Levothyroxine (T4) | Synthetic T4 | ⭐ DRUG OF CHOICE. Dose = 1.7 mcg/kg/day. Take on EMPTY STOMACH. Half-life = 7 days |
| Liothyronine (T3) | Synthetic T3 | Faster, more potent. Used in MYXEDEMA COMA (emergency) |
| Liotrix | T4:T3 mix (4:1) | Not preferred |
| Desiccated thyroid | From animal thyroid | Old preparation, unreliable |
🚨 Why Take Levothyroxine on Empty Stomach?
Because calcium antacids, iron, omeprazole reduce absorption. Take it 30-60 minutes before food. Separate calcium by 4 hours.
🔍 How to Monitor: Check TSH after 6-8 weeks
Special Case - Myxedema Coma (life-threatening hypothyroidism):
- Give IV liothyronine (T3) - faster acting
- Plus IV hydrocortisone (because adrenal function may be suppressed too)
PART B: ANTITHYROID DRUGS (For Hyperthyroidism)
Patient is "fast" - weight loss, sweating, palpitations, diarrhea, bulging eyes (in Graves' disease)
Four Types of Antithyroid Treatment:
1. THIOAMIDES (Most Important Drug Class!)
Two drugs: Propylthiouracil (PTU) and Methimazole (Carbimazole is a prodrug → methimazole in body)
Simple Mechanism:
Think of thioamides as blocking the TPO enzyme (the machine that activates iodine). No active iodine = no hormone made.
What they do:
- Block TPO → block organification → no T3/T4 made
- Block coupling of MIT + DIT
- PTU ONLY: Also blocks peripheral T4 → T3 conversion (extra benefit!)
- ❌ They do NOT block iodide uptake into the gland
Onset: SLOW (3-4 weeks) - because stored hormone must be used up first
Methimazole vs PTU - KD Tripathi Favourite Comparison!
| Feature | Methimazole | PTU |
|---|---|---|
| Daily doses | Once daily (longer half-life) | 3-4 times daily |
| Blocks T4→T3 conversion? | ❌ No | ✅ Yes |
| Preferred in pregnancy | 2nd & 3rd trimester | 1st trimester ✅ |
| Teratogenicity | Aplasia cutis, choanal atresia | Relatively safer (1st trimester) |
| Liver toxicity | Cholestatic jaundice (milder) | Severe hepatitis - BLACK BOX WARNING |
| Preferred in thyroid storm? | ❌ No | ✅ Yes (blocks conversion too) |
| 1st choice for most patients | ✅ YES | Only in specific cases |
Adverse Effects of Thioamides:
- Most common: Maculopapular itchy rash (4-6%), nausea
- Most dangerous: Agranulocytosis (0.1-0.5%) - sudden drop in WBC → fever + sore throat = STOP DRUG immediately!
- Cross-sensitivity between PTU and methimazole = 50% → don't switch if serious reaction
- PTU: Fatal hepatitis (rare but black box)
- Methimazole: altered taste/smell, cholestatic jaundice
2. IODIDES (High-Dose Iodine) - Paradoxical Effect!
Normal iodine = needed for hormone production
HIGH dose iodine = STOPS hormone production ← This is the paradox!
Preparations: Lugol's iodine (5% I₂ + 10% KI), SSKI (potassium iodide solution)
Mechanisms of action:
- Wolff-Chaikoff Effect: Large iodide → blocks organification → reduces T3/T4 synthesis
- Reduces vascularity and size of the thyroid (useful before surgery)
- Reduces hormone release
Uses:
- Pre-operative prep for thyroidectomy (given 10-14 days before operation to shrink gland)
- Thyroid storm (given 1 hour AFTER thioamides! Never before!)
- Radiation emergency - protects thyroid from radioactive fallout
⭐ The Jod-Basedow vs Wolff-Chaikoff - HIGH YIELD!
| Wolff-Chaikoff Effect | Jod-Basedow Phenomenon | |
|---|---|---|
| What happens | High iodide → BLOCKS hormone → Hypothyroidism | High iodide → TRIGGERS excess hormone → Hyperthyroidism |
| Who gets it? | Normal thyroid, Hashimoto's patients | People with multinodular goiter |
| How long? | Temporary (gland "escapes" in 2 weeks) | Persistent |
| Example | Amiodarone → hypothyroidism | Amiodarone → hyperthyroidism |
3. RADIOACTIVE IODINE (¹³¹I) - The "Radiation Bomb"
Mechanism: Thyroid traps ¹³¹I just like normal iodine. But ¹³¹I emits beta radiation → destroys thyroid follicular cells from inside!
