Teach me every aspect of blood test CBC and it's significance and ddiagnosis
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive data from multiple authoritative textbooks. Let me compile everything into a thorough, well-organized answer.
Complete Blood Count (CBC): A Comprehensive Guide
The CBC is the single most ordered laboratory test in clinical medicine. It quantifies the cellular elements of blood — red cells, white cells, and platelets — and derives calculated indices that help classify disease. Modern automated analyzers provide 20+ parameters in minutes from a 3–5 mL EDTA-anticoagulated venous blood sample.
1. How the CBC is Performed
Blood is collected in an EDTA (purple-top) tube, which chelates calcium and prevents clotting. Automated hematology analyzers use two primary technologies:
- Electrical impedance (Coulter principle): Cells passing through an aperture displace electrolyte, generating a pulse proportional to cell volume.
- Light scatter (flow cytometry): Laser light hitting each cell produces forward scatter (cell size) and side scatter (internal complexity/granularity), used to generate the 5-part differential.
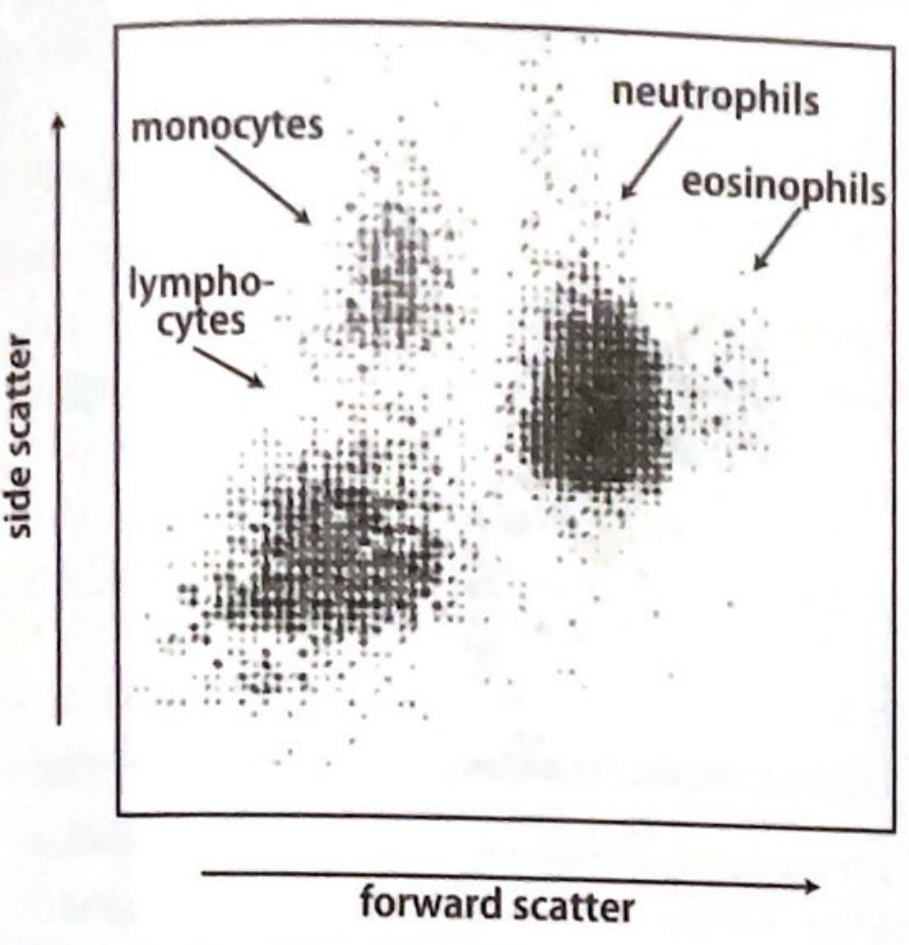
The scatter plot above shows how the analyzer separates leukocyte populations — neutrophils (large, high granularity) appear upper-right; lymphocytes (small, low granularity) lower-left; monocytes between them.
