Explain cataract and glaucome definition pathophysiology and management
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have more than enough comprehensive content from multiple authoritative sources. Let me compose the full detailed answer.
Cataract and Glaucoma: Definition, Pathophysiology, and Management
PART 1 - CATARACT
Definition
A cataract is an opacity of the crystalline lens of the eye. It may be congenital or acquired. The lens is a closed epithelial system enclosed entirely within the lens capsule; unlike other epithelia, it cannot shed dead cells, so they accumulate centrally with age, progressively losing transparency.
- Robbins & Kumar Basic Pathology: "Cataracts are opacities of the lens that may be congenital or acquired."
- Goldman-Cecil Medicine: "A cataract is an opacification of the crystalline lens."
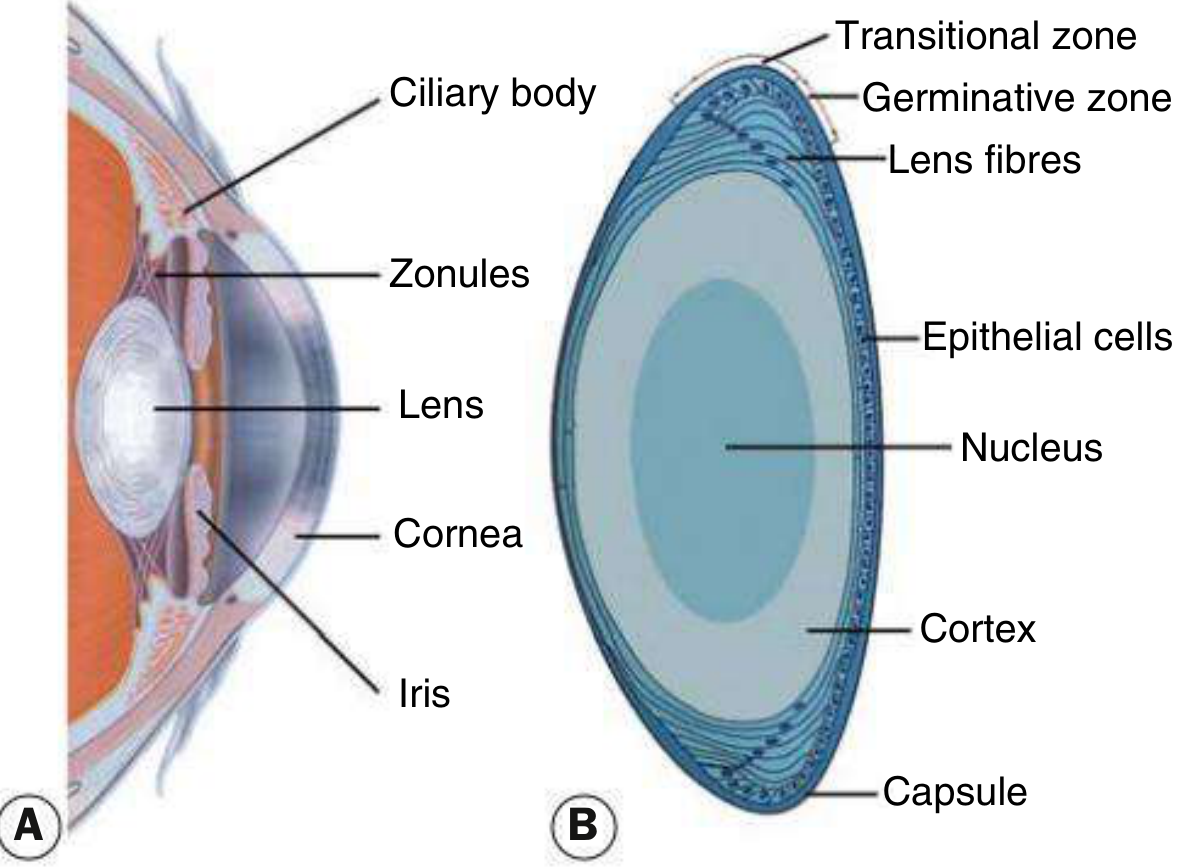
Lens Anatomy (relevant to pathophysiology)
The normal lens is made up of the capsule (basement membrane), a monolayer of epithelial cells, the cortex (newer lens fibres), and the nucleus (older compressed fibres). New fibres are continuously laid down from the germinative zone, pushing older fibres centrally. The lens is avascular and dependent on aqueous humor for nutrition.
Pathophysiology
Age-related cataract (most common)
The lens doubles in volume between birth and age 70. By age 45 it loses pliability (presbyopia). Continued accumulation of aged, denatured lens proteins in the nucleus leads to nuclear sclerosis - the most common form. Three main morphological subtypes exist:
| Subtype | Location | Key Feature |
|---|---|---|
| Nuclear sclerotic | Central nucleus | Yellowish/brown hue from urochrome pigment; associated myopia ("second sight of the aged") |
| Posterior subcapsular (PSC) | Just anterior to posterior capsule | Granular/plaque-like; most symptomatic - profoundly affects vision due to nodal point location; worsened by miosis |
| Cortical | Anterior/posterior cortex | Clefts and vacuoles from cortical hydration; cuneiform (wedge-shaped) or spoke-like opacities |
Kanski's Clinical Ophthalmology, 10th ed.