Use: Treatment of choice for Graves' disease in non-pregnant adults
Key Points:
- Contraindicated in pregnancy and breastfeeding
- Usually causes permanent hypothyroidism → needs lifelong levothyroxine
- Can worsen thyroid eye disease (ophthalmopathy) - especially in smokers
- Give 1 week AFTER stopping antithyroid drugs
4. BETA-BLOCKERS (Symptomatic Relief Only)
Propranolol (non-selective beta-blocker) is used in hyperthyroidism:
- Controls palpitations, tremor, sweating, anxiety, heat intolerance
- Propranolol at HIGH doses also inhibits peripheral T4 → T3 conversion (unlike other beta-blockers)
- Does NOT treat the cause - only relieves symptoms
- Also used in thyroid storm
5. ANION INHIBITORS
Perchlorate, Thiocyanate, Pertechnetate → Competitively block NIS pump → iodide cannot enter thyroid
- Rarely used clinically (risk of aplastic anemia with perchlorate)
- Potassium perchlorate: used in amiodarone-induced hyperthyroidism
🔥 THYROID STORM - High Yield Protocol
What is it? Life-threatening explosive release of thyroid hormones - medical emergency!
Treatment sequence (Remember: "P-T-I-S"):
| Step | Drug | Why |
|---|---|---|
| 1 | Propranolol (IV) | Control heart rate, block T4→T3 |
| 2 | PTU (500-1000 mg loading, then 250 mg every 4h) | Block synthesis + T4→T3 |
| 3 | Iodide (Lugol's/SSKI) - give 1 hour AFTER PTU | Block hormone release |
| 4 | Steroids (Hydrocortisone 50 mg IV every 6h) | Prevent shock + block T4→T3 |
| + | Supportive: fever control, IV fluids |
🧠 Memory trick: "P-T-I-S" = Propranolol, Thioamide (PTU), Iodide (1 hr later), Steroids
Drugs That Affect Thyroid Function (Important Exam Topic!)
| Drug | Effect on Thyroid | Mechanism |
|---|---|---|
| Amiodarone | Both hypo AND hyperthyroidism | 37% iodine by weight; also blocks T4→T3 |
| Lithium | Hypothyroidism, goiter | Inhibits hormone release |
| Interferon-alpha | Autoimmune thyroiditis | Immune activation |
| Rifampicin, Phenytoin | Reduces T4 levels | Induces hepatic enzymes → faster metabolism |
| Estrogen, OCP | ↑ TBG → ↑ total T4 (but free T4 normal) | Increases thyroid binding globulin |
CHAPTER 2: INSULIN & ANTIDIABETIC DRUGS
First, Understand Diabetes Simply
Type 1 DM: Beta cells in pancreas are destroyed (autoimmune). No insulin at all. Like a factory that burned down.
Type 2 DM: Beta cells are tired and weak. Body cells also don't respond to insulin (insulin resistance). Like a lazy factory + deaf workers.
Diagnosis (remember the numbers!):
- Fasting glucose ≥ 126 mg/dL
- 2-hr post-meal glucose ≥ 200 mg/dL
- HbA1c ≥ 6.5% (reflects 3 months of average sugar)
- Prediabetes: fasting 100-125 mg/dL, HbA1c 5.7-6.4%
INSULIN
Types of Insulin - Read the Graph!