2. Components of the CBC
The CBC has three major compartments: Red Cell Parameters, White Cell Parameters, and Platelet Parameters.
🔴 Part A: Red Blood Cell (RBC) Parameters
2.1 Hemoglobin (Hgb/Hb)
| Parameter | Normal Range |
|---|---|
| Hgb (Female) | 12–16 g/dL |
| Hgb (Male) | 13.5–17.5 g/dL |
Hemoglobin is the most clinically important red cell parameter. It is measured by the cyanohemoglobin (HiCN) method — blood is lysed and converted to a stable chromogen measured spectrophotometrically at 540 nm. Note: HiCN does not detect sulfhemoglobin (SHb). Lipemia and paraproteinemia can falsely elevate Hgb by increasing turbidity.
Clinical significance:
- Anemia = Hgb < 12 g/dL (females) or < 13.5 g/dL (males). Pallor of conjunctival mucosa generally indicates Hgb < 9 g/dL; failure of palmar creases to redden indicates Hgb ≤ 7–8 g/dL.
- Polycythemia/Erythrocytosis = Hgb elevated, may indicate primary (polycythemia vera) or secondary causes (renal carcinoma, hepatocellular carcinoma, high altitude, COPD, androgens, exogenous EPO, postrenal transplant, polycystic kidney disease).
2.2 Hematocrit (Hct / PCV)
| Parameter | Normal Range |
|---|---|
| Hct (Female) | 36–48% |
| Hct (Male) | 40–52% |
The hematocrit is the fraction of blood volume occupied by red cells. In automated analyzers, Hct = MCV × RBC / 10 (calculated, not directly spun).
2.3 RBC Count
| Parameter | Normal Range |
|---|---|
| RBC (Female) | 4.0–5.4 × 10⁶/μL |
| RBC (Male) | 4.5–6.0 × 10⁶/μL |
Direct count of red blood cells per microliter. Used to calculate MCV, MCH, and MCHC.
2.4 Red Cell Indices
These calculated parameters are critical for classifying anemia:
| Index | Formula | Normal Range | What it measures |
|---|---|---|---|
| MCV | Hct / RBC (× 10) | 81–99 fL | Average red cell volume (size) |
| MCH | Hgb / RBC | 30–34 pg | Average Hgb per red cell (weight) |
| MCHC | (Hgb / Hct) × 100 | 30–36 g/dL | Average Hgb concentration per red cell |
| RDW-CV | SD of MCV / Mean MCV | 12–15% | Variability in RBC size (anisocytosis) |
| RDW-SD | 37–47 fL | Standard deviation of MCV distribution |
Clinical pearls on indices:
- High MCV (macrocytosis) → B12/folate deficiency, hypothyroidism, alcohol, liver disease, reticulocytosis, drugs (hydroxyurea, methotrexate)