Biochemical mechanisms
- Oxidative damage to lens proteins leads to aggregation and light scattering
- In diabetes: hyperglycemia causes excess glucose in the aqueous → enters lens → converted to sorbitol by aldose reductase → sorbitol accumulates (cannot leave cell) → osmotic overhydration → cortical vacuoles → opacities. Classic diabetic cataract shows "snowflake" cortical opacities.
- In galactosemia: same pathway with galactitol
- Corticosteroids (systemic or topical): cause PSC cataracts
- Radiation: ionizing and infrared (e.g., glassblower's cataract) cause posterior opacities
Cataract maturity stages (Kanski)
- Immature - lens partially opaque
- Mature - lens completely opaque
- Hypermature - shrunken, wrinkled anterior capsule due to water leakage
- Morgagnian - cortex liquefied; nucleus sinks inferiorly
Secondary (complicated) cataracts
- Chronic anterior uveitis - most common cause; inflammation + steroids both contribute
- Acute angle-closure glaucoma - causes "glaukomflecken" (focal grey-white anterior capsular opacities = focal epithelial infarcts; pathognomonic)
- High myopia - PSC and early nuclear sclerosis
- Neurofibromatosis type 2 - PSC in >60% of patients
- Atopic dermatitis - bilateral anterior subcapsular shield-like plaques
- Silicone oil (intraocular) - almost universal cataract in phakic eyes
- Trauma - penetrating trauma ruptures capsule; blunt trauma gives "flower-shaped" opacity
Clinical Features
- Gradual, painless decrease in vision
- Glare (especially from headlights at night) - particularly with PSC and cortical cataracts
- Monocular diplopia
- Change in color perception (reduced blue perception)
- Difficulty in low-light situations
- Myopic shift ("second sight") - patient can suddenly read without glasses again as nuclear density increases the refractive index
Management
Indications for surgery
- Functional: opacity sufficient to interfere with daily activities (reading, driving, occupational needs)
- Medical: phacolytic glaucoma (hypermature lens protein leakage), phacomorphic glaucoma (intumescent lens causing angle closure), need for fundus visualization in diabetic retinopathy
Surgical techniques
Phacoemulsification (standard technique):
- Small-incision (2.2-2.8 mm) surgery under local anaesthesia as a day case
- Ultrasonic probe emulsifies and aspirates the lens nucleus and cortex
- Lens capsule is preserved intact
- A foldable intraocular lens (IOL) is implanted into the capsular bag
- Standard phacoemulsification gives results as good as femtosecond laser-assisted surgery (Goldman-Cecil)
Extracapsular cataract extraction (ECCE): larger incision; used for very hard nuclei
Intracapsular cataract extraction (ICCE): historical; entire lens including capsule removed
Preoperative precautions (Kanski)
- Alpha-blockers (e.g. tamsulosin for BPH) cause intraoperative floppy iris syndrome (IFIS) - must inform surgeon
- Anticoagulants: follow local protocol
- Diabetic patients: monitor retina before and after surgery (cataract surgery can worsen diabetic macular oedema)
Postoperative complications
- Posterior capsular opacification (PCO) - "after-cataract" - most common; treated with Nd:YAG laser capsulotomy
- Endophthalmitis, corneal decompensation, cystoid macular oedema
PART 2 - GLAUCOMA
Definition
Glaucoma is a collection of diseases characterized by progressive optic neuropathy, usually (but not always) associated with elevated intraocular pressure (IOP), resulting in damage to retinal ganglion cells and their axons, with characteristic optic nerve cupping and visual field loss.
- Goldman-Cecil: "Glaucoma is an optic neuropathy in which progressive damage to retinal ganglion cells and their axons results in the characteristic loss of optic nerve tissue and damage to the peripheral and central visual field."
- The primary site of damage is at the lamina cribrosa, where optic nerve axons exit the eye.
