Shoulder complex detailed notes
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Loading Image
I now have all the material needed to write detailed, well-illustrated notes. Here they are:
The Shoulder Complex - Detailed Notes
Sources: Gray's Anatomy for Students; General Anatomy and Musculoskeletal System (THIEME Atlas); Rockwood and Green's Fractures in Adults 10th ed 2025
1. Overview
The shoulder complex is not a single joint - it is a group of four articulations that work together to provide the widest range of motion of any joint in the body:
- Glenohumeral joint - the "true" shoulder joint (ball and socket)
- Acromioclavicular (AC) joint - clavicle to acromion
- Sternoclavicular (SC) joint - clavicle to sternum; the only true bony connection between the upper limb and the trunk
- Scapulothoracic articulation - a physiological (not synovial) joint between the scapula and the thoracic cage
This design prioritizes mobility over stability - compensated by the rotator cuff, glenoid labrum, and ligaments.
2. Bones of the Shoulder Complex
Clavicle
- S-shaped bone; medial two-thirds are convex anteriorly, lateral third is concave anteriorly
- Acts as a strut, transmitting forces from the upper limb to the axial skeleton
- Most commonly fractured bone at its middle third
- Articulates medially with the manubrium (SC joint) and laterally with the acromion (AC joint)
Scapula
- Flat, triangular bone lying on the posterior thorax (ribs 2-7)
- Key landmarks:
- Spine - horizontal ridge separating the supraspinous and infraspinous fossae
- Acromion - lateral projection of the spine; forms the AC joint
- Coracoid process - hook-shaped projection anteriorly; attachment for muscles and ligaments
- Glenoid cavity - shallow, pear-shaped fossa; articulates with the humeral head
- Supraglenoid tubercle - attachment for long head of biceps
- Infraglenoid tubercle - attachment for long head of triceps