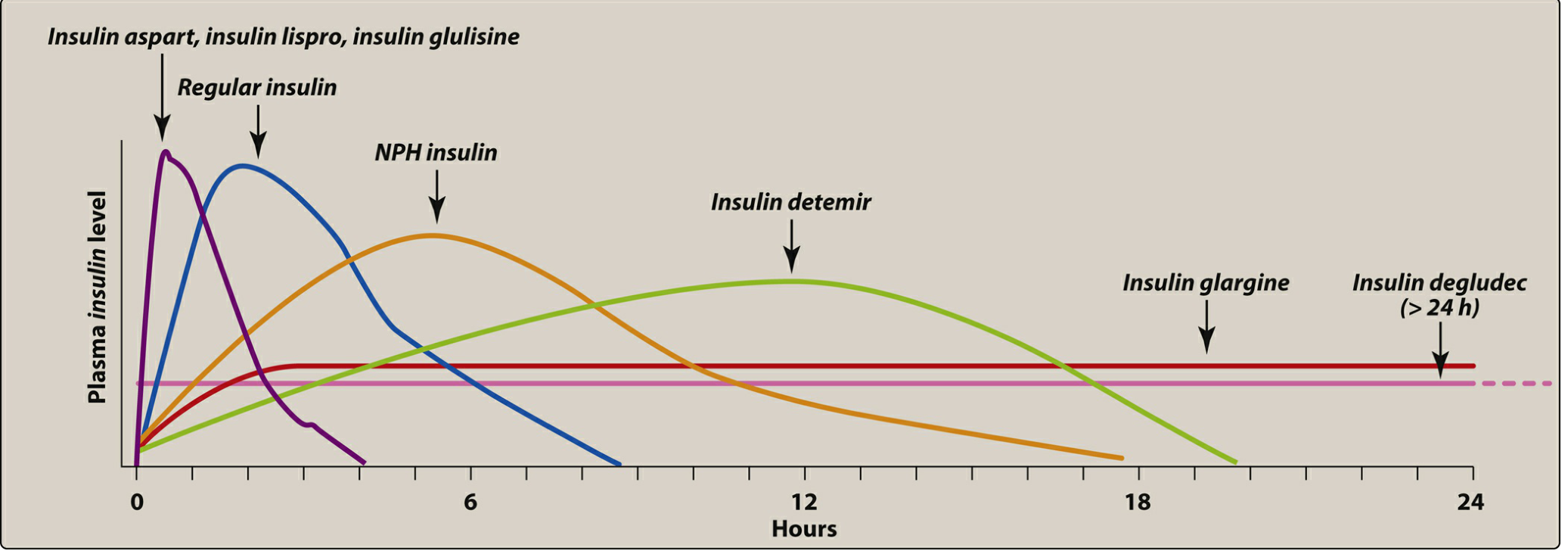
Onset and duration of action of different insulin preparations. Rapid-acting analogs (lispro, aspart, glulisine) peak earliest. Regular insulin peaks at 2-4h. NPH is intermediate. Glargine and degludec provide near-flat, long-acting coverage. - Lippincott Illustrated Reviews: Pharmacology
Insulin Types - Easy Comparison Table
| Type | Drugs | Onset | Peak | Duration | When Given |
|---|---|---|---|---|---|
| Rapid-acting | Lispro, Aspart, Glulisine | 5-15 min | 1-2 h | 3-5 h | Just before or after meal |
| Short-acting | Regular insulin | 30-60 min | 2-4 h | 6-8 h | 30 min before meal |
| Intermediate | NPH (Isophane) | 1-2 h | 6-10 h | 16-24 h | BD or OD |
| Long-acting | Glargine, Detemir | 1-4 h | No peak (flat) | 20-24 h | Once at night |
| Ultra-long | Degludec | 1-2 h | No peak | >42 h | Once daily |
How Regular Insulin is Different from Analogs:
- Regular insulin = crystalline zinc insulin = clear, given 30 min BEFORE meals
- Rapid analogs (Lispro, Aspart) = amino acid sequence modified → faster absorbed → give 15 min before or immediately after meal
- NPH = regular insulin + protamine + zinc = cloudy, intermediate
- Glargine = modified to precipitate at neutral pH (subcutaneous) → slow, no peak = "peakless basal insulin"
Mechanism of Action of Insulin:
Insulin binds to insulin receptor (tyrosine kinase receptor) on cell surface → signals GLUT-4 transporters to move to surface → glucose enters the cell
What insulin does in the body:
- ↑ glucose uptake (muscle, fat)
- ↑ glycogen synthesis (liver, muscle)
- ↑ protein synthesis
- ↑ fat storage (lipogenesis)
- ↓ gluconeogenesis, glycogenolysis, lipolysis
- Drives K⁺ INTO cells (used in hyperkalemia treatment!)
Adverse Effects of Insulin:
- Hypoglycemia - most common and important!