- Low MCV (microcytosis) → iron deficiency anemia (IDA), thalassemia, anemia of chronic disease (some)
- High MCHC → hereditary spherocytosis, cold agglutinins, lipemic specimens
- RDW high in IDA, normal in thalassemia — a key distinguishing point: thalassemia minor produces uniform microcytosis (low MCV, normal RDW); IDA produces variable microcytosis (low MCV, elevated RDW)
- Pronounced reticulocytosis can raise the MCV (reticulocytes are larger than mature RBCs)
Anemia Classification by MCV:
| MCV | Type | Common Causes |
|---|---|---|
| < 80 fL | Microcytic | IDA, thalassemia, sideroblastic anemia, anemia of chronic disease |
| 80–100 fL | Normocytic | Acute blood loss, hemolysis, renal failure, bone marrow failure |
| > 100 fL | Macrocytic | B12/folate deficiency, alcohol, hypothyroidism, MDS |
2.5 Reticulocyte Count
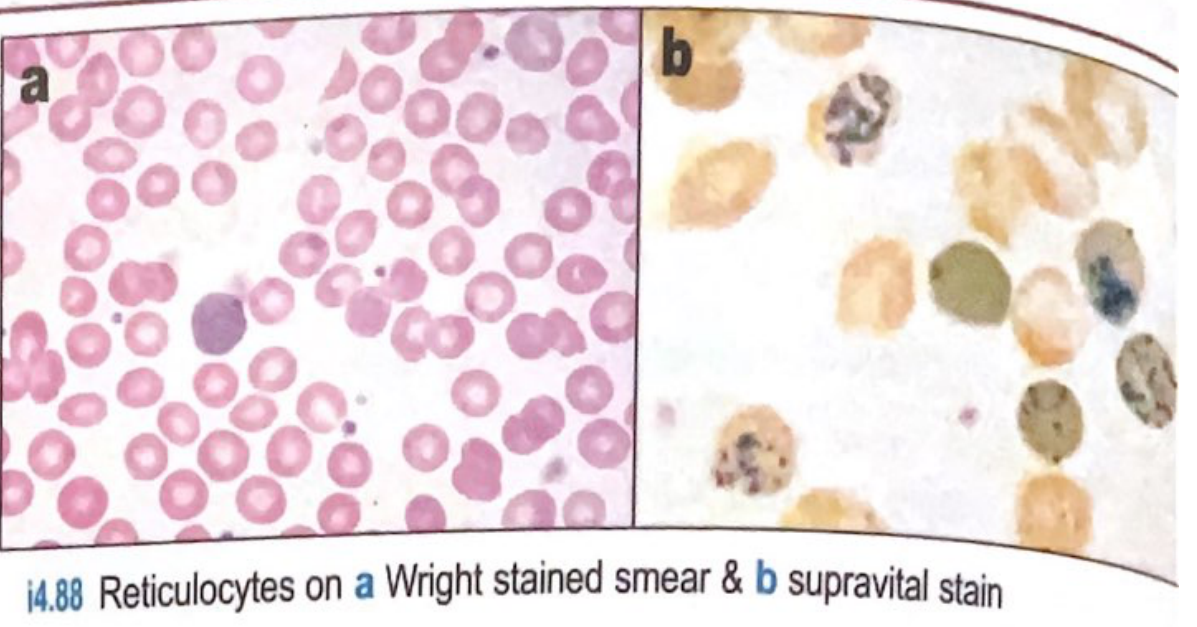
Reticulocytes on a Wright-stained smear (a) appear as slightly larger cells with bluish tinge; on supravital stain (b) with new methylene blue, residual ribosomal RNA is highlighted as blue precipitate.
| Parameter | Normal Range |
|---|---|
| Reticulocyte % | 0.5–1.5% |
| Absolute reticulocyte count | 20,000–100,000/μL |
| Reticulocyte Production Index (RPI) | 0.5–2.5 |
Reticulocytes are immature RBCs that still contain ribosomal RNA (survive 1–2 days in circulation). They are stained with supravital dyes (new methylene blue or azure B).
Formulas:
- Absolute reticulocyte count = % reticulocytes × RBC count
- Corrected reticulocyte count (CRC) = % retics × (patient Hct / 45)
- RPI = CRC / maturation factor (maturation factor: 1.0 at Hct 36–45%, 1.5 at 26–35%, 2.0 at 16–25%, 2.5 at ≤15%)
RPI interpretation:
- RPI > 3: Adequate marrow response → hemorrhage or hemolysis (hyperproliferative)
- RPI < 2: Inadequate marrow response → hypoproliferative anemia (iron deficiency, B12/folate, aplastic anemia, renal failure)
Immature Reticulocyte Fraction (IRF): Automated analyzers measure this using RNA-binding fluorescent dyes — brighter signal = more immature reticulocyte. High IRF with low reticulocyte count = marrow recovery.
Reticulocyte Hemoglobin Concentration (CHr / Ret-He): Reflects availability of iron to the marrow; useful for detecting functional iron deficiency even before morphological changes appear.