- Suprascapular notch - converted into a foramen by the superior transverse scapular ligament
Humerus
- Anatomical neck - between the head and tubercles; joint capsule attaches here
- Surgical neck - between the tubercles and shaft; site of fractures; axillary nerve closely related
- Greater tubercle - posterolateral; receives supraspinatus (superior facet), infraspinatus (middle facet), teres minor (inferior facet)
- Lesser tubercle - anterior; receives subscapularis
- Intertubercular sulcus (bicipital groove) - between the tubercles; houses the tendon of the long head of biceps brachii, held by the transverse humeral ligament
- Deltoid tuberosity - on the lateral shaft; insertion of deltoid muscle
3. Glenohumeral Joint
The glenohumeral joint is the primary joint of the shoulder. It is a synovial ball-and-socket joint between the large spherical head of the humerus and the small, shallow glenoid cavity of the scapula.
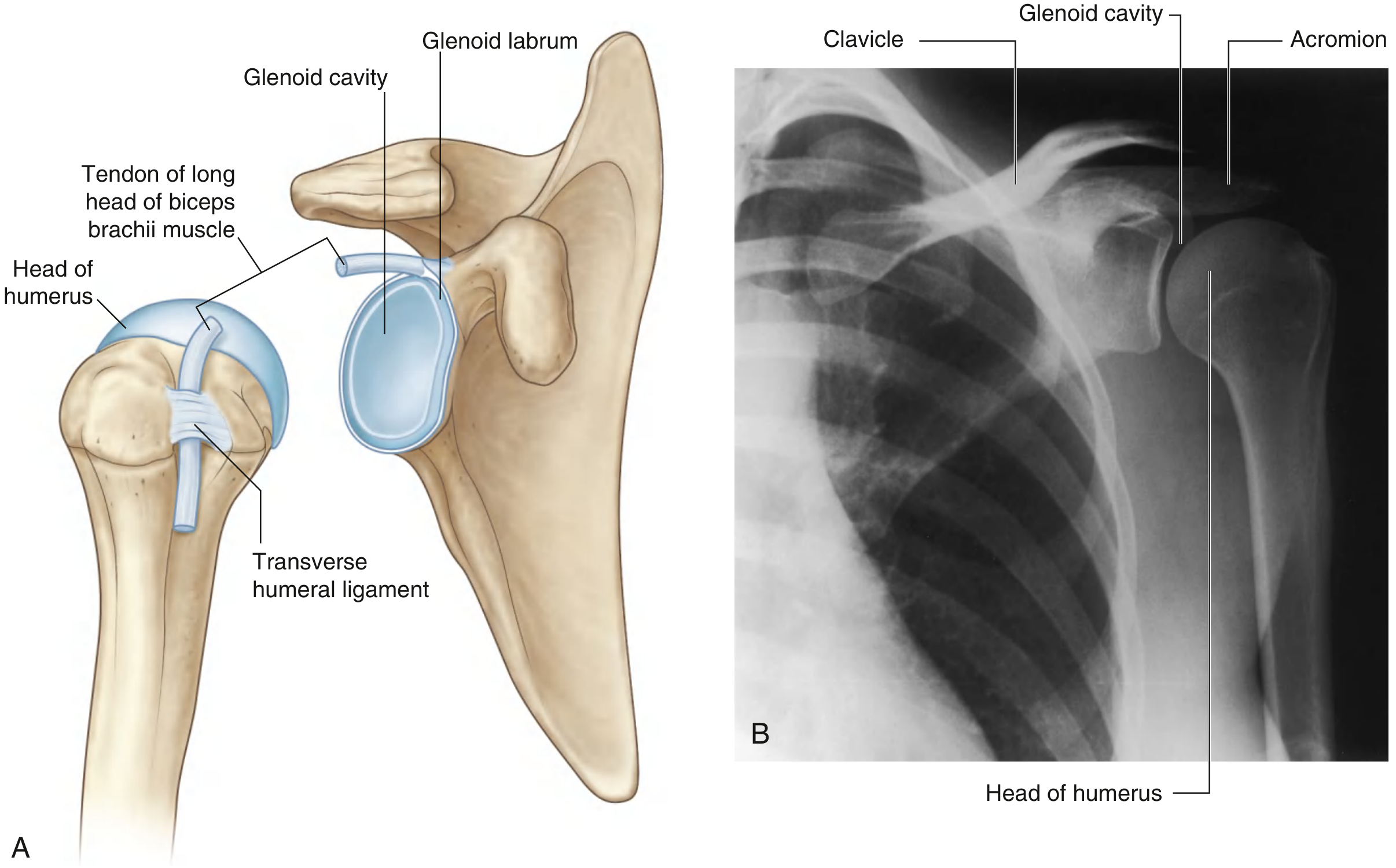
Fig. 7.25 - Glenohumeral joint articular surfaces and radiograph (Gray's Anatomy for Students)
Articular Surfaces
- Humeral head covered in hyaline cartilage; much larger than the glenoid
- Glenoid cavity covered in hyaline cartilage; only ~25-30% of the humeral head contacts it at any time
Glenoid Labrum
- A fibrocartilaginous rim that attaches to the glenoid margin
- Deepens and expands the glenoid cavity
- Superiorly, it is continuous with the tendon of the long head of biceps brachii (which attaches to the supraglenoid tubercle)
- Increases joint stability; torn in anterior dislocations (Bankart lesion)
Joint Capsule
Fibrous membrane:
- Attaches to the glenoid cavity margin (outside the glenoid labrum) and to the anatomical neck of the humerus
- Medially, the attachment extends inferiorly onto the shaft (creating a redundant fold that accommodates abduction)
- Thickened in three locations to form the glenohumeral ligaments
Synovial membrane:
- Attaches to articular margins, lines the fibrous capsule
- Loose inferiorly - this redundant portion accommodates abduction
- Protrudes through capsule apertures to form bursae (e.g., subtendinous bursa of subscapularis)
- Wraps around the long head of biceps tendon within the joint, then extends along it into the intertubercular sulcus
Ligaments of the Glenohumeral Joint
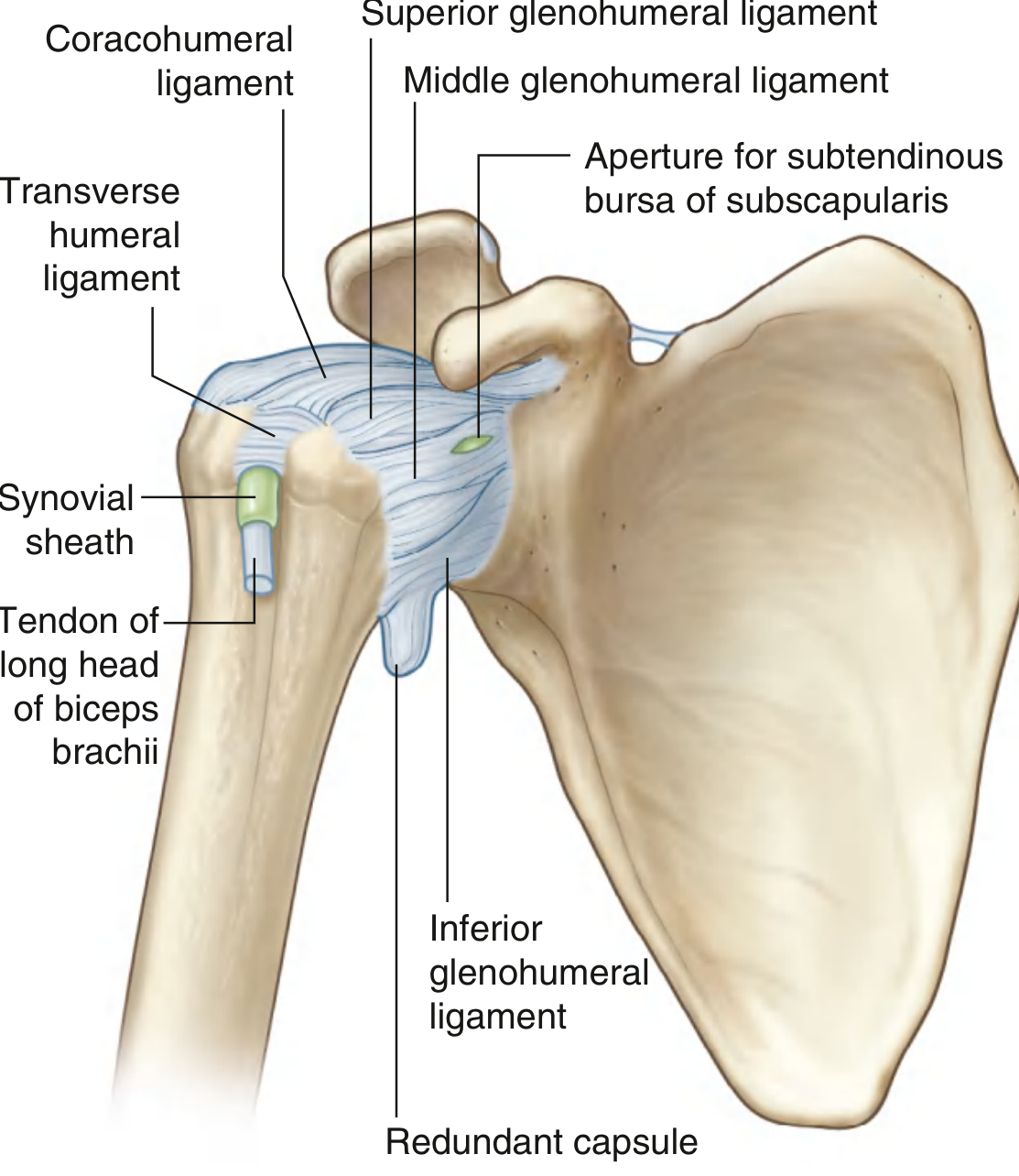
Fig. 7.27 - Capsule and ligaments of the right glenohumeral joint (Gray's Anatomy for Students)
| Ligament | Attachments | Function |
|---|---|---|
| Superior glenohumeral ligament | Superomedial glenoid margin → lesser tubercle | Restrains inferior translation with arm at side |
| Middle glenohumeral ligament | Superomedial glenoid margin → lesser tubercle | Restrains anterior translation at 45-60° abduction |
| Inferior glenohumeral ligament | Glenoid margin → anatomical neck (inferior) | Primary restraint to anterior/posterior instability at 90° abduction; most important stabilizer |
| Coracohumeral ligament | Base of coracoid process → greater tubercle | Resists inferior translation; limits extension and external rotation |
| Transverse humeral ligament | Greater tubercle → lesser tubercle | Holds long head of biceps in the intertubercular sulcus |
Coraco-Acromial Arch
- Formed by the coracoid process, coraco-acromial ligament, and acromion
- Forms a protective arch superior to the humeral head
- The subacromial space lies beneath this arch; contains supraspinatus tendon and subacromial bursa
Bursae
Four main bursae are associated with the glenohumeral joint:
- Subacromial (subdeltoid) bursa - between the acromion/deltoid and supraspinatus/capsule; does NOT directly communicate with the joint cavity in normal anatomy. Clinically the most important - becomes inflamed in impingement.
- Subtendinous bursa of subscapularis - between subscapularis tendon and joint capsule; communicates with the articular cavity through an aperