a 60 year old female come to opd with hostory of htn and nasal bleed now the patient having bp 160/100 and the nose bleed is continue please suggest me the treatment for stopping the bleeding
epistaxis management hypertension
Epistaxis Management in a 60-Year-Old Hypertensive Female (BP 160/100 mmHg)
Step 1 - Initial Assessment (Do This Immediately)
- Assess the airway - ensure she can breathe and is not aspirating blood
- Sit her upright, leaning slightly forward (prevents blood from flowing down the throat and being swallowed/aspirated)
- Pinch her nose and let her spit blood into a bowl - do NOT ask her to tilt the head back
- Establish IV access
- Order baseline labs: CBC, PT/INR, aPTT (check for coagulopathy); also a renal panel given HTN history
- Check medication history - is she on aspirin, warfarin, clopidogrel, or NSAIDs?
Note: An elevated BP upon presentation is very common in epistaxis patients, and studies have NOT established a direct causal link between hypertension and epistaxis. However, elevated BP is associated with persistent bleeding. - Rosen's Emergency Medicine, p. 920
Step 2 - First-Line Hemostasis (Do These Together)
A. Direct Pressure
- Ask the patient (or do it yourself) to firmly compress the soft cartilaginous part of the nose (not the bony bridge) for 10 to 15 minutes continuously without releasing
- A nose clip is superior to manual pressure alone
B. Topical Vasoconstrictor Immediately
- Instil 2 sprays of oxymetazoline 0.05% (Afrin/Otrivin) into the affected nostril before applying pressure
- Alternatively, use a cotton pledget soaked in phenylephrine + 4% lidocaine solution - this both decongests and anesthetizes
- These topical vasoconstrictors reduce mucosal blood flow and help achieve hemostasis
Step 3 - Identify the Bleeding Site
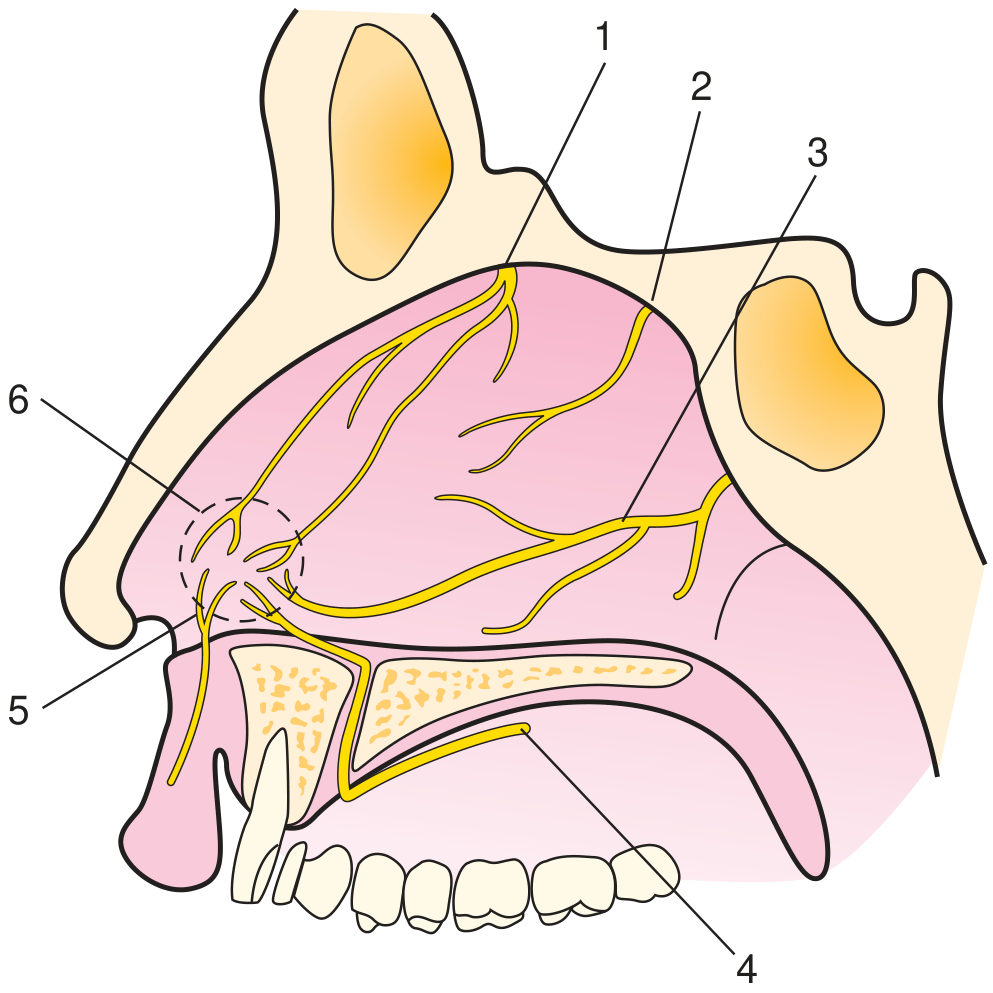
- Anterior epistaxis (90% of cases): Bleeding from Kiesselbach's plexus at the anteroinferior nasal septum - visible on inspection, usually unilateral, easier to control
- Posterior epistaxis (10%): More severe, older adults, bleeds from both nostrils or drains into the throat - suspect if anterior measures fail
Step 4 - Escalating Treatment for Active Bleeding
A. Chemical Cautery (if bleeding site is visible)
- Apply a silver nitrate stick to the bleeding point
- Cauterize from the periphery inward, superior to inferior
- Do NOT apply pressure >15 seconds at one spot (risk of septal damage)
- Do NOT cauterize both sides of the septum simultaneously (risk of necrosis)
- Likely to fail during active bleeding - secure hemostasis first, then cauterize
B. Topical Tranexamic Acid (excellent adjunct, especially in this patient)
