Grand mother effect Everything about this from standard obs text
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Searching the Web
grandmother hypothesis menopause evolution obstetrics gynecology textbook explanation
Reading File
Searching PubMed
"grandmother hypothesis" menopause evolution postreproductive
Loading Image
Grand mother effect with respect to obstetrics rh pregnancies
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Searching the Web
grandmother effect Rh isoimmunization obstetrics mechanism RhD sensitization at birth anti-D
Reading File
Finding Sources
Loading Image
Reading Web Page
https://www.sciencedirect.com/topics/medicine-and-dentistry/…
Now I have all the information needed to give a thorough, well-illustrated answer. Let me compile it.
The Grandmother Effect in Rh Isoimmunization
This is a completely different concept from the evolutionary "grandmother hypothesis." In obstetrics, the grandmother effect (also called the "grandmother theory") is a specific immunological mechanism that explains how an Rh-negative woman can become sensitized to the D antigen before she ever has her first pregnancy.
The Core Concept
The standard explanation for Rh sensitization requires fetal Rh-positive blood entering the maternal circulation - but clinicians occasionally encountered Rh-negative women with anti-D antibodies who had no identifiable prior exposure: no previous Rh-positive pregnancy, no blood transfusion, no sensitizing event.
The grandmother theory explains this paradox.
The Mechanism - Step by Step
Generation 1 - The Grandmother (Patient's Mother):
- The patient's mother (the grandmother) is Rh-positive
- She carries an Rh-negative fetus (the future patient)
- At the time of delivery, a maternal-fetal hemorrhage occurs (this is physiological - blood normally crosses from mother to fetus at delivery)
- Rh-positive red cells from the grandmother enter the fetal circulation of her Rh-negative baby
Generation 2 - The Patient (Future Mother):
- The Rh-negative baby (future patient) is thus exposed to Rh-positive (D antigen-bearing) red cells at her own birth
- These cells stimulate low-level anti-D antibody formation in the neonate
- The antibody levels are subclinical - they may not be detectable on routine antenatal screening
- However, immunological memory cells (sensitized B lymphocytes) are established
When the Patient Becomes Pregnant:
- Her first pregnancy with an Rh-positive fetus triggers an anamnestic (secondary) immune response
- Because she is already sensitized, the response is rapid and produces high-titer IgG anti-D
- This IgG crosses the placenta and causes Hemolytic Disease of the Fetus and Newborn (HDFN)
- Clinically, it behaves like a "second pregnancy" reaction, occurring in what appears to be her first pregnancy
