Cxt pneumothorax
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive textbook content and actual CXR images. Let me compose the full answer.
Pneumothorax on Chest X-Ray (CXR)
Definition
Air in the pleural space is a pneumothorax. When air and liquid are both present, a prefix is added: hydro-, haemo-, pyo-, or chylo- depending on the fluid type. - Grainger & Allison's Diagnostic Radiology, p. 67
Classic CXR Signs (Erect PA Film)
On an erect radiograph, pleural air rises to the lung apex. The hallmark findings are:
- Visceral pleural line - a thin, sharp white line running parallel to the chest wall, representing the edge of the collapsed lung
- Hyperlucent zone - avascular, dark region between the pleural line and the chest wall, with a complete absence of lung markings (vessels)
- Partial lung collapse - ipsilateral lung appears denser/smaller than normal
The right-sided pneumothorax below demonstrates these features clearly - note the absence of lung markings and increased (air density) lucency lateral to the pleural line:

FIGURE: Right-sided pneumothorax showing absence of lung markings and increased lucency lateral to the pleural line. - Tintinalli's Emergency Medicine, p. 1775
Expiratory CXR
Taking the film at deep expiration accentuates a pneumothorax because the lung volume decreases while the air in the pleural space remains constant, making the gap relatively larger. This is especially useful for small/subtle pneumothoraces.