- Soak a nasal pledget in 500 mg tranexamic acid (IV solution applied topically) and place in the nostril
- Or atomize it into the nasal cavity
- A systematic review found moderate-quality evidence: topical TXA reduces immediate bleeding at 10 minutes and re-bleeding at 7-10 days compared to standard care alone, with no significant adverse events
- Particularly effective in patients on antiplatelet drugs - Rosen's Emergency Medicine, p. 920
C. Topical Thrombogenic Agents
- If cautery is not successful, apply absorbable gelatin sponge (Gelfoam) or absorbable knitted fabric (Surgicel) to the bleeding area
D. Anterior Nasal Packing (if above fail)
- Use a pre-formed pack: Merocel (polyvinyl acetal) nasal tampon or an inflatable Rapid Rhino balloon (coated in procoagulant material)
- Coat the pack in antibiotic ointment, insert along the floor of the nose (horizontally, not upward)
- Inflate Rapid Rhino balloon with air after seating; self-lubricating
- If unilateral pack fails, insert a second pack in the opposite nostril
- Once packed, observe for continued bleeding
Step 5 - If Anterior Packing Fails (Posterior Epistaxis)
- Insert a double balloon catheter (e.g., Epistat device): inflate the posterior balloon first, seat it by pulling anteriorly, then inflate the anterior balloon
- If no commercial device is available, a Foley catheter (12-14 Fr) can be inserted into the nasopharynx, inflated with 5-7 mL water, pulled anteriorly to tamponade the posterior choana
- Admit the patient for monitoring - posterior packing carries risk of hypoxia, vasovagal response, and pressure necrosis
- Urgent ENT consultation is required
Step 6 - Managing the Blood Pressure (BP 160/100)
- Do NOT aggressively lower BP acutely in a setting of active bleeding - the anxiety and pain of the nosebleed itself raise BP, and it usually falls once bleeding is controlled
- Once hemostasis is achieved, reassess BP
- If BP remains elevated:
- Short-acting oral agent: Amlodipine 5 mg or Labetalol (if no contraindication)
- Avoid aggressive IV antihypertensives - sudden hypotension can worsen end-organ perfusion in a 60-year-old
- Ensure the patient's chronic antihypertensive medications (if any) are continued
- The goal is controlled BP reduction over hours, not minutes
Step 7 - Refractory Cases (If All Above Fail)
- Endovascular embolization of the sphenopalatine artery - success rate >80%, less invasive, preferred in patients with multiple comorbidities
- Surgical ligation of the sphenopalatine artery (endoscopic approach preferred)
- Anterior/posterior ethmoidal artery ligation for superior bleeding - Rosen's Emergency Medicine, p. 921
Antibiotics?