- Weight gain - promotes fat storage
- Lipodystrophy at injection site - lipoatrophy (fat loss) or lipohypertrophy (fat buildup)
- Hypokalemia - insulin pushes K⁺ into cells
- Insulin allergy (rare)
Special Uses of Insulin:
- Type 1 DM: MANDATORY (no beta cells = no choice)
- Type 2 DM: when oral drugs fail
- DKA (Diabetic Ketoacidosis): IV regular insulin
- Hyperkalemia: IV insulin + dextrose → drives K⁺ into cells (rapid fix)
- Gestational diabetes
ORAL ANTIDIABETIC DRUGS (OADs)
🧠 Simple way to remember all OAD classes: "B-S-M-T-A-D-G-S" (Biguanides, Sulfonylureas, Meglitinides, TZDs, Alpha-glucosidase inhibitors, DPP-4 inhibitors, GLP-1 agonists, SGLT-2 inhibitors)
1. BIGUANIDES - METFORMIN ⭐ (DRUG OF CHOICE FOR TYPE 2 DM)
Simple explanation: Metformin tells the liver - "Stop making new glucose from scratch (gluconeogenesis)!"
Mechanism:
- Activates AMPK enzyme in liver → shuts down gluconeogenesis
- Also increases insulin sensitivity in muscle
- Does NOT stimulate insulin release → does NOT cause hypoglycemia alone
Why it is the BEST first-choice drug:
- ✅ No weight gain (actually may reduce weight)
- ✅ No hypoglycemia when used alone
- ✅ Cheap, proven, safe
- ✅ Cardiovascular benefit (UKPDS study)
Adverse Effects:
- GI effects (nausea, diarrhea, metallic taste) - most common; take with food to reduce
- Lactic acidosis - rare but serious, especially in renal failure
- Reduces B12 absorption (long-term use)
Contraindications (when NOT to use):
- eGFR < 30 (severe kidney disease) - lactic acidosis risk
- Liver failure, alcohol abuse
- Hold before IV contrast dye (48 hours before and after)
- Hypoxic states (heart failure, respiratory failure)
2. SULFONYLUREAS ⭐ (Second Most Important)
Simple explanation: Sulfonylureas literally "squeeze" the beta cell to release insulin regardless of blood sugar!
Mechanism:
Block ATP-sensitive K⁺ channels on beta cells → K⁺ can't leave → cell depolarizes → Ca²⁺ enters → insulin granules released!
Drugs:
- 1st generation (older): Tolbutamide, Chlorpropamide, Glibenclamide
- 2nd generation (better, preferred): Glipizide, Glibenclamide (Glyburide), Glimepiride
Adverse Effects:
- Hypoglycemia - most important! (Because they stimulate insulin even when glucose is normal/low)
- Weight gain (due to insulin release)
- Sulfa allergy cross-reactivity (rare)
Chlorpropamide special points (exam favourite!):
- Longest acting sulfonylurea
- Causes disulfiram-like reaction with alcohol (flushing, nausea)
- Causes SIADH (water retention)
- Not preferred now due to prolonged hypoglycemia
Important: Sulfonylureas NEED working beta cells to work → useless in Type 1 DM!
3. MEGLITINIDES (Glinides)
Drugs: Repaglinide, Nateglinide
Same mechanism as sulfonylureas (block K⁺ channels) BUT:
- Much faster onset, shorter duration
- Taken just before each meal
- Controls postprandial (after-meal) glucose
- Less hypoglycemia risk than sulfonylureas
- Do NOT combine with sulfonylureas (same mechanism = double risk of hypoglycemia)
4. THIAZOLIDINEDIONES (TZDs / Glitazones)
Drugs: Pioglitazone (preferred), Rosiglitazone (restricted use)
Simple explanation: TZDs make body cells "listen" to insulin better - they reduce insulin resistance.
Mechanism:
Activate PPAR-γ (nuclear receptor) in fat/muscle/liver → cells become more insulin sensitive → glucose uptake improves
Key Points:
- Do NOT cause hypoglycemia alone
- Need 2-3 months to show full effect
- Need insulin to be present to work
Adverse Effects:
- Weight gain + edema (fluid retention)
- Heart failure - CONTRAINDICATED in heart failure!
- Osteoporosis + fractures (especially in women)
- Pioglitazone: slight risk of bladder cancer (long-term)
- Rosiglitazone: cardiovascular concerns → mostly withdrawn
5. ALPHA-GLUCOSIDASE INHIBITORS
Drugs: Acarbose, Miglitol, Voglibose
Simple explanation: Think of these as "speed bumps" in the intestine. They slow down digestion of carbohydrates so sugar is absorbed slowly → no postprandial spike.