2.6 RDW — Red Cell Distribution Width
RDW measures anisocytosis (variation in RBC size). It is one of the most discriminating features between:
| Condition | MCV | RDW |
|---|---|---|
| Iron deficiency anemia | Low | High |
| Thalassemia minor | Low | Normal |
| Anemia of chronic disease | Low-normal | Normal |
| B12/folate deficiency | High | High |
| Mixed deficiency | Normal ("dimorphic") | Very high |
⚪ Part B: White Blood Cell (WBC) Parameters
2.7 Total WBC Count
Normal: 4,000–11,000 cells/mm³
Particles > 36 fL are counted as leukocytes. The analyzer uses light scatter to produce a 5-part differential.
Leukocytosis (WBC > 10,000/mm³):
Caused by reactive processes or primary hematologic malignancy. Always determine which cell type is elevated:
| Cell Type Elevated | Common Causes |
|---|---|
| Neutrophilia | Bacterial infection, trauma, burns, drugs (corticosteroids, G-CSF), leukemia, rheumatic disorders, neoplasms |
| Eosinophilia | Parasitic infections, allergic diseases (asthma, atopic dermatitis), drug reactions, myeloproliferative disorders, malignancy |
| Basophilia | CML, polycythemia vera, myeloid metaplasia, allergic reactions, hypothyroidism, chronic hemolytic anemia, post-splenectomy |
| Monocytosis | TB/chronic infections, sarcoidosis, neoplasms, GI inflammatory diseases, recovering from marrow suppression |
| Lymphocytosis | Viral infections (EBV, CMV, HIV), CLL, pertussis, other lymphoid neoplasms |
Leukopenia (WBC < 4,000/mm³):
| Cell Type Decreased | Common Causes |
|---|---|
| Neutropenia | Overwhelming bacterial/viral infection, drug reactions, ionizing radiation, aplastic anemia, hematopoietic diseases, hypersplenism, autoimmune disease |
| Lymphopenia | HIV, immunosuppressants, corticosteroids, genetic immunodeficiencies |
| Eosinopenia | Acute physical stress, corticosteroid use |
2.8 The 5-Part Differential
The differential counts each leukocyte type as a percentage, and the absolute count (total WBC × %) is what matters clinically.
| Cell | Normal % | Absolute Normal | Key Roles |
|---|---|---|---|
| Neutrophils (segs + bands) | 50–70% | 1800–7700/μL | First-line defense vs. bacteria; phagocytosis |
| Lymphocytes | 20–40% | 1000–4800/μL | Adaptive immunity (T cells, B cells, NK cells) |
| Monocytes | 2–8% | 200–800/μL | Phagocytosis, antigen presentation, become macrophages |
| Eosinophils | 1–4% | 100–400/μL | Parasitic defense, allergic/hypersensitivity reactions |
| Basophils | 0–1% | 0–100/μL | IgE-mediated allergy, contain histamine and heparin |
Absolute Neutrophil Count (ANC):
ANC = Total WBC × (% bands + % segs) / 100
- ANC < 1500/μL = neutropenia
- ANC < 500/μL = severe neutropenia → high risk of life-threatening bacterial infections
"Left shift" — increased band neutrophils (immature forms) in peripheral blood indicates bone marrow responding to acute bacterial infection or stress. The Immature Granulocyte (IG) fraction on modern analyzers (sum of metamyelocytes, myelocytes, promyelocytes) has proven superior to manual band counting for diagnosing sepsis.
"Leukemoid reaction" — WBC > 50,000/mm³ with a marked left shift, resembling leukemia but reactive. Caused by severe infection, malignancy, hemolysis, or drugs.
🟡 Part C: Platelet Parameters
2.9 Platelet Count
Normal: 150,000–400,000/mm³ (150–400 × 10⁹/L)
| Condition | Platelet Count | Significance |
|---|---|---|
| Thrombocytopenia | < 150,000/mm³ | Bleeding risk increases below 50,000; spontaneous hemorrhage < 20,000 |
| Normal | 150,000–400,000 | — |
| Thrombocytosis | > 400,000/mm³ | May be reactive or primary (essential thrombocythemia) |
Important caveat: Before diagnosing thrombocytopenia, always examine the peripheral smear for platelet clumping (EDTA-induced pseudothrombocytopenia) — repeat with sodium citrate tube if suspected.