Summary Algorithm
| Step | Action |
|---|---|
| 1 | Sit forward, pinch nose, IV access, labs |
| 2 | Oxymetazoline spray + direct pressure x 15 min |
| 3 | Examine - anterior vs posterior source |
| 4a | Silver nitrate cautery (if site visible) |
| 4b | Topical tranexamic acid 500 mg pledge |
| 4c | Gelfoam/Surgicel topical agents |
| 4d | Anterior nasal packing (Merocel/Rapid Rhino) |
| 5 | Posterior packing + ENT consult + admit |
| 6 | Control BP after hemostasis (not before) |
| 7 | Embolization or surgical ligation if refractory |
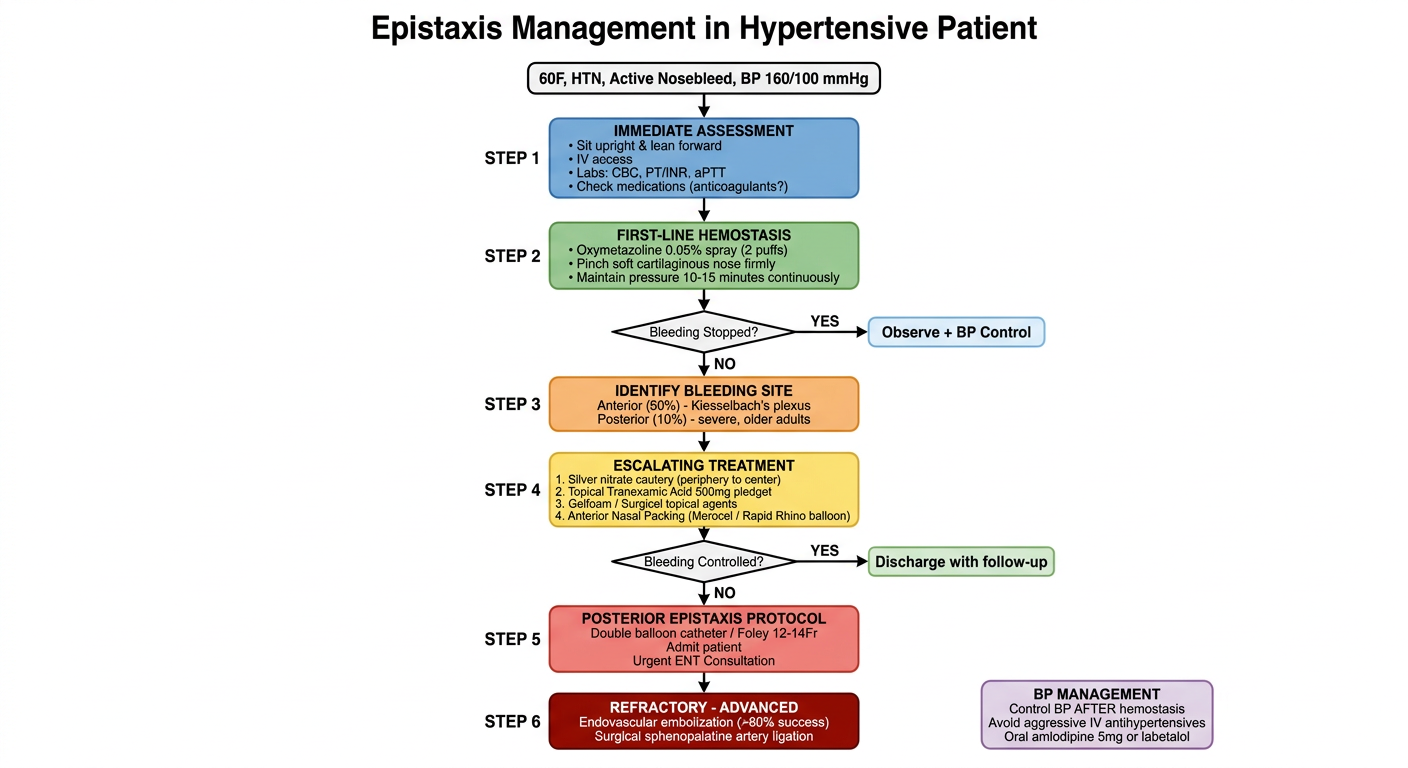
explain this procedure in diagram form
A clear, professional medical flowchart diagram titled "Epistaxis Management in Hypertensive Patient" showing a step-by-step clinical algorithm. The diagram flows top to bottom with labeled boxes and arrows. Include these steps in order: TOP: Patient box - "60F, HTN, Active Nosebleed, BP 160/100 mmHg" STEP 1 box (blue): "IMMEDIATE ASSESSMENT" with bullet points: Sit upright & lean forward, IV access, Labs: CBC, PT/INR, aPTT, Check medications (anticoagulants?) STEP 2 box (green): "FIRST-LINE HEMOSTASIS" with bullet points: Oxymetazoline 0.05% spray (2 puffs), Pinch soft cartilaginous nose firmly, Maintain pressure 10-15 minutes continuously Decision diamond: "Bleeding Stopped?" YES arrow → "Observe + BP Control" box. NO arrow continues downward. STEP 3 box (orange): "IDENTIFY BLEEDING SITE" with: Anterior (90%) - Kiesselbach's plexus, Posterior (10%) - severe, older adults STEP 4 box (yellow): "ESCALATING TREATMENT" with numbered list: 1. Silver nitrate cautery (periphery to center), 2. Topical Tranexamic Acid 500mg pledget, 3. Gelfoam / Surgicel topical agents, 4. Anterior Nasal Packing (Merocel / Rapid Rhino balloon) Decision diamond: "Bleeding Controlled?" YES → "Discharge with follow-up". NO → continues STEP 5 box (red): "POSTERIOR EPISTAXIS PROTOCOL" with: Double balloon catheter / Foley 12-14Fr, Admit patient, Urgent ENT Consultation STEP 6 box (dark red): "REFRACTORY - ADVANCED" with: Endovascular embolization (>80% success), Surgical sphenopalatine artery ligation BOTTOM right box (purple): "BP MANAGEMENT" note: Control BP AFTER hemostasis, Avoid aggressive IV antihypertensives, Oral amlodipine 5mg or labetalol Use color-coded boxes, clear arrows, clean medical illustration style, white background, legible sans-serif font.
- Initial Assessment - stabilize, IV access, labs
- First-Line Hemostasis - oxymetazoline spray + 15 minutes of firm pinching
- Check if bleeding stopped - if yes, observe and manage BP; if no, escalate
- Identify the bleeding source - anterior (90%) vs posterior (10%)
- Escalating treatment - cautery → tranexamic acid → Gelfoam → anterior nasal packing
- Check again - if controlled, discharge with follow-up; if not, move to posterior protocol
- Posterior epistaxis protocol - balloon catheter, admit, ENT consult
- Refractory cases - embolization or surgical ligation
- BP management - always addressed after hemostasis, not before