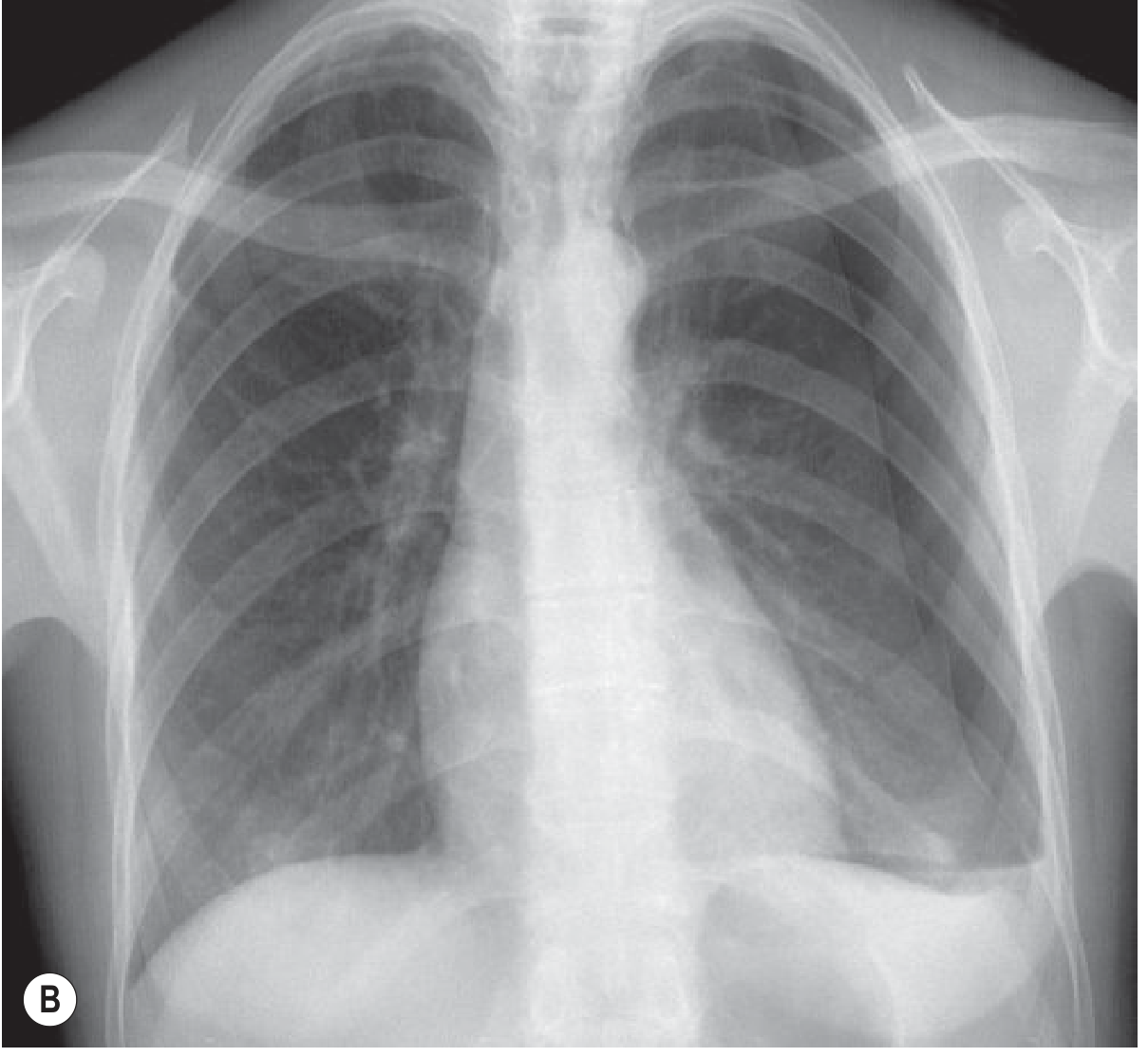
Fig. 3.17B: Left PSP, deep expiration - pneumothorax is accentuated. - Grainger & Allison's Diagnostic Radiology, p. 67
Tension Pneumothorax on CXR
Tension pneumothorax is a clinical diagnosis - do NOT delay treatment to get a CXR. If a film is taken, features include:
| Feature | Description |
|---|---|
| Contralateral mediastinal shift | Trachea/heart pushed away from affected side |
| Ipsilateral diaphragm depression | Pushed inferiorly - the more reliable sign |
| Expanded ipsilateral hemithorax | With complete collapse of the lung |
"Mild degrees of contralateral mediastinal shift are not unusual with a nontension pneumothorax because of the negative pressure in the normal pleural space. However, moderate or gross mediastinal shift should be taken as indicating tension, particularly if the ipsilateral hemidiaphragm is depressed." - Grainger & Allison's Diagnostic Radiology, p. 69
The image below shows a large left-sided pneumothorax with contralateral mediastinal shift (tension pattern):
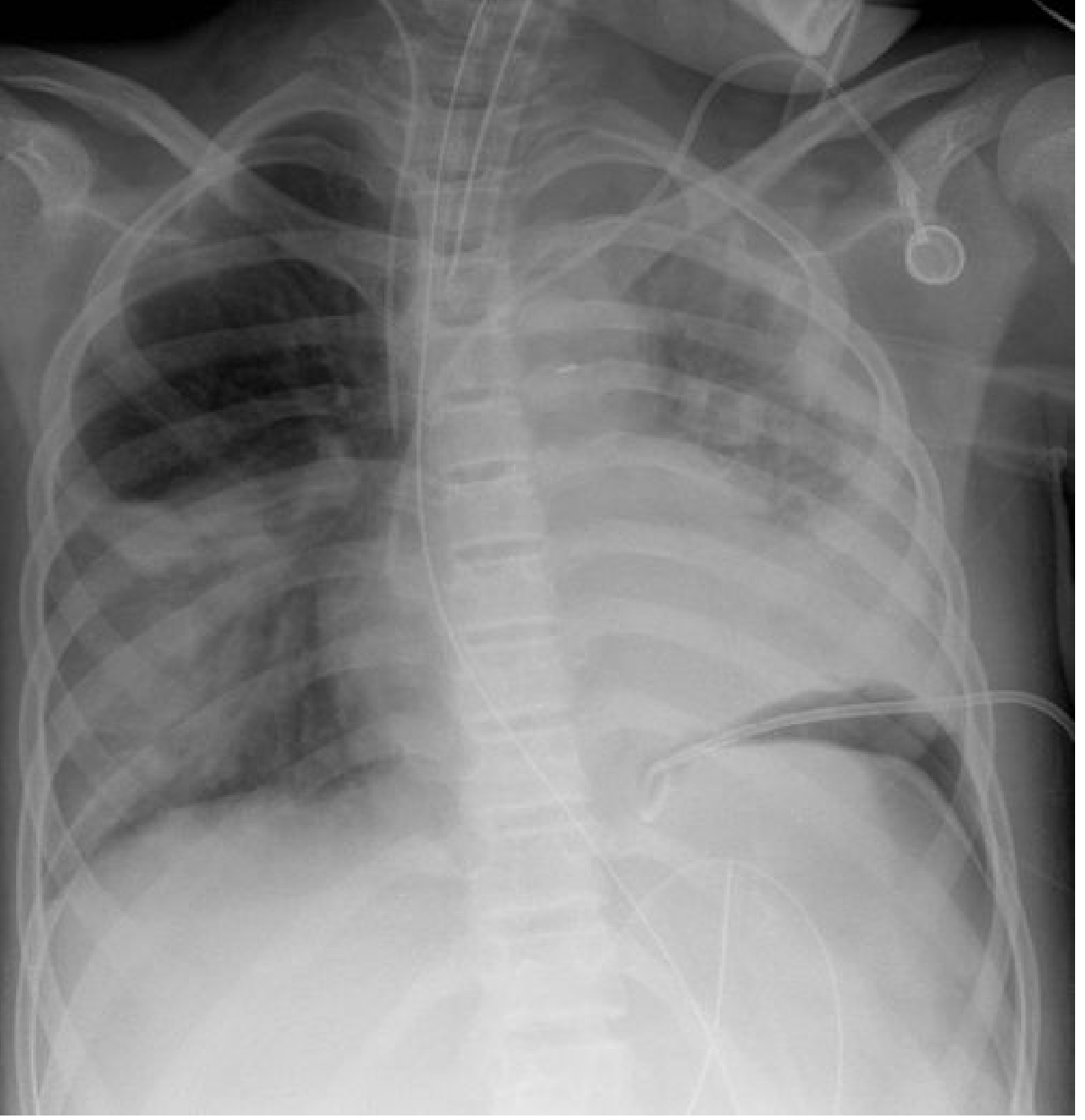
Fig. 3.19: Supine pneumothorax - large left-sided air collection with mediastinal shift. - Grainger & Allison's Diagnostic Radiology
Supine / Atypical CXR Signs
When the patient is supine (e.g. ICU/trauma), air rises anteriorly and basally, not to the apex. The classic apical pleural line may be absent. Look for:
| Sign | Appearance |
|---|---|
