Ostiomilitis
Reading File
Finding Sources
Searching PubMed
"osteomyelitis"[MeSH Terms] AND ("diagnosis" OR "treatment")
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the information needed for a thorough answer. Here is a complete overview of osteomyelitis:
Osteomyelitis
Osteomyelitis is inflammation of bone and bone marrow, virtually always caused by infection. It can be acute, subacute, or chronic, and may involve any bone in the body.
Definition and Classification
| Type | Key Feature |
|---|---|
| Acute | First episode, <2 weeks; neutrophilic inflammation |
| Subacute | 2 weeks - 3 months; Brodie abscess |
| Chronic | >3 months; sequestrum + involucrum formation, sinus tracts |
Routes of Infection
Organisms reach bone by three mechanisms (Robbins & Kumar Basic Pathology):
- Hematogenous spread - most common in children; bacteria seed the metaphysis during bacteremia
- Contiguous spread - from adjacent soft tissue infection (e.g., diabetic foot ulcer)
- Direct implantation - open fractures, surgery, penetrating wounds
Why the Metaphysis?
The diagram below illustrates the key mechanism - slow sinusoidal blood flow at the metaphysis combined with microtrauma allows bacterial colonies to seed during bacteremia:
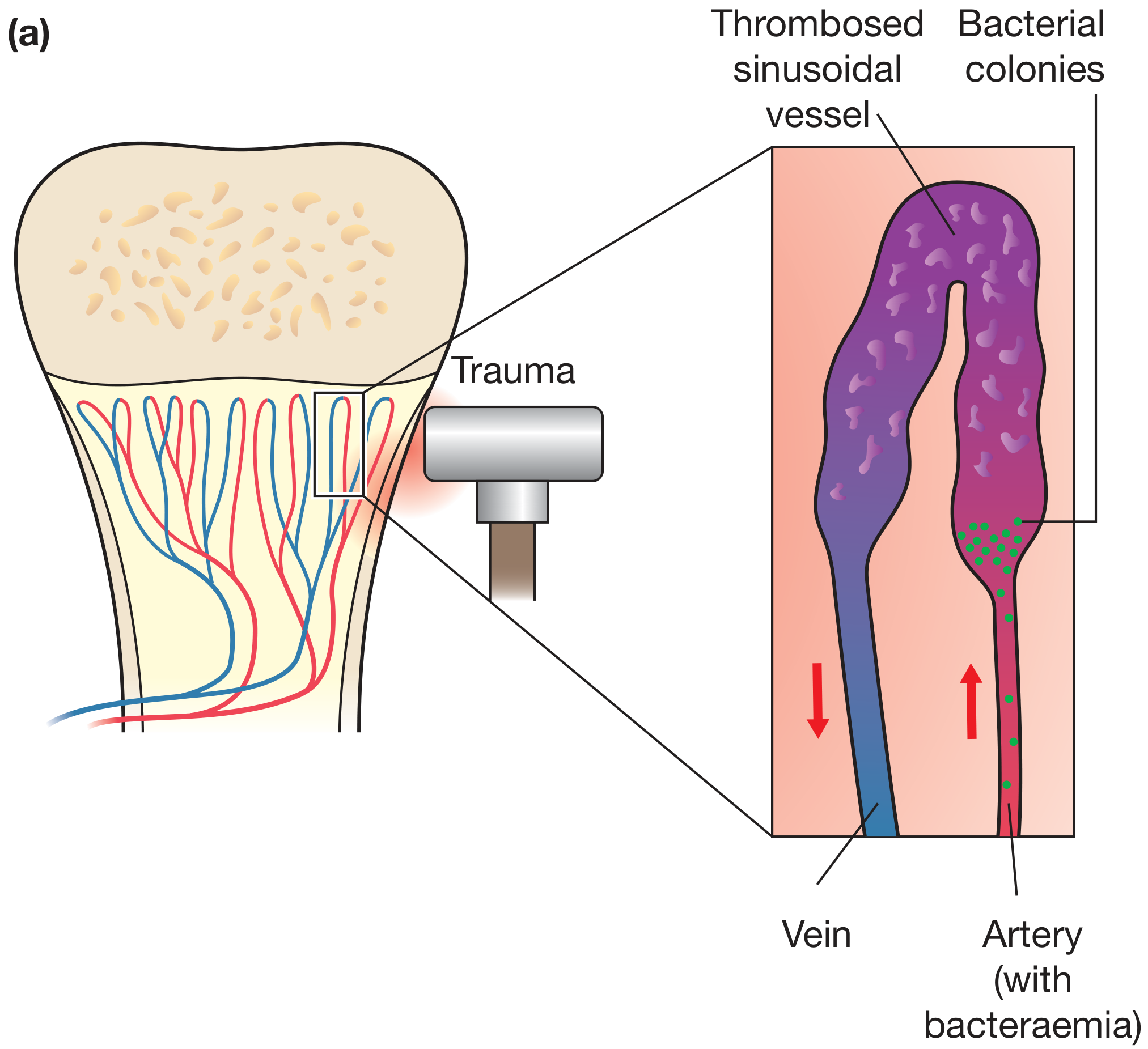
Hematogenous osteomyelitis: trauma slows flow in sinusoidal vessels; bacteria from a bacteremic artery seed the area and form colonies - Bailey and Love's Short Practice of Surgery 28e
Microbiology
| Clinical Context | Most Likely Organism(s) |
|---|---|
| Children (all ages) | S. aureus (MRSA predominant in AHO) |
| Neonates | Group B Streptococcus, E. coli |