Why This Matters Clinically
| Feature | Standard Rh Sensitization | Grandmother Effect |
|---|---|---|
| Sensitizing event | Previous Rh+ pregnancy or transfusion | Rh+ maternal blood at patient's own birth |
| When it occurs | After 1st pregnancy | Before patient's own 1st pregnancy |
| Detectable on routine screening | Usually yes (known exposure history) | May be undetectable / low titer |
| Clinical behavior | HDFN in 2nd+ pregnancy | HDFN in apparently 1st pregnancy |
| Prevention with RhIG | Standard prophylaxis effective | Cannot be prevented retroactively |
Pathogenesis of HDFN (Standard Path - for Context)
The standard sequence, from Robbins & Cotran Pathologic Basis of Disease:
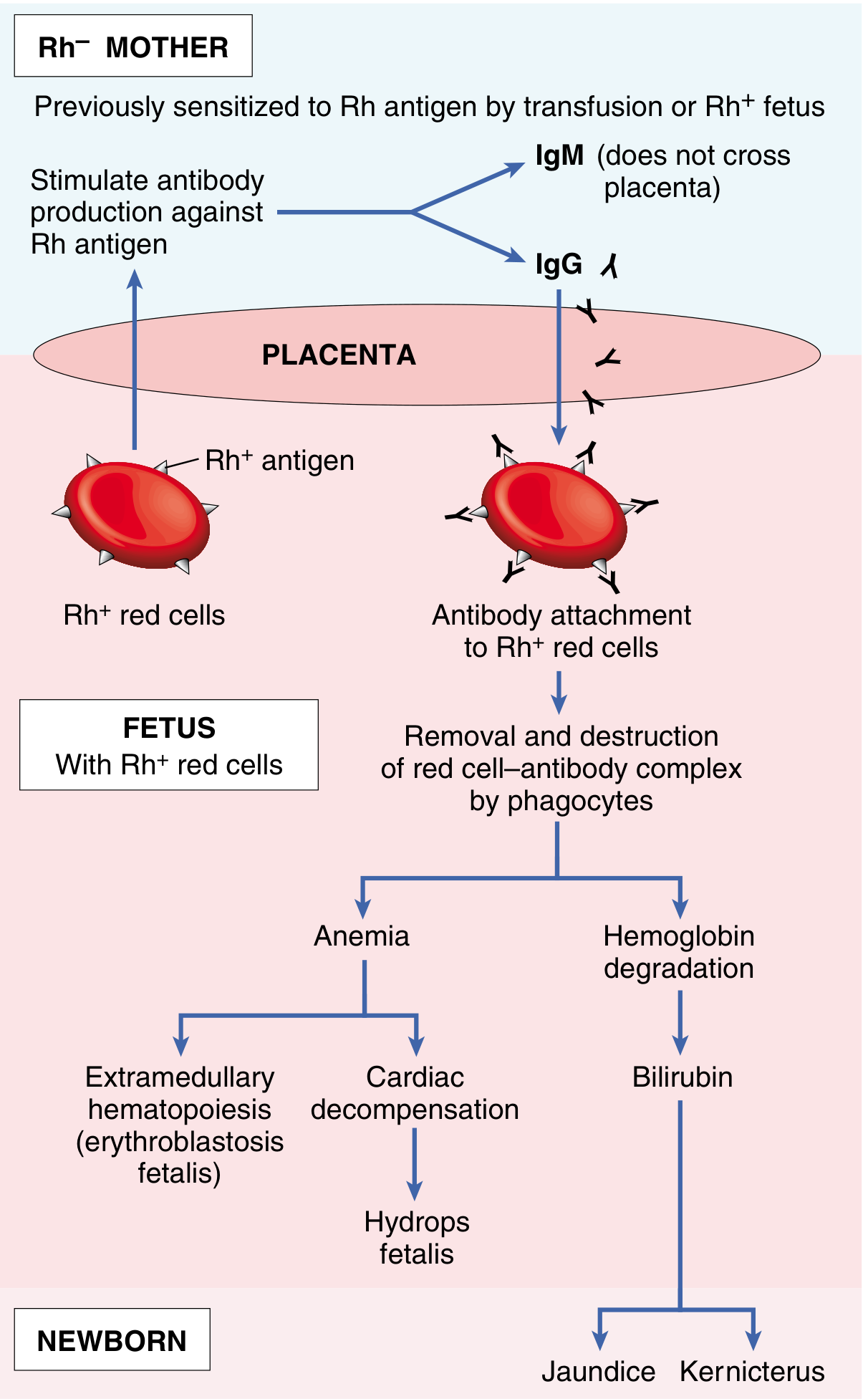
Key points from the diagram:
- IgM anti-D forms first - does not cross the placenta (large molecule)
- IgG anti-D forms subsequently - crosses the placenta via FcRn receptors
- IgG coats fetal Rh+ red cells → phagocytic destruction in fetal spleen/liver → fetal anemia
- Anemia → extramedullary hematopoiesis (erythroblastosis fetalis) + cardiac decompensation → hydrops fetalis
- Hemoglobin breakdown → bilirubin → jaundice and kernicterus postnatally
In the grandmother effect, all of this occurs in what the clinician records as the first pregnancy, because the sensitizing event happened a generation earlier.
Important Immunological Detail
- The sensitizing dose at the grandmother's delivery can be as little as 0.1-0.5 mL of Rh-positive fetal blood entering the baby's circulation
- The primary immune response after this neonatal exposure is slow (may take months to fully develop) and produces mainly IgM initially
- Antibody titers may be very low for years - hence why routine first-trimester Rh typing and antibody screening is essential; a low-level anti-D on booking bloods should never be ignored even in a primigravida
Clinical Implication - Why RhIG Cannot Help Here
Since the sensitization occurs at the patient's own birth (decades before her first pregnancy), there is no opportunity to administer RhIG prophylaxis to prevent the grandmother effect. This is why:
- All Rh-negative women should have indirect Coombs test (antibody screen) at booking regardless of parity
- A primigravida with anti-D should raise suspicion of either the grandmother effect, an unrecognized early miscarriage, or (rarely) prior transfusion
- Once sensitized, RhIG is of no benefit - management shifts to monitoring and intrauterine transfusion if needed
Sources: Robbins, Cotran & Kumar - Pathologic Basis of Disease, p. 436 | Henry's Clinical Diagnosis and Management by Laboratory Methods | Rhesus Isoimmunization overview (ScienceDirect)
This is a shared conversation. Sign in to Orris to start your own chat.