Mechanism:
Inhibit intestinal alpha-glucosidase enzyme → delay CHO breakdown → slow glucose absorption → reduce postprandial hyperglycemia
Adverse Effects:
- Gas, flatulence, bloating, diarrhea (very common - undigested CHO ferments in colon)
- No hypoglycemia alone
- ⭐ Important: If hypoglycemia occurs (due to combination therapy) → treat with pure glucose (NOT sucrose/table sugar) because sucrose needs the same enzyme that is blocked!
6. DPP-4 INHIBITORS (Gliptins)
Drugs: Sitagliptin, Vildagliptin, Saxagliptin, Alogliptin, Teneligliptin
Simple explanation: DPP-4 is a scissor enzyme that cuts and destroys GLP-1. Gliptins break this scissor → GLP-1 levels rise → more insulin released.
Mechanism:
Inhibit DPP-4 enzyme → GLP-1 and GIP levels rise → glucose-dependent insulin secretion increases + glucagon decreases
Key features:
- Insulin release only when glucose is high → minimal hypoglycemia
- Weight neutral
- Safe in elderly
Adverse Effects:
- Upper respiratory infections, nasopharyngitis
- Urinary tract infections
- Rare: pancreatitis, joint pain
7. GLP-1 RECEPTOR AGONISTS (Incretins)
Drugs: Exenatide (Byetta), Liraglutide (Victoza), Semaglutide, Dulaglutide
Simple explanation: These drugs ARE GLP-1 itself (or similar). They do everything GLP-1 does - and more!
Mechanism: Act on GLP-1 receptors:
- ↑ insulin secretion (glucose-dependent)
- ↓ glucagon secretion
- ↓ gastric emptying (food stays longer → feel full)
- ↓ appetite (act on brain)
- → Significant weight loss
Additional benefits:
- Cardiovascular protection (liraglutide, semaglutide - proven in trials)
- Renal protection (semaglutide)
Adverse Effects:
- Nausea, vomiting (most common - improves with time)
- Rare: pancreatitis
- Thyroid C-cell tumors in animal studies (caution in MEN-2, thyroid cancer history)
- Given as subcutaneous injection (semaglutide also available as oral pill)
8. SGLT-2 INHIBITORS (Gliflozins) - Newest & Trendy!
Drugs: Dapagliflozin (Forxiga), Empagliflozin (Jardiance), Canagliflozin
Simple explanation: Kidneys normally "save" all glucose from the urine and put it back into blood. SGLT-2 inhibitors break this recycling pump → glucose spills into urine → blood sugar falls!
Mechanism:
Block SGLT-2 transporter in proximal tubule of kidney → glucose not reabsorbed → glycosuria (glucose in urine)
Benefits beyond glucose:
- Weight loss (glucose = calories wasted in urine)
- Blood pressure reduction (osmotic diuresis)
- Heart failure benefit - reduces hospitalizations!
- Kidney protection - reduces CKD progression
Adverse Effects:
- Genital fungal infections (glucose in urine = food for fungi) - most common!
- Urinary tract infections
- Polyuria
- Euglycemic DKA (DKA even when glucose is normal - rare but dangerous)
- Fournier's gangrene (necrotizing fasciitis of genitals - rare)
- ❌ Do NOT use if eGFR < 30
📊 Master Summary Table - All Oral Antidiabetics
| Drug Class | Mechanism (1 word) | Causes Hypoglycemia? | Weight Effect | Top ADR | Unique Feature |
|---|---|---|---|---|---|
| Metformin | ↓gluconeogenesis | ❌ No | ↓ lose | Lactic acidosis | 1st choice, no wt gain |
| Sulfonylureas | ↑ insulin secretion | ✅ Yes | ↑ gain | Hypoglycemia | Need working beta cells |
| Meglitinides | ↑ insulin (postprandial) | Mild | ↑ slight | Hypoglycemia | Pre-meal, short acting |
| TZDs | PPAR-γ agonist | ❌ No | ↑↑ gain | Edema, fractures | CI in heart failure |
| Acarbose | Delay CHO absorption | ❌ No | Neutral | Flatulence | Treat hypo with glucose! |
| DPP-4i (Gliptins) | ↑ GLP-1 (inhibit breakdown) | ❌ No | Neutral | Nasopharyngitis | Weight neutral |
| GLP-1 agonists | GLP-1 mimic | ❌ No | ↓↓ lose | Nausea/vomiting | CV + weight benefit |
| SGLT-2i (Gliflozins) | Glycosuria | ❌ No | ↓ lose | Genital infections | CV + renal benefit |
CHAPTER 3: GLUCOCORTICOIDS
Think of Glucocorticoids as the Body's "Stress Hormone"
Cortisol is released in stress. It raises blood sugar (glucose = energy for fight/flight), suppresses inflammation (so you don't swell up in battle), and mobilizes energy stores.
Natural vs Synthetic Glucocorticoids
| Drug | Glucocorticoid Potency | Mineralocorticoid Effect | Duration | Dose Equivalent |
|---|---|---|---|---|
| Hydrocortisone | 1 (reference) | 1 | Short (8-12h) | 20 mg |
| Prednisolone | 4 | 0.8 | Medium (12-36h) | 5 mg |
| Methylprednisolone | 5 | 0.5 | Medium | 4 mg |
| Dexamethasone | 25-30 | ≈ 0 (none!) | Long (36-72h) | 0.75 mg |
| Betamethasone | 25-30 | ≈ 0 | Long | 0.6 mg |
| Fludrocortisone | 10 | 125-150 | - | (mineralocorticoid) |
⭐ Dexamethasone = most potent glucocorticoid + ZERO mineralocorticoid activity = perfect when you want only anti-inflammatory effect (cerebral edema, fetal lung maturity)
Mechanism of Action (Simple Version)
Glucocorticoid → enters cell → binds cytoplasmic glucocorticoid receptor (GR) → GR-steroid complex enters nucleus → binds DNA (GRE) → changes gene expression
Anti-inflammatory mechanism: ↑ Lipocortin (annexin-1) → inhibits phospholipase A₂ → less arachidonic acid → less prostaglandins AND leukotrienes (blocks both COX and LOX pathways!)
Immunosuppressive mechanism: Inhibit NF-κB → less IL-1, IL-2, TNF-α → reduced T-cell and neutrophil activity
Effects of Glucocorticoids on the Body
| System | Effect | Clinical Result |
|---|---|---|
| Carbohydrate | ↑ gluconeogenesis, ↓ glucose uptake | Hyperglycemia ("steroid diabetes") |
| Protein | Catabolic | Muscle wasting, thin skin, poor wound healing |
| Fat | Redistribution | Moon face, buffalo hump, truncal obesity |
| Calcium | ↓ gut absorption, ↑ urine excretion | Osteoporosis |
| Immune | Anti-inflammatory | Infection risk |
| CVS | ↑ BP (mineralocorticoid effect) | Hypertension |
| Stomach | ↑ acid, ↓ mucus | Peptic ulcer |
| Eye | ↑ IOP | Glaucoma, cataracts |
| HPA axis | Suppresses ACTH | Adrenal atrophy |
| Bone | ↓ osteoblast activity | Osteoporosis, fractures |
Clinical Uses of Glucocorticoids
1. Replacement therapy (physiological dose):
- Addison's disease (adrenal insufficiency): hydrocortisone + fludrocortisone
- Congenital adrenal hyperplasia (CAH)
2. Anti-inflammatory / Immunosuppressive (pharmacological dose):
- Asthma, COPD (budesonide inhaler, prednisolone)
- Rheumatoid arthritis, SLE
- Inflammatory bowel disease
- Allergic reactions, anaphylaxis (adjunct)
- Organ transplant rejection prevention
3. Special uses (high-yield!):
- Cerebral edema: Dexamethasone (no mineralocorticoid = no Na/water retention!)
- Fetal lung maturity (preterm labor): Betamethasone or Dexamethasone given to mother at 24-34 weeks
- Thyroid storm: Hydrocortisone (blocks T4→T3 + prevents shock)
- Septic shock: Hydrocortisone (relative adrenal insufficiency)
- Cushing's syndrome diagnosis: Dexamethasone suppression test
Adverse Effects - "Cushing's Syndrome in a Box"
Long-term steroid use = iatrogenic Cushing's syndrome:
🧠 Memory trick: "WASHED"
- Weight gain, moon face, buffalo hump
- Adrenal suppression (never stop abruptly!)
- Sugar raised (hyperglycemia, steroid diabetes)
- Hypertension + Hypokalemia
- Eyes (cataracts, glaucoma)
- Decreased immunity + Delayed wound healing + Depression/psychosis
Plus: Osteoporosis, peptic ulcer, growth retardation in children, striae (stretch marks), acne
⭐ Steroid Withdrawal - Never Stop Abruptly!
Long-term steroids → HPA axis suppressed → adrenal glands shrink (atrophy)
If you stop suddenly → adrenal crisis (life-threatening!): hypotension, shock, fever
Always taper gradually when stopping long-term steroids!
MINERALOCORTICOIDS
Fludrocortisone:
- Acts on mineralocorticoid receptor in kidney collecting duct
- ↑ Na⁺ reabsorption, ↑ K⁺ excretion, ↑ H⁺ excretion → retains sodium and water
- Used in: Addison's disease (combined with hydrocortisone), orthostatic hypotension
Spironolactone & Eplerenone = Mineralocorticoid ANTAGONISTS (blockers)
- Block aldosterone receptor
- Used in: Conn's syndrome (hyperaldosteronism), heart failure, hypertension
- Spironolactone ADRs: gynecomastia, menstrual irregularities (also has anti-androgen effect)
- Eplerenone: more selective, fewer hormonal side effects
CHAPTER 4: SEX HORMONES & ORAL CONTRACEPTIVES
ESTROGENS
Natural: Estradiol (most potent), Estrone, Estriol (in pregnancy)
Synthetic: Ethinyl estradiol (used in OCP), Diethylstilbestrol (DES - historical)
Mechanism: Bind nuclear estrogen receptors (ERα, ERβ) → change gene expression
Uses:
- OCP (combined with progestin)
- Hormone replacement therapy (HRT) for menopause symptoms
- Hypogonadism in females
- Osteoporosis prevention
- Dysfunctional uterine bleeding
Adverse Effects:
- Nausea, breast tenderness
- Thromboembolism (DVT, PE, stroke) - most dangerous!
- Hypertension
- Endometrial hyperplasia/cancer (if used alone without progestin)
- Breast cancer risk (long-term)
PROGESTINS
Natural: Progesterone
Synthetic: Norethisterone, Levonorgestrel, Medroxyprogesterone acetate (MPA), Desogestrel
Uses:
- OCP, Progestin-only pill (POP / mini-pill)
- Threatened/habitual abortion
- Endometriosis
- Contraception (DMPA injection = Depo-Provera, Mirena IUD)
ORAL CONTRACEPTIVES - VERY IMPORTANT FOR EXAMS!
Combined OCP (Estrogen + Progestin)
How does it prevent pregnancy? (3 mechanisms):
- Inhibits ovulation - suppresses LH surge via negative feedback on GnRH → no egg released (main mechanism)
- Thickens cervical mucus - sperm cannot swim through
- Thins endometrium - even if fertilized, egg cannot implant
Types of Combined OCP:
- Monophasic: Same dose every day (e.g., Yasmin - ethinyl estradiol + drospirenone)
- Biphasic/Triphasic: Varying doses across the cycle
Adverse Effects of OCP:
- Nausea (most common early complaint)
- Breast tenderness
- Breakthrough (irregular) bleeding
- Thromboembolism - estrogen increases clotting factors → DVT/PE/stroke risk
- Hypertension
- Headache, migraine
- Chloasma (dark skin patches, especially with sun exposure)
- Reduced libido
Absolute Contraindications of OCP ("FACH rule"):
- Family history of VTE / Previous DVT or PE
- Age >35 + Smoker (5-10x VTE risk)
- Cardiovascular disease, ischemic heart disease, stroke history
- Hepatitis/liver disease, breast cancer, migraine with aura, pregnancy
Progestin-Only Pill (POP / Mini-Pill)
- No estrogen → safer in breastfeeding mothers, smokers >35, hypertension patients
- Works mainly by thickening cervical mucus
- Must be taken at SAME TIME every day (less forgiving than combined OCP)
EMERGENCY CONTRACEPTION ("Morning After Pill")
| Method | Drug | Time Limit | Mechanism |
|---|---|---|---|
| Plan B | Levonorgestrel 1.5 mg | Within 72 h (up to 120 h) | Delays/inhibits ovulation |
| Ella | Ulipristal acetate | Within 120 h (5 days) | Progesterone receptor modulator |
| Copper IUD | Copper device | Within 5 days | Most effective; hostile to sperm + implantation |
⭐ Copper IUD = most effective emergency contraceptive (>99% effective!)
ANDROGENS & ANTIANDROGENS
Testosterone uses: Male hypogonadism, delayed puberty, aplastic anemia
Anabolic steroids (Stanozolol, Oxandrolone): Used in catabolic states, burns (but abused in sports)
Antiandrogens - High-Yield Table:
| Drug | Mechanism | Use |
|---|---|---|
| Finasteride | 5α-reductase inhibitor → blocks DHT formation | BPH, male-pattern baldness |
| Dutasteride | 5α-reductase inhibitor (both types) | BPH |
| Spironolactone | Androgen receptor antagonist | Hirsutism, PCOS, acne |
| Flutamide, Bicalutamide | Pure androgen receptor blockers | Prostate cancer |
| Cyproterone acetate | Androgen receptor antagonist | Hirsutism, precocious puberty |
CHAPTER 5: ANTERIOR PITUITARY HORMONES - Quick Reference
| Hormone | Deficiency Drug (Replace) | Excess Drug (Block) |
|---|---|---|
| Growth Hormone (GH) | Somatropin (rGH) - for dwarfism | Octreotide, Lanreotide (for acromegaly) |
| Gonadotropins (FSH/LH) | hMG, FSH injections - for infertility | GnRH agonists (paradoxical suppression) |
| TSH | Thyrotropin alfa | - |
| ACTH | Cosyntropin (diagnostic) | Metyrapone, Ketoconazole (Cushing's) |
| Prolactin | - | Bromocriptine, Cabergoline |
| ADH (Vasopressin) | Desmopressin (DDAVP) | Demeclocycline (SIADH) |
| Oxytocin | Syntocinon | Atosiban (tocolysis) |
Key Point - GnRH Agonists (Leuprolide, Goserelin):
- Pulsatile use → stimulates FSH/LH → used in infertility
- Continuous use → DOWNREGULATES receptors → SUPPRESSES FSH/LH → like "medical castration"
- Used in: prostate cancer, endometriosis, precocious puberty, uterine fibroids
Bromocriptine (Dopamine D2 agonist):
- Inhibits prolactin secretion
- Used in: prolactinoma, hyperprolactinemia, Parkinson's, type 2 DM (Cycloset)
- ADRs: nausea, postural hypotension, nasal congestion
🏆 EXAM POWER SUMMARY - One Liner Facts
| Topic | One-Liner |
|---|---|
| Drug of choice - hypothyroidism | Levothyroxine (T4) |
| Drug of choice - thyroid storm | PTU + Propranolol + Iodide (1h later) + Hydrocortisone |
| PTU vs Methimazole - 1st trimester | PTU preferred (methimazole = teratogenic) |
| Wolff-Chaikoff | High iodide blocks thyroid hormone synthesis |
| Jod-Basedow | High iodide causes hyperthyroidism in multinodular goiter |
| Amiodarone and thyroid | Can cause BOTH hypo and hyperthyroidism |
| Drug of choice - Type 2 DM | Metformin |
| Only OAD for Type 1 DM | Insulin (only!) |
| Sulfonylurea + alcohol reaction | Chlorpropamide (disulfiram-like reaction) |
| OAD contraindicated in heart failure | TZDs (Glitazones) |
| Treat hypoglycemia from acarbose | Pure glucose, NOT sucrose |
| Most potent glucocorticoid | Dexamethasone |
| Glucocorticoid for fetal lung maturity | Betamethasone or Dexamethasone |
| Glucocorticoid for cerebral edema | Dexamethasone (no mineralocorticoid effect) |
| Adrenal insufficiency replacement | Hydrocortisone + Fludrocortisone |
| Mineralocorticoid antagonist | Spironolactone |
| Gynecomastia from | Spironolactone |
| Most effective emergency contraception | Copper IUD (within 5 days) |
| 5α-reductase inhibitor | Finasteride (BPH + male pattern baldness) |
| GnRH agonist continuous use | Suppresses FSH/LH (paradox!) |
| Prolactinoma drug | Bromocriptine or Cabergoline |
| Diabetes insipidus treatment | Desmopressin (DDAVP) |
| SGLT-2 inhibitor benefit beyond glucose | Heart failure + kidney protection |
Sources: Katzung's Basic & Clinical Pharmacology 16th Ed. | Lippincott Illustrated Reviews: Pharmacology | Goodman & Gilman's The Pharmacological Basis of Therapeutics - with KD Tripathi-style approach
This is a shared conversation. Sign in to Orris to start your own chat.