| Adults with diabetes / open fracture | S. aureus; polymicrobial |
| Sickle cell disease | Salmonella spp., gram-negative organisms |
| Post-surgical / prosthesis | S. aureus, coagulase-negative Staph |
| Immunocompromised | Mycobacteria, fungi (Candida, Aspergillus) |
S. aureus is the single most common pathogen overall. Its cell wall proteins (e.g., MSCRAMM proteins) bind collagen in bone matrix, facilitating adherence. No organism is identified in nearly 50% of cases. - Robbins & Kumar Basic Pathology, p. 779
Pathology and Morphology
Acute Phase (< 48 hours)
- Bacterial proliferation triggers neutrophilic infiltration
- Necrosis of bone cells and marrow
- Bacteria spread through Haversian canals to the periosteum
- Subperiosteal abscess forms (especially in children, where periosteum is loosely attached)
- Periosteal lifting further impairs vascular supply → more necrosis
Chronic Phase (after ~1 week)
- Chronic inflammatory cells (lymphocytes, plasma cells) release cytokines
- Osteoclastic resorption + fibrous ingrowth
- Sequestrum: dead, devascularized bone fragment - the hallmark of chronicity
- Involucrum: shell of new reactive periosteal bone surrounding the sequestrum
The photograph below shows a resected femur from a patient with draining chronic osteomyelitis - the involucrum (red arrow) contains the sequestrum (yellow arrow):
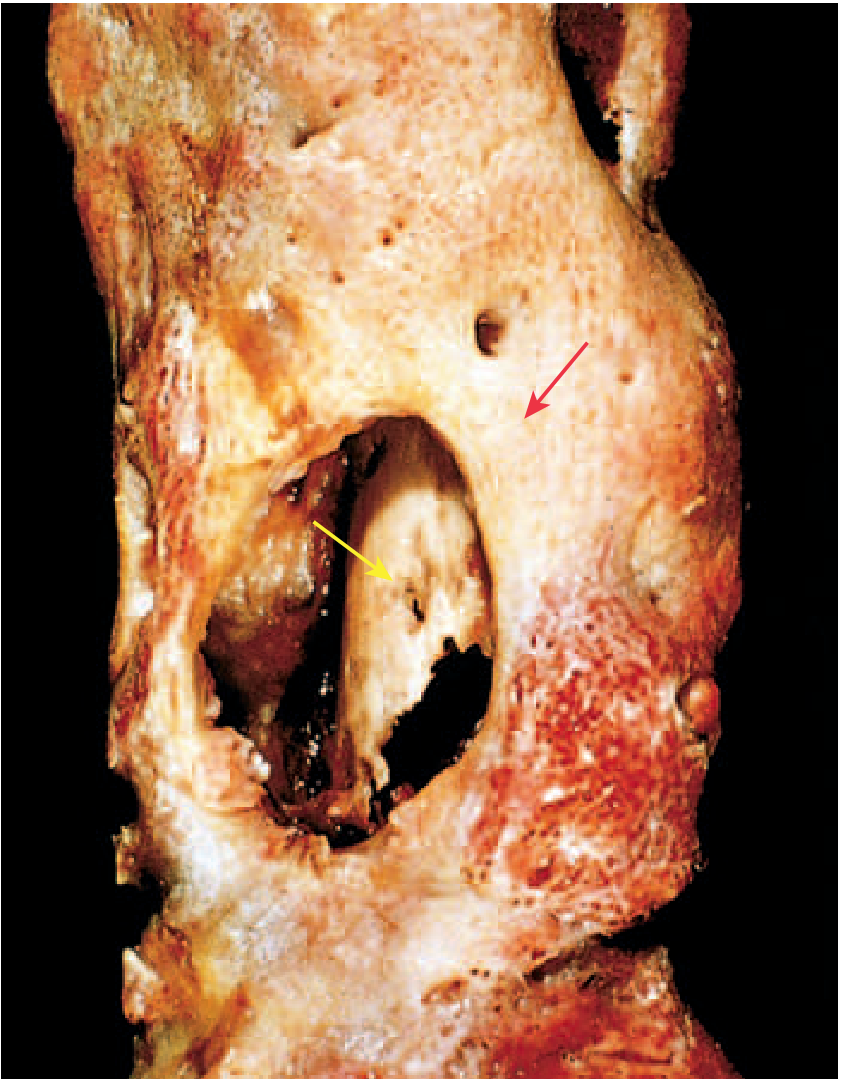
FIG. 19.13 Resected femur: involucrum (red arrow) = new bone shell; sequestrum (yellow arrow) = necrotic original cortex - Robbins & Kumar Basic Pathology
Pus may track through gaps in the involucrum (called cloacae) and form sinus tracts to the skin surface.
A special subacute form is the Brodie abscess - a well-defined lytic lesion with a sclerotic rim, most common in the distal tibia metaphysis of adolescents.
Clinical Features
Acute osteomyelitis:
- Fever, rigors, malaise, anorexia
- Point tenderness over the infected bone - the most reliable physical finding
- Localized warmth, swelling, erythema
- In children: sudden limp or refusal to bear weight on the affected limb
Chronic osteomyelitis:
- Often low-grade or no fever
- Persistent pain
- Palpable involucrum
- Draining sinus tracts to the skin
- Intermittent acute flare-ups after years of dormancy
Vertebral osteomyelitis (Pott's disease / pyogenic spondylodiscitis):
- Severe focal back pain not relieved by rest
- Can complicate spinal procedures/injections, or arise from hematogenous spread
- Risk of spinal cord compression
- Diskitis (involvement of the avascular intervertebral disc) commonly coexists in adults
Investigations
| Test | Findings / Notes |
|---|---|
| WBC, ESR, CRP | Elevated in acute; ESR/CRP more sensitive than WBC |
| Blood cultures | Positive in ~40% of pediatric AHO |
| Plain X-ray | Lytic lesion + periosteal reaction; lags 10-14 days behind disease |
| MRI (gold standard) | Highest sensitivity and specificity; shows bone edema, abscess, extent of involvement; mandatory for vertebral OM |
| CT | Defines cortical destruction, detects sequestra; useful in post-trauma/post-op |
| Ultrasound | Useful in infants/children; detects subperiosteal abscess; guides aspiration |
| Bone scintigraphy | Useful for multifocal disease, especially in neonates |
| Bone biopsy + culture | Most specific for identifying pathogen; required in most adults |
Radiographic changes typically appear 10-14 days after symptom onset - Grainger & Allison's Diagnostic Radiology
Management
Antibiotics
- Empirical therapy targets S. aureus; adjust after culture results
- Nafcillin/oxacillin (MSSA) or vancomycin (MRSA) are first-line IV agents
- Transition from IV to oral therapy is appropriate once the patient is improving clinically and hematologically
- Duration: typically 4-6 weeks total; uncomplicated pediatric cases may be treated with shorter IV courses followed by oral antibiotics
- Local MRSA prevalence and Panton-Valentine leukocidin (PVL) status affect choice
Surgery
Indications:
- Abscess drainage (pus must be drained)
- Debridement of sequestrum and necrotic bone
- Spinal cord compression or progressive deformity (vertebral OM)
- Recurrence after adequate treatment
- Retained prosthetic device with acute infection (debridement + irrigation + retention for early prosthetic joint infection)
Adjuncts
- Rest / splintage of the affected limb
- Adequate analgesia
- In chronic osteomyelitis: reconstruction (bone grafting, flap coverage) may be needed after eradication of infection
Complications
- Chronic osteomyelitis (5-25% of acute cases fail to resolve)
- Pathologic fracture
- Septic arthritis (especially when metaphysis is intracapsular, e.g., hip in neonates)
- Growth arrest / limb deformity in children (if epiphysis involved)
- Bacteremia and sepsis
- Brain abscess, meningitis, endocarditis (hematogenous spread of ongoing infection)
- Secondary (reactive) amyloidosis in long-standing chronic OM
- Squamous cell carcinoma arising in a chronic sinus tract (Marjolin's ulcer variant)
- Sarcoma in chronically infected bone (rare)
Special Forms
Mycobacterial (TB) Osteomyelitis:
- Affects ~1-3% of TB patients; usually hematogenous from an active visceral focus
- Spine involved in 40% of cases (Pott's disease) - infection spreads across disc space to adjacent vertebrae, may form a psoas abscess
- Histology: caseating granulomas
- More destructive and harder to control than pyogenic OM
- Robbins & Kumar Basic Pathology
Diabetic Foot Osteomyelitis:
- Most common cause of adult osteomyelitis in high-income countries
- Contiguous spread from ulcers; polymicrobial
- Diagnosis often requires MRI + bone biopsy
Recent Evidence
A 2025 systematic review and meta-analysis (PMID 40607967) identified key risk factors for osteomyelitis development. A 2024 systematic review of 1,118 cases of calcaneal osteomyelitis (PMID 38869983) reported on treatment outcomes in this anatomically complex location. These do not contradict current management principles described above.
Sources:
- Robbins & Kumar Basic Pathology, pp. 778-780 (Pyogenic and Mycobacterial Osteomyelitis)
- Bailey and Love's Short Practice of Surgery 28e, pp. 656-657
- Rosen's Emergency Medicine: Concepts and Clinical Practice (Clinical Features, Subsets, Imaging)
- Grainger & Allison's Diagnostic Radiology (Imaging, Pathology Summary)
This is a shared conversation. Sign in to Orris to start your own chat.