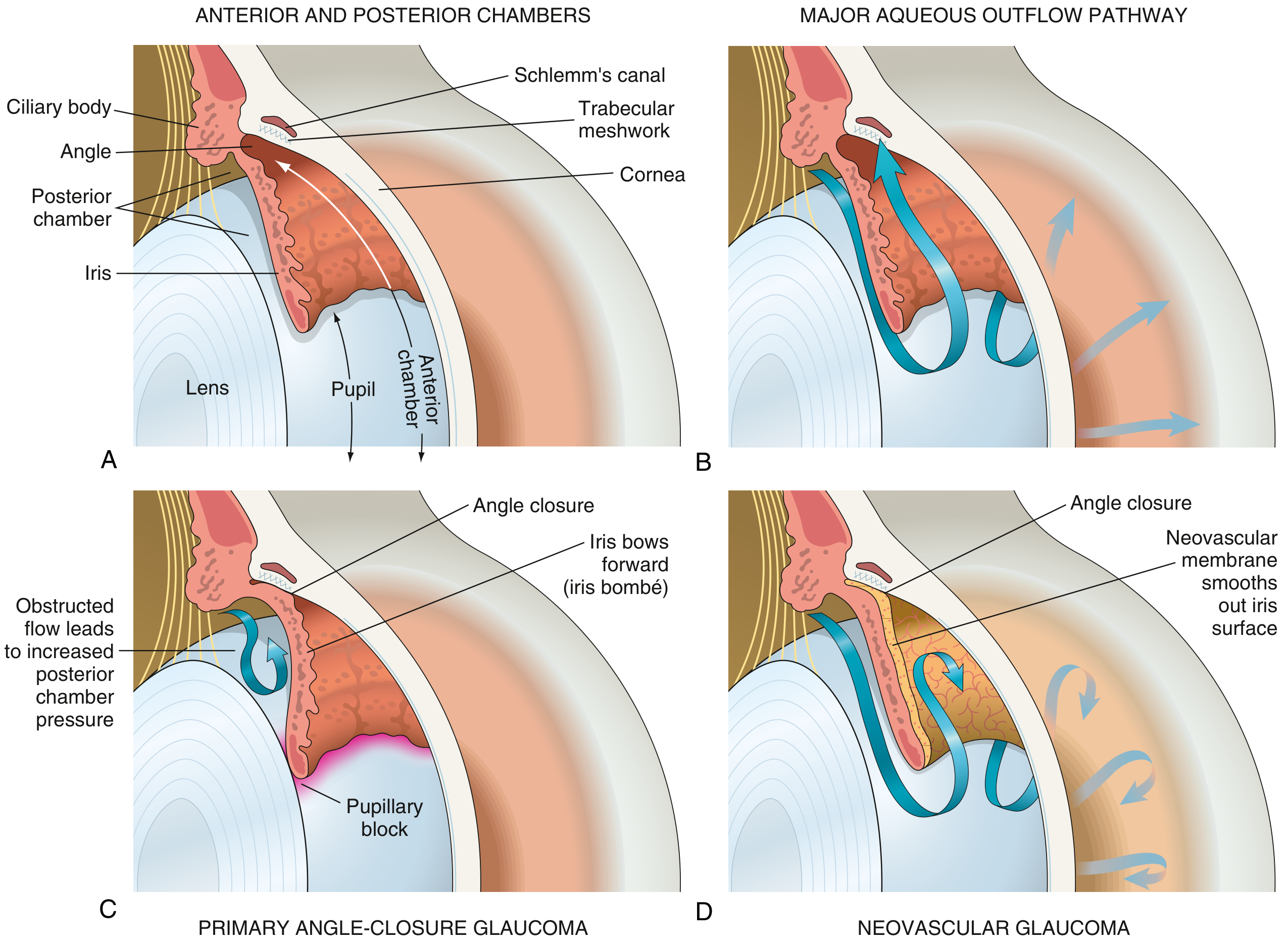
Aqueous Humor Physiology (basis of pathophysiology)
Aqueous humor is produced by the nonpigmented ciliary epithelium of the pars plicata of the ciliary body → flows into posterior chamber → passes through the pupil into the anterior chamber → drains mainly through the trabecular meshwork → into Schlemm's canal → episcleral veins. A minor pathway is the uveoscleral route.
If drainage does not match production, IOP rises. Normal IOP is 10-21 mmHg. >21 mmHg = ocular hypertension (but note: some develop glaucoma at normal IOP = "normal-tension glaucoma").
