Heapatitis pathology
Reading File
Finding Sources
Finding Sources
Searching PubMed
"hepatitis" AND "pathology"[MeSH Terms]
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I have extensive content from Robbins. Let me now compile the comprehensive answer using all the material gathered.
Hepatitis - Pathology
Based on Robbins, Cotran & Kumar - Pathologic Basis of Disease and Robbins & Kumar Basic Pathology
Overview
"Hepatitis" refers to two distinct contexts:
- Liver diseases caused by hepatotropic viruses (HAV, HBV, HCV, HDV, HEV) that specifically target the liver
- Similar patterns of hepatic injury caused by non-hepatotropic viruses (EBV, CMV, HSV, adenovirus), autoimmune reactions, drugs, and toxins
The inflammatory cells in both acute and chronic viral hepatitis are predominantly cytotoxic T lymphocytes (CD8+ T cells) and NK cells - not the virus itself directly. Morphologic findings overlap across etiologies.
The Hepatitis Viruses - Comparison
| Feature | HAV | HBV | HCV | HDV | HEV |
|---|---|---|---|---|---|
| Genome | ssRNA (+) | Partial dsDNA | ssRNA (+) | ssRNA (-) | ssRNA (+) |
| Family | Picornaviridae | Hepadnaviridae | Flaviviridae | Deltaviridae | Hepeviridae |
| Transmission | Fecal-oral | Parenteral/sexual/perinatal | Parenteral | Parenteral (needs HBV) | Fecal-oral |
| Chronic disease | No | Yes | Yes (~85%) | Yes | No (except immunocompromised) |
| Carrier state | No | Yes | Yes | Yes | No |
| Fulminant hepatitis | 0.1-0.3% | Rare | Very rare | High (superinfection) | High in pregnancy |
Individual Viruses
Hepatitis A (HAV)
- Nonenveloped, positive-strand RNA picornavirus; genus Hepatovirus
- Receptor on hepatocytes: HAVcr-1 (TIM-1)
- Spread by fecal-oral route (contaminated water, food, shellfish)
- Incubation period: 2-6 weeks
- Shed in stool 2-3 weeks before and 1 week after jaundice onset
- NOT cytopathic - liver injury is immune-mediated (CTLs, NK cells)
- Serology: IgM anti-HAV = acute infection marker; IgG anti-HAV = persists for years (lifelong immunity)
- Does not cause chronic hepatitis or carrier state
- Fulminant hepatitis in only 0.1-0.3% (more risk if underlying chronic liver disease)
Hepatitis B (HBV)
Epidemiology: 254 million people with chronic HBV worldwide (WHO 2022); 1.1 million deaths/year. Highest prevalence in Africa, Asia, Western Pacific (>8%). In high-prevalence regions, perinatal transmission accounts for 90% of cases.
Structure: Member of Hepadnaviridae (DNA viruses). Has:
- Outer lipid envelope with surface proteins (HBsAg)
- Inner nucleocapsid (HBcAg)
- Partially double-stranded circular DNA genome
Key antigens:
- HBsAg - surface antigen; three related glycoproteins (large, middle, small). Large HBsAg is on complete virions; small HBsAg released in huge quantities from infected hepatocytes as noninfectious particles
- HBcAg - nucleocapsid protein
- HBeAg - secreted form; correlates with active viral replication and high infectivity
- HBV DNA polymerase - has reverse transcriptase activity (replicates via RNA intermediate)
Pathogenesis: HBV itself is not directly cytopathic. Liver injury is mediated by the host CD8+ T cell response against infected hepatocytes. Immune tolerance (especially in perinatally infected patients) leads to the carrier state.
Clinical outcomes (5 possibilities):
- Acute hepatitis → recovery and viral clearance
- Fulminant hepatitis with massive liver necrosis
- Chronic hepatitis - nonprogressive
- Chronic hepatitis - progressive → cirrhosis
- Asymptomatic "healthy" carrier state
Morphology (Acute HBV): "Ground-glass" hepatocytes - pale, finely granular eosinophilic cytoplasm due to massive accumulation of HBsAg in the ER. These are pathognomonic of HBV.
Hepatitis C (HCV)
- Positive-strand RNA flavivirus
- Almost always subclinical acutely
- ~85% develop chronic hepatitis (most common cause of chronic viral hepatitis in the West)
- 20% of chronic cases progress to cirrhosis
- High mutation rate due to error-prone RNA polymerase → 6 major genotypes → makes vaccine development difficult
- Extrahepatic manifestations: mixed cryoglobulinemia, membranoproliferative glomerulonephritis
Characteristic histology: Portal tract expansion by lymphoid aggregates/follicles + fatty change (steatosis) in hepatocytes - relatively specific for HCV (see histology image below)
Hepatitis D (HDV) - Delta Agent
- Defective RNA virus - can only infect and replicate when HBV is also present (requires HBsAg for its own envelope)
- Two patterns:
- Coinfection (simultaneous HBV + HDV): generally self-limited, rarely chronic
- Superinfection (HDV in chronic HBV carrier): severe acute hepatitis, high risk of chronic disease and cirrhosis
Hepatitis E (HEV)
- Nonenveloped positive-strand RNA virus (genus Hepevirus)
- Fecal-oral transmission; endemic in equatorial and developing regions
- Usually self-limited acute hepatitis
- High mortality in pregnancy (up to 20%)
- Can cause chronic hepatitis in immunocompromised individuals
Morphological Patterns of Hepatitis
Acute Viral Hepatitis
Gross: Enlarged, congested liver with tense capsule.
Microscopic features:
- Hepatocyte injury: Ballooning degeneration (swollen, pale, rarefied cytoplasm) and eosinophilic degeneration
- Councilman (acidophil) bodies: Shrunken, deeply eosinophilic hepatocytes representing apoptotic cells - hallmark finding
- Lobular disarray: Loss of the normal hepatic plate architecture
- Inflammatory infiltrate: Predominantly lymphocytes and macrophages throughout the lobule and portal tracts
- Kupffer cell hypertrophy with phagocytosed debris (lipofuscin, bile)
- Cholestasis: Bile plugs in canaliculi in more severe cases
- Hepatocyte regeneration: Mitotic figures, binucleate cells
Severe/Fulminant acute hepatitis:
- Massive hepatocyte necrosis - bridging necrosis or panacinar necrosis
- Collapse of the reticulin framework
- Liver shrinks dramatically (acute yellow atrophy)
Chronic Viral Hepatitis
Defined as hepatic inflammation lasting >6 months with evidence of ongoing injury. Liver biopsy is the gold standard for assessment of:
- Activity/grade - degree of necroinflammation (portal, periportal/interface, lobular)
- Fibrosis/stage - extent of fibrosis (periportal → bridging → cirrhosis)
Key microscopic features of chronic hepatitis:
- Portal tract inflammation - lymphocytic infiltration expanding portal tracts
- Interface hepatitis (piecemeal necrosis) - lymphocytes breach the limiting plate between portal tract and parenchyma; hepatocytes undergo apoptosis at this junction - key indicator of activity
- Lobular hepatitis - scattered necroinflammatory foci within lobules
- Bridging necrosis - necrosis connecting portal tracts to central veins, or portal-to-portal; indicates severe activity
- Progressive fibrosis - periportal → portal-to-portal bridges → cirrhosis (Metavir staging: F0-F4)
HCV-specific features:
- Lymphoid follicles within portal tracts (very characteristic)
- Steatosis (fatty change)
- Bile duct damage
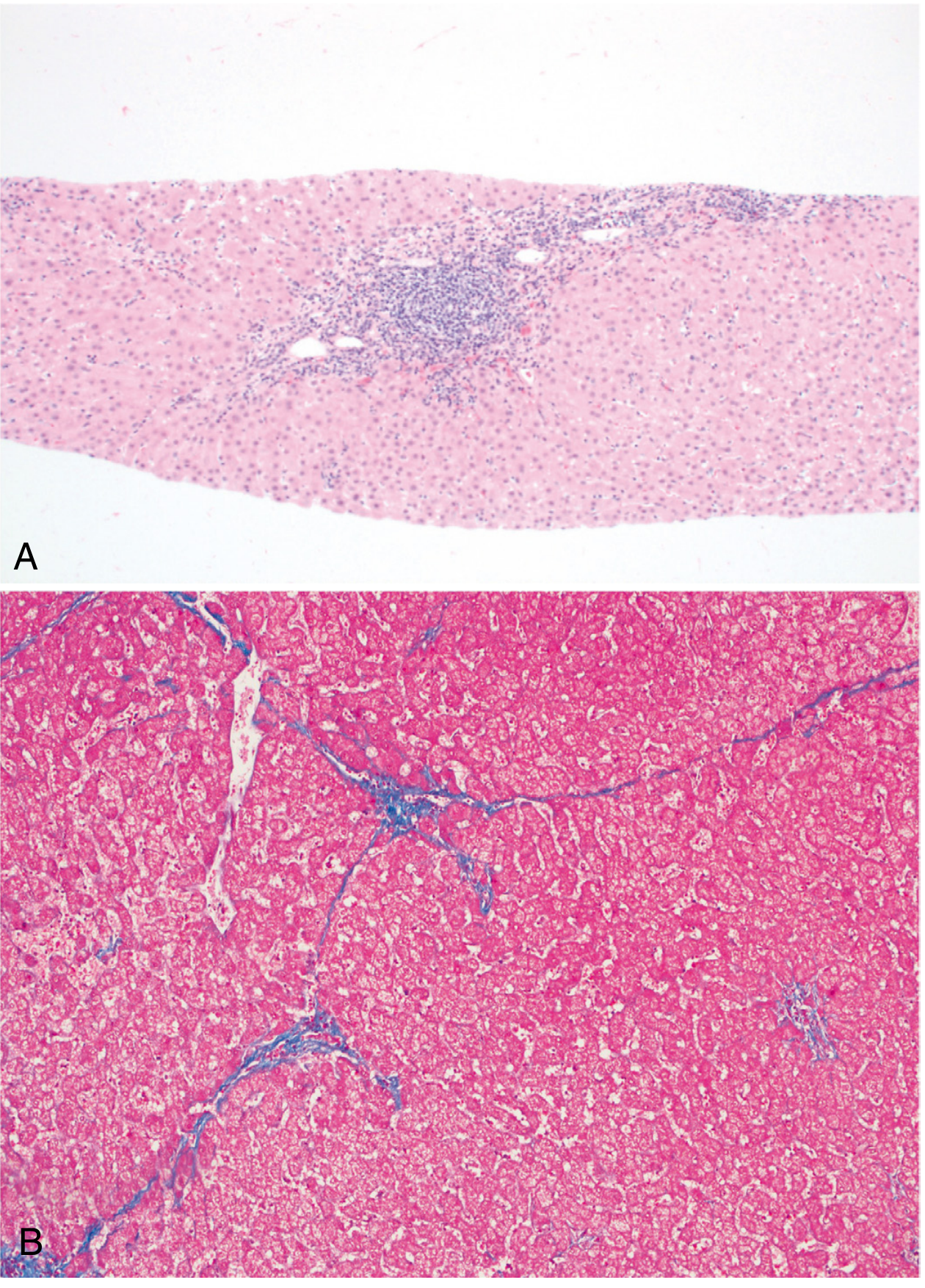
Fig: Chronic viral hepatitis due to HCV. (A) Portal tract expansion by a lymphoid aggregate, H&E. (B) Bridging fibrosis, trichrome stain showing collagen fibers in blue. - Robbins, Cotran & Kumar Pathologic Basis of Disease
Autoimmune Hepatitis
- Chronic, progressive hepatitis with female predominance (78%)
- Associated with other autoimmune diseases
- Responds to immunosuppression (90% remission rate)
Two types by autoantibody pattern:
| Type 1 | Type 2 | |
|---|---|---|
| Population | Adults | Children/teenagers |
| Antibodies | ANA, anti-SMA, anti-SLA/LP | Anti-LKM-1, anti-LC1, anti-SLA/LP |
Morphology:
- Interface hepatitis with confluent/bridging necrosis
- Plasma cell predominance in the mononuclear infiltrate (distinguishes from viral hepatitis)
- Hepatocyte "rosettes" - circular arrangement of regenerating hepatocytes around a dilated canaliculus
- Up to 30% have cirrhosis at presentation
Complications and Outcomes
| Complication | Associated Virus(es) |
|---|---|
| Cirrhosis | HBV, HCV, HDV |
| Hepatocellular carcinoma (HCC) | HBV >> HCV |
| Fulminant hepatic failure | HAV (rare), HBV, HDV superinfection, HEV in pregnancy |
| Cryoglobulinemia | HCV |
| MPGN | HCV, HBV |
| Polyarteritis nodosa | HBV |
HBV and HCC: HBV can integrate into the host genome and directly cause HCC even without cirrhosis (unlike HCV, which causes HCC almost exclusively through cirrhosis). HBV-encoded HBx protein has transcriptional transactivation properties that may promote carcinogenesis.
Key Grading/Staging Systems (Liver Biopsy)
| Stage (Fibrosis) | Metavir | Ishak |
|---|---|---|
| No fibrosis | F0 | 0 |
| Portal fibrosis without septa | F1 | 1-2 |
| Portal fibrosis with few septa | F2 | 3 |
| Numerous septa without cirrhosis | F3 | 4 |
| Cirrhosis | F4 | 5-6 |
Biopsy staging determines whether antiviral therapy is indicated and predicts prognosis.
Sources: Robbins & Kumar Basic Pathology (9780323790185), p. 600-607; Robbins, Cotran & Kumar Pathologic Basis of Disease (9780443264528), p. 772-779
This is a shared conversation. Sign in to Orris to start your own chat.