| Deep sulcus sign | Ipsilateral costophrenic angle appears abnormally deep and lucent |
| Generalised ipsilateral hyperlucency | Affected hemithorax appears darker overall |
| Double diaphragm sign | Anterior costophrenic recess seen as an oblique line, parallel to but distinct from the real diaphragm |
| Transradiant band | Parallel to diaphragm and/or mediastinum; undue clarity of mediastinal border |
| Visible cardiac fat pads | Appear as rounded opacities suggesting masses |
- Grainger & Allison's Diagnostic Radiology, p. 68
Pitfalls and Mimics
Skin folds are the most common mimic - especially in neonates and elderly patients positioned slumped in AP projection. Features that help distinguish skin fold from real pneumothorax:
- Skin fold line extends beyond the chest wall margin
- Laterally located blood vessels are still visible beyond the line
- The fold line is much wider than the thin visceral pleural line
- Orientation is inconsistent with the edge of a partially collapsed lung
Other mimics: bullae, pneumatoceles, pneumomediastinum, local emphysema. When doubt remains, CT is definitive.
Sizing the Pneumothorax
| Method | Small | Large |
|---|---|---|
| BTS (British Thoracic Society) | Visible rim <2 cm at apex | Rim ≥2 cm at apex |
| ACCP (Light's criteria) | <15% hemithorax volume | >15% hemithorax volume |
Clinically, size alone does not drive management - symptoms and haemodynamic status are equally important.
Diagnostic Sensitivity
| Modality | Sensitivity |
|---|---|
| Erect PA CXR | ~83% |
| Supine AP CXR | ~20-50% (misses 17-80%) |
| POCUS | Higher than supine CXR; rapid bedside diagnosis |
| CT | Most sensitive; gold standard for small/occult pneumothoraces |
"CXR will miss between 17% and 80% of pneumothoraces for upright and supine chest radiographs, respectively. POCUS is more sensitive than a supine radiograph." - Tintinalli's Emergency Medicine, p. 1775
Causes Summary
| Category | Examples |
|---|---|
| Primary spontaneous (PSP) | Ruptured apical bleb; young tall males, 20-40 yrs, M:F = 5:1 |
| Secondary spontaneous (SSP) | COPD, asthma, cystic fibrosis, TB, cavitating pneumonia, Marfan syndrome, LAM, histiocytosis X |
| Traumatic (non-iatrogenic) | Rib fracture, penetrating trauma, ruptured oesophagus/trachea |
| Iatrogenic | Central line insertion, thoracocentesis, percutaneous biopsy, tracheostomy |
| Catamenial | Endometriosis - occurs within 72 hours of menstruation |
- Grainger & Allison's Diagnostic Radiology, Table 3.2, p. 68
POCUS Findings (Ultrasound)
For completeness - when CXR is unavailable or inconclusive:
-
Absent pleural sliding (replaced by "barcode/stratosphere sign" on M-mode) - suggests pneumothorax
-
Lung point (transition between sliding and no-sliding) - highly specific for pneumothorax; represents the edge of the air collection
-
B-lines absent - their presence excludes pneumothorax at that location
-
Sea-shore sign absent on M-mode
-
Murray & Nadel's Textbook of Respiratory Medicine
Cxr findings in pneumothorax
I already covered this in detail in my previous response! Here's a focused summary of all CXR findings in pneumothorax:
CXR Findings in Pneumothorax
Erect PA Film (Classic/Standard)
| Finding | Description |
|---|---|
| Visceral pleural line | Thin, sharp white line parallel to the chest wall - the collapsed lung edge |
| Hyperlucent zone | Dark, avascular area between the pleural line and chest wall - no lung markings visible |
| Absent lung markings | No vascular shadows peripheral to the pleural line |
| Partial lung collapse | Ipsilateral lung appears smaller and relatively denser |
Expiratory Film
- Pneumothorax is accentuated on a deep expiratory film
- Lung shrinks on expiration but pleural air stays constant - increases the relative gap
- Useful for small/subtle pneumothoraces not seen on inspiration film
Tension Pneumothorax (on CXR)
Remember: tension PTx is a clinical diagnosis - never delay treatment for imaging.
| Finding | Detail |
|---|---|
| Ipsilateral diaphragm depression | Most reliable sign; almost invariably present |
| Contralateral mediastinal shift | Trachea and heart pushed to opposite side |
| Complete ipsilateral lung collapse | Dense opaque collapsed lung near hilum |
| Expanded hemithorax | Ribs spread apart on affected side |
Supine / AP Film (ICU, Trauma)
Air rises anteriorly and basally - not to the apex. The classic apical pleural line may be absent. Signs to look for:
| Sign | Appearance |
|---|---|
| Deep sulcus sign | Ipsilateral costophrenic angle abnormally deep and lucent - most recognisable sign |
| Generalised ipsilateral hyperlucency | Affected side appears darker overall |
| Double diaphragm sign | Anterior costophrenic recess creates a second line parallel to the diaphragm |
| Transradiant band | Along diaphragm or mediastinal border; mediastinal border appears unusually sharp |
| Visible cardiac fat pads | Appear as rounded opacities |
| Diaphragm depression | Present in larger collections |
Pitfalls / Mimics on CXR
| Mimic | How to differentiate |
|---|---|
| Skin fold | Line extends beyond chest wall; vessels visible beyond line; line much wider than pleural line; orientation inconsistent with collapsed lung edge |
| Bulla/bleb | No pleural line; concave inner margin; CT differentiates |
| Pneumomediastinum | Air tracks along mediastinal structures; continuous diaphragm sign |
| Gastric bubble | Subdiaphragmatic; air-fluid level |
When in doubt: CT is definitive (also detects occult pneumothoraces missed on CXR in 25-40% post-biopsy cases).
Sensitivity of CXR
| Position | Sensitivity |
|---|---|
| Erect PA | ~83% |
| Supine AP | Misses 17-80% of pneumothoraces |
POCUS outperforms supine CXR and is now the preferred bedside tool in trauma/ICU settings.
This is a shared conversation. Sign in to Orris to start your own chat.