Classification and Pathophysiology
1. Primary Open-Angle Glaucoma (POAG) - most common
- Anterior chamber angle is anatomically open with free access to trabecular meshwork
- Mechanism: increased resistance to aqueous outflow at the level of trabecular meshwork (trabecular cell dropout, extracellular matrix accumulation) → IOP rises insidiously
- Chronic, bilateral, painless, asymptomatic until late stages
- Peripheral visual field loss first; central vision preserved until advanced disease
- Risk factors: age, African ancestry, family history, myopia, thin corneas, disc haemorrhages, low blood pressure
2. Primary Angle-Closure Glaucoma (PACG)
- Mechanism: pupillary block - anatomically shallow anterior chamber (common in hyperopes, small eyes) → lens enlarges with age → iris-lens apposition at pupil → aqueous builds in posterior chamber → pushes peripheral iris forward (iris bombé) → peripheral iris occludes trabecular meshwork → acute IOP spike (can reach >60 mmHg, nearly equaling diastolic arterial pressure)
Acute attack symptoms:
- Severe eye pain (may radiate to head)
- Nausea and vomiting (can mimic acute abdomen)
- Blurred vision with halos around lights
- Red eye with mid-dilated, non-reactive pupil (fixed due to ischemia of iris sphincter)
- Corneal haze/oedema
3. Secondary Open-Angle Glaucoma
- Pseudoexfoliation syndrome (PXF/PEX): most common secondary cause; fibrillogranular material (abnormal fibrillin) deposits on lens, iris, trabecular meshwork → mechanical obstruction; especially common in Scandinavians and Saudi Arabians
- Steroid-induced glaucoma: corticosteroids increase trabecular meshwork resistance
- Pigment dispersion syndrome: pigment granules from iris rub onto trabecular meshwork
- Traumatic/hemorrhagic: red blood cells or ghost cells block trabecular meshwork
4. Secondary Angle-Closure Glaucoma
- Neovascular glaucoma (NVG): new vessels (from retinal ischemia in DR, CRVO) grow over iris and trabecular meshwork as a fibrovascular membrane → contracts → peripheral anterior synechiae → angle closure
- Lens-induced: phacolytic (hypermature lens proteins) or phacomorphic (intumescent lens pushes iris forward)
5. Normal-Tension Glaucoma
- Optic neuropathy and visual field loss with IOP consistently ≤21 mmHg
- Vascular mechanisms (nocturnal hypotension, vasospasm) likely contribute to optic nerve ischemia
Optic Nerve Changes
Rising IOP compresses axons at the lamina cribrosa → ischemic axon loss. Clinically this manifests as:
- Enlarged cup-to-disc (C/D) ratio (normal <0.5; >0.7 suspicious; asymmetry >0.2 significant)
- Inferior and superior notching of the neuroretinal rim ("ISNT rule" - normal: Inferior > Superior > Nasal > Temporal rim thickness)
- Disc haemorrhages
- Peripapillary retinal nerve fibre layer (RNFL) thinning on OCT
Diagnosis
- Tonometry: IOP measurement (Goldmann applanation - gold standard)
- Gonioscopy: classification of angle (open vs closed)
- Optic disc assessment: slit lamp + 78D lens; OCT of RNFL
- Visual field testing: Humphrey automated perimetry
- 24-2 pattern: tests within 24° temporal, 30° nasal (routine glaucoma monitoring)
- 10-2 pattern: detailed central field assessment in advanced glaucoma
Management
Medical (pharmacological - for open-angle glaucoma)
All agents aim to reduce IOP as the primary modifiable risk factor. Drops are typically lifelong.
| Drug Class | Example | Mechanism |
|---|---|---|
| Prostaglandin analogues (1st line) | Latanoprost 0.005%, travoprost 0.004% - once daily | Increase uveoscleral outflow |
| Beta-blockers | Timolol 0.5% - twice daily | Reduce aqueous production |
| Carbonic anhydrase inhibitors (CAI) | Dorzolamide drops 3x/day; acetazolamide oral/IV | Reduce aqueous production |
| Alpha-2 agonists | Brimonidine drops 3x/day | Reduce production + increase uveoscleral outflow |
| Rho-kinase inhibitors | Netarsudil 0.02% - once daily | Increase conventional outflow through trabecular meshwork |
(Goldman-Cecil Medicine)
Laser treatment
- Laser trabeculoplasty (SLT/ALT): applies energy to trabecular meshwork → increases outflow. Now considered first-line in many guidelines; can maintain IOP control for years without medications.
- Laser peripheral iridotomy (LPI): treatment of choice for angle-closure glaucoma; creates a hole in the peripheral iris to bypass pupillary block and equalize pressure between posterior and anterior chambers. Also done prophylactically in the fellow eye.