Causes of thrombocytopenia:
- Decreased production: aplastic anemia, myelophthisis, chemotherapy, alcohol, B12/folate deficiency
- Increased destruction: ITP, TTP/HUS, DIC, heparin-induced thrombocytopenia (HIT — typically drops to 50,000–70,000 within 5–15 days of heparin)
- Sequestration: hypersplenism
Causes of thrombocytosis:
- Reactive: infection, iron deficiency, post-splenectomy, inflammatory disorders, hemorrhage
- Primary: essential thrombocythemia (ET), CML, polycythemia vera
Severe thrombocytopenia + DIC — prompt peripheral smear for acute promyelocytic leukemia (APL); leukemic cells may be sparse in blood but DIC can be the presenting sign.
2.10 Mean Platelet Volume (MPV)
Normal: ~7.5–12.5 fL
- High MPV → large platelets from marrow, indicating peripheral destruction/consumption (e.g., ITP, HIT) — the marrow is producing young, large platelets to compensate
- Low MPV → suggests decreased production (aplastic anemia, marrow infiltration)
Immature Platelet Fraction (IPF): Similar to IRF for reticulocytes, IPF reflects newly produced (thrombopoiesis-active) platelets. High IPF + low count = peripheral destruction; low IPF + low count = production failure.
3. Additional / Extended CBC Parameters
| Parameter | Significance |
|---|---|
| Schistocytes (auto-enumerated) | RBC fragments in platelet channel → microangiopathic hemolytic anemia (TTP, HUS, DIC) |
| Immature Granulocyte (IG) fraction | Sum of metamyelocytes + myelocytes + promyelocytes; superior to bands for sepsis diagnosis |
| Immature Reticulocyte Fraction (IRF) | Marrow recovery indicator |
| Ret-He / CHr | Functional iron availability in marrow |
| NRBC (nucleated RBCs) | Normally absent; presence suggests severe anemia with extramedullary hematopoiesis, asplenia, or leukemia |
4. Anemia: CBC-Based Diagnostic Algorithm
Low Hemoglobin → Is it hypoproliferative or hyperproliferative?
↓
Check RPI / Reticulocyte count
↓
RPI < 2 (hypoproliferative) RPI > 3 (hyperproliferative)
→ Check MCV: → Hemolysis or blood loss
Low MCV → IDA, thalassemia, → Check LDH, bilirubin,
sideroblastic anemia haptoglobin, peripheral smear
Normal MCV → ACD, aplastic,
renal failure
High MCV → B12/folate, alcohol,
hypothyroidism, MDS
5. Key CBC Patterns and Their Diagnoses
| CBC Pattern | Likely Diagnosis |
|---|---|
| Low Hgb + Low MCV + High RDW | Iron deficiency anemia |
| Low Hgb + Low MCV + Normal RDW | Thalassemia minor |
| Low Hgb + High MCV + High RDW | B12 or folate deficiency |
| Pancytopenia (↓ WBC + ↓ Hgb + ↓ platelets) | Aplastic anemia, MDS, leukemia, B12 deficiency, hypersplenism |
| Leukocytosis + left shift + fever | Bacterial infection / sepsis |
| Leukocytosis + eosinophilia | Parasitic infection, allergy, drug reaction |
| Very high WBC (>100,000) + blasts | Leukemia (CML, ALL, AML) |
| Thrombocytopenia + schistocytes + anemia | TTP/HUS, DIC |
| Thrombocytopenia alone + large platelets | ITP |
| Thrombocytopenia + falling Hgb after heparin | HIT |
| Basophilia + leukocytosis | CML (until proven otherwise) |
| Lymphocytosis + smudge cells (on smear) | CLL |
| High RBC + high Hgb + low EPO | Polycythemia vera |
| High platelet + JAK2 mutation | Essential thrombocythemia |
6. Race, Sex, and Age Effects on Reference Ranges
CBC values are not universal. Important variations (from Tietz Textbook of Laboratory Medicine):
- Hematocrit, Hgb, and MCV are lower in African Americans than Caucasians
- Hematocrit, Hgb, MCH, MCHC, and MPV are lower in Asians than Caucasians
- Children have higher WBC and lymphocyte counts relative to adults
- Pregnant women have physiological dilutional anemia (expanded plasma volume)
- Elderly patients may have slightly lower RBC counts and slightly altered WBC differential
7. Common Pitfalls and Spurious Results
| Pitfall | Cause | What is falsely affected |
|---|---|---|
| Pseudothrombocytopenia | EDTA-induced platelet clumping | Falsely low platelet count → repeat with citrate |
| Falsely high Hgb | Lipemia, paraproteinemia (turbidity) | HiCN method overestimates |
| Falsely high MCV | Pronounced reticulocytosis, hyperglycemia, cold agglutinins | Agglutinated cells counted as one large cell |
| Falsely high MCHC | Spherocytosis, cold agglutinins, lipemia | |
| WBC count falsely elevated | Nucleated RBCs (NRBCs), cryoglobulin, platelet clumps | Uncorrected WBC inflated |
| Giant platelets misclassified as RBCs | Rare congenital macrothrombocytopenia | Apparent anemia on analyzer |
8. When to Order a CBC
The CBC is indicated in virtually every clinical encounter involving:
- Suspected or known anemia (fatigue, pallor, dyspnea)
- Infection workup (fever, suspected sepsis)
- Bleeding or bruising disorders
- Preoperative assessment
- Monitoring chemotherapy, radiation therapy, or myelosuppressive drugs
- Diagnosis and monitoring of hematologic malignancies
- Evaluation of systemic inflammatory disorders
- Screening in pregnancy, pediatric well-visits
- Baseline prior to starting medications that affect marrow (e.g., clozapine, carbamazepine, methotrexate)
Summary Table: All CBC Parameters at a Glance
| Parameter | Normal | ↑ Means | ↓ Means |
|---|---|---|---|
| Hgb | 12–17.5 g/dL | Polycythemia, dehydration | Anemia (multiple causes) |
| Hct | 36–52% | Same | Same |
| RBC | 4.0–6.0 ×10⁶/μL | Polycythemia | Anemia |
| MCV | 81–99 fL | Macrocytic anemia | Microcytic anemia |
| MCH | 30–34 pg | Macrocytosis | Hypochromia, microcytosis |
| MCHC | 30–36 g/dL | Spherocytosis | Hypochromic anemia |
| RDW | 12–15% | Mixed deficiency, IDA | Not clinically significant |
| Reticulocyte % | 0.5–1.5% | Hemolysis, recovery | Hypoproliferative |
| WBC | 4,000–11,000/mm³ | Infection, leukemia | Marrow failure, viral, drugs |
| Neutrophils | 50–70% / >1800 abs | Infection, stress | Aplasia, viral, drugs, autoimmune |
| Lymphocytes | 20–40% | Viral infections, CLL | HIV, immunosuppression |
| Monocytes | 2–8% | TB, chronic infection | Rare |
| Eosinophils | 1–4% | Parasites, allergy, CML | Steroids, acute stress |
| Basophils | 0–1% | CML, allergy, PV | Non-specific |
| Platelets | 150–400 ×10³/mm³ | ET, reactive, post-splenectomy | ITP, TTP, DIC, HIT, aplasia |
| MPV | 7.5–12.5 fL | Peripheral destruction (ITP) | Production failure |
Sources:
- Goldman-Cecil Medicine, 26th ed., Chapter 144 (Approach to Anemia; Complete Blood Counts)
- Quick Compendium of Clinical Pathology, 5th ed., Sections 4.4.1–4.4.3 (Methods: RBC, Leukocyte, Platelet Indices)
- Textbook of Family Medicine, 9th ed., Chapter 14 (White Blood Cells, Platelets, Erythrocytosis)
- Tietz Textbook of Laboratory Medicine, 7th ed. (Reference intervals, analyzer technology)
RFT and it's components and significance
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.