Surgery
For refractory cases where medical and laser treatment fails:
- Trabeculectomy: creates a fistula between anterior chamber and sub-Tenon space (filtering bleb) - bypasses trabecular meshwork; often performed with mitomycin C to prevent bleb scarring
- Tube-shunt (glaucoma drainage device): synthetic tube from anterior chamber into reservoir behind eye equator; preferred when trabeculectomy likely to fail (e.g. neovascular glaucoma, previous failed trabeculectomy)
- Minimally invasive glaucoma surgery (MIGS): newer ab interno procedures (iStent, Hydrus) with better safety profiles
- Cyclodestructive procedures (diode laser cyclophotocoagulation): reduces ciliary body aqueous production; used when other options exhausted
Acute angle-closure glaucoma - emergency management
- Immediate IOP lowering:
- Topical timolol 0.5% (one dose)
- IV acetazolamide 250-500 mg (or oral if IV not available)
- Topical pilocarpine (to constrict pupil and pull iris away from angle)
- IV mannitol (osmotic agent) if above insufficient
- Once IOP lowered: Laser peripheral iridotomy (definitive treatment)
- Prophylactic LPI in the fellow eye
- Lens extraction may be considered (enlarging lens contributes to angle narrowing)
Risk Factors Summary
| Cataract | Glaucoma |
|---|---|
| Increasing age | Increasing age |
| Diabetes mellitus | African ancestry |
| Corticosteroids | Family history / genetics |
| UV radiation | Elevated IOP |
| Trauma | Thin cornea |
| Systemic disease (Wilson's, atopic, myotonic dystrophy) | Myopia (for POAG), Hyperopia (for PACG) |
| Smoking | Disc haemorrhages |
Key Differences
| Feature | Cataract | Glaucoma |
|---|---|---|
| Primary pathology | Lens opacity | Optic neuropathy |
| Pain | None | None (POAG); Severe (acute PACG) |
| IOP | Normal | Often elevated |
| Visual loss | Gradual, blurred | Peripheral field loss (POAG); Acute (PACG) |
| Reversibility | Fully reversible with surgery | Irreversible nerve damage |
| Treatment | Surgery (phacoemulsification + IOL) | Drops, laser, surgery |
Sources:
- Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed. (Elsevier)
- Goldman-Cecil Medicine, International Edition (Elsevier)
- Robbins & Kumar Basic Pathology (Elsevier)
- Robbins, Cotran & Kumar Pathologic Basis of Disease (Elsevier)
Papilloedema
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
I now have comprehensive data from five authoritative textbooks plus fundus images. Here is the full structured answer:
Papilloedema
Definition
Papilloedema is swelling of the optic nerve head specifically secondary to raised intracranial pressure (ICP). This precise term must be distinguished from the broader terms "disc swelling" or "disc oedema," which include papilloedema but also disc swelling from other causes (e.g., optic neuritis, ischaemia, infiltration).
"Papilloedema is swelling of the optic nerve head secondary to raised intracranial pressure. All patients with papilloedema should be suspected of harbouring an intracranial mass." - Kanski's Clinical Ophthalmology, 10th ed.
"Papilledema refers to bilateral swelling of the optic nerve head as a result of elevated intracranial pressure." - Robbins & Kumar Basic Pathology
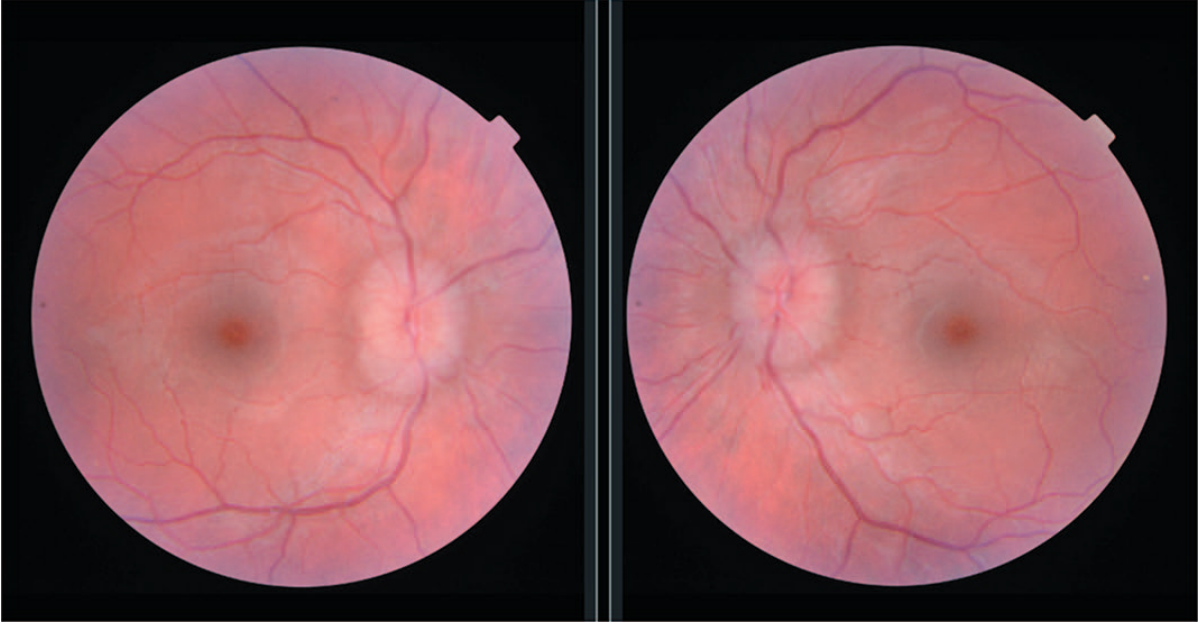
Papilloedema is nearly always bilateral, although it may be asymmetric. Unilateral disc swelling is more likely due to a local cause.
Pathophysiology
CSF Circulation (Normal)
To understand papilloedema, CSF dynamics must be understood:
- CSF is formed by the choroid plexus in the ventricles
- Flows: Lateral ventricles → Foramina of Monro → Third ventricle → Sylvian aqueduct → Fourth ventricle → Foramina of Luschka and Magendie → Subarachnoid space
- Absorbed via arachnoid villi into cerebral venous sinuses
- Normal CSF pressure (lumbar puncture, not upright): 10-18 cmH₂O in adults
Mechanism of Optic Nerve Head Swelling
The optic nerve is surrounded by a meningeal sheath that is continuous with the intracranial subarachnoid space, meaning raised ICP is directly transmitted down the optic nerve sheath to the retrolaminar nerve.
Two key mechanisms operate:
- Obstruction of axoplasmic flow: Raised pressure around the retrolaminar optic nerve compresses axons at the lamina cribrosa → blocks orthograde and retrograde axoplasmic transport → axoplasm accumulates in nerve fibres → swelling of the optic disc
- Venous stasis: Nerve fibre oedema compresses capillaries and venules → venous stasis and dilation → microaneurysm formation → flame-shaped haemorrhages at the disc and peripapillary area
(Bradley and Daroff's Neurology in Clinical Practice)
Importantly, in acute papilloedema, visual acuity and colour vision are typically preserved - there is a mismatch between significant disc swelling and relatively spared visual function. This helps distinguish papilloedema from anterior ischaemic optic neuropathy.
Causes of Raised ICP (Causes of Papilloedema)
| Category | Examples |
|---|---|
| Space-occupying lesions | Brain tumour, abscess, subdural/extradural haematoma, intracerebral haemorrhage |
| Obstruction of ventricular system | Hydrocephalus (congenital stenosis of aqueduct, posterior fossa tumour compressing 4th ventricle) |
| Impaired CSF absorption | Meningitis, subarachnoid haemorrhage, trauma |
| Cerebral venous sinus thrombosis | Particularly in pregnancy, hypercoagulable states |
| Cerebral oedema | Stroke, encephalitis, hypertensive crisis |
| Idiopathic intracranial hypertension (IIH) | Obese young women; pseudotumour cerebri |
| Infectious | Cryptococcal meningitis (most commonly associated with significant papilloedema) |
Cryptococcal meningitis is the infectious disorder most commonly causing significant papilloedema (Bradley & Daroff).
Causes of Optic Disc Elevation (must distinguish from papilloedema)
- Pseudopapilloedema (disc drusen, tilted disc, hypermetropic crowded disc)
- Anterior ischaemic optic neuropathy
- Optic neuritis (inflammatory/infiltrative)
- Accelerated hypertension
- Central retinal vein occlusion
- Uveitis, posterior scleritis, hypotony
Clinical Features
Symptoms
| Symptom | Notes |
|---|---|
| Headache | Present in >90% of IIH; typically worse in morning, with Valsalva |
| Transient visual obscurations | Lasting seconds in one or both eyes; precipitated by bending, coughing, Valsalva - pathognomonic of established papilloedema |
| Nausea and vomiting | Due to raised ICP |
| Horizontal diplopia | Due to unilateral or bilateral 6th nerve palsy (false localising sign - abducens nerve stretched over petrous tip as ICP rises) |
| Visual field loss | Enlarged blind spot earliest; peripheral constriction; arcuate defects (inferonasal) |
| Visual acuity | Preserved early; severe reduction is a late sign indicating secondary optic atrophy |
| Pulsatile tinnitus | Particularly in IIH |
Ophthalmoscopic signs (key)
- Absent spontaneous venous pulsations (SVP) - normally seen where veins enter the disc; their absence indicates ICP >20 cmH₂O (important early sign, though not present in ~20% of normal individuals)
- Disc hyperaemia and oedema
- Blurring of disc margins (superior and inferior poles first - where NFL is thickest)
- Engorged, tortuous retinal veins
- Peripapillary flame-shaped haemorrhages
- Cotton-wool spots (NFL infarcts)
- Paton's lines (circumferential retinal folds around disc)
Stages of Papilloedema
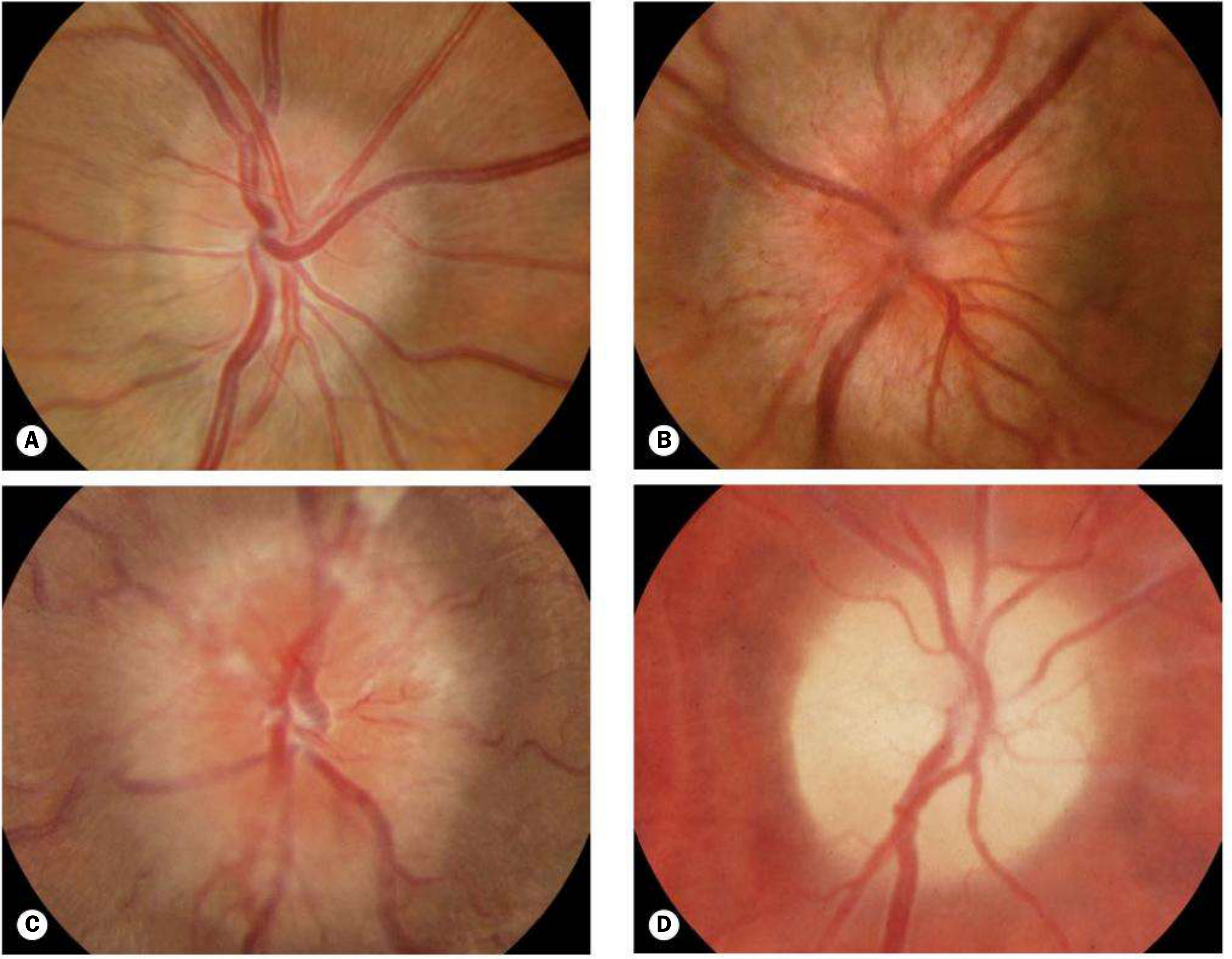
Stage 1 - Early
- Mild disc hyperaemia with capillary dilation; central cup preserved
- Mild opacification of peripapillary nerve fibre layer (loses linear light reflex)
- Mild swelling, most prominent at superior and inferior poles
- Absent SVP
- Peripapillary NFL haemorrhages
Stage 2 - Fully Developed (Acute)
- Gross disc surface elevation; central cup still initially retained (distinguishes from glaucoma)
- Engorged and tortuous retinal veins
- Splinter haemorrhages at/adjacent to disc margin
- Surface vessels obscured by opaque, swollen NFL
- Cotton-wool spots (NFL infarcts)
- Paton's lines (circumferential/concentric retinal folds) or choroidal folds
- Macular star or exudates
- In acute cases (e.g., subarachnoid haemorrhage): subhyaloid haemorrhages → may break into vitreous (Terson syndrome)
- Visual acuity still typically preserved
Stage 3 - Chronic
- Haemorrhages and cotton-wool spots resolve
- Central cup eventually becomes obliterated
- Disc changes from hyperaemic → milky grey appearance
- Visual fields begin to constrict
- Optociliary shunt (collateral) vessels appear (dilation of pre-existing retinociliary communications)
- Drusen-like crystalline deposits (corpora amylacea / pseudodrusen) on disc surface = extruded axoplasm from prolonged stasis; disc takes on "champagne cork" appearance
Stage 4 - Atrophic (Secondary Optic Atrophy)
- Papilloedema resolves but ICP damage has been sustained
- Optic disc pallor (grey-white) with slight elevation, few crossing vessels, indistinct margins
- Visual acuity severely impaired
- Visual fields severely constricted
- Retinal vessels narrow and sheathed
- Central vision may be relatively spared until very late (selective loss of peripheral axons)

Investigations
1. Neuroimaging (MANDATORY FIRST STEP)
"All patients with papilloedema should undergo urgent neuroradiological investigation to exclude intracranial pathology." - Kanski
- MRI brain (preferred): excludes space-occupying lesions, enlarged ventricles, sinus thrombosis; can measure optic nerve sheath diameter (ONSD, normal ~5.5 mm on MRI)
- CT brain: faster; used acutely
- MR venography (MRV): to exclude cerebral venous sinus thrombosis
- MRI signs of IIH: slit-like ventricles, flattening of pituitary gland ("empty sella sign"), posterior globe flattening
2. Lumbar Puncture
- ONLY after imaging excludes space-occupying lesion (risk of transtentorial herniation if performed blindly)
- Also contraindicated with coagulopathy
- Opening pressure measured with patient in lateral decubitus position
- CSF analysis for infection (cryptococcal meningitis, bacterial meningitis), malignancy
3. B-Scan Ultrasonography
- ONSD measured 3 mm posterior to the globe (axially)
- ONSD ≥5.0-5.7 mm = raised ICP (sensitivity/specificity 80-90%)
- "Crescent sign": echolucent area in anterior intra-orbital nerve = increased nerve-sheath separation
- 30-degree test: lateral gaze causes ~10% reduction in ONSD diameter on A-scan if fluid is present (positive in papilloedema, not in infiltration)
- Advantage: ONSD does not normalise with short-term ICP fluctuations (unlike SVP)
4. Fluorescein Angiography
- Arterial phase: absent/delayed disc fluorescence
- AV phase: dilated capillaries and microaneurysms
- Venous phase: fluorescein leakage beyond disc margins (distinguishes true papilloedema from pseudopapilloedema where leakage is absent)
5. Visual Function Monitoring
- Visual acuity, colour vision, automated perimetry (visual fields)
- OCT of RNFL thickness
Distinguishing Papilloedema from Pseudopapilloedema
| Feature | True Papilloedema | Pseudopapilloedema (e.g., drusen) |
|---|---|---|
| Central cup | Present early (obliterated late) | Absent |
| SVP | Absent | Present |
| Haemorrhages | Present | Absent (rare exceptions) |
| Cotton-wool spots/exudates | May be present | Absent |
| Fluorescein leakage | Present | Absent |
| Vessels | Obscured by oedema | Arise from central disc apex |
| Vessel anomalies | None | Anomalous branching, increased number |
| Transillumination | No glow | Drusen may glow |
Management
Management is directed at treating the underlying cause of raised ICP and protecting visual function.
Treat the Cause
- Brain tumour → neurosurgical resection, radiotherapy
- Hydrocephalus → ventriculoperitoneal (VP) shunt
- Venous sinus thrombosis → anticoagulation
- Meningitis → appropriate antimicrobials
- Discontinue offending drugs (tetracyclines, vitamin A derivatives, OCP in IIH)
Idiopathic Intracranial Hypertension (IIH) - most common cause managed medically
1. Weight loss
- Most important intervention in obese patients
- Bariatric surgery effective in refractory cases
- Even modest weight gain (5-15%) in non-obese women is a risk factor
2. Medical therapy
- Acetazolamide (carbonic anhydrase inhibitor) - first-line drug - reduces CSF production; improves symptoms and reduces disc swelling
- Furosemide - second-line diuretic
- Corticosteroids - controversial; short course sometimes used in severe papilloedema
- IV mannitol - reserved for acute exacerbations (hyperosmotic agent)
- Topiramate - adjunct (also aids weight loss)
3. Lumbar puncture
- Therapeutic LP gives transient ICP reduction
- Useful for acute exacerbations
- Effect is usually short-lived; repeated LPs not practical long-term
4. Surgical options (for progressive visual loss unresponsive to medical treatment)
- Optic nerve sheath fenestration (ONSF): incisions in the optic nerve sheath to allow CSF to decompress and protect the optic nerve; primary indication is progressive visual loss
- Lumboperitoneal shunting: diverts CSF from lumbar space to peritoneum; high complication rate (shunt failure, radiculopathy)
- Transverse dural sinus stenting: treats venous sinus stenosis contributing to raised ICP; increasingly used but technically demanding
Ophthalmologist's Role
- Diagnosis and monitoring of visual function: VA, colour vision, visual fields, optic disc photography, OCT RNFL
- Communicate urgency of visual loss to neurologist/neurosurgeon for escalation of management
Key Clinical Pearls
- Papilloedema ≠ disc swelling - papilloedema strictly means raised ICP; other causes of disc swelling must be excluded
- 6th nerve palsy in papilloedema is a false localising sign - it does not indicate a lesion at the brainstem; it results from stretching of the long abducens nerve over the petrous tip
- Preserved central vision in acute papilloedema is a distinguishing feature - when acuity drops acutely, consider optic neuritis or ischaemic optic neuropathy
- LP is contraindicated without prior imaging - risk of downward transtentorial herniation
- Optociliary shunt vessels in chronic papilloedema develop as the retinal venous system bypasses obstruction through pre-existing retinociliary communications
- VP shunt failure should be suspected when visual loss or signs of dorsal midbrain syndrome appear, even without ventriculomegaly on imaging ("stiff ventricles" phenomenon)
Sources:
- Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed.
- Bradley and Daroff's Neurology in Clinical Practice
- Localization in Clinical Neurology, 8th ed.
- Adams and Victor's Principles of Neurology, 12th ed.
- Robbins & Kumar Basic Pathology
This is a shared conversation. Sign in to Orris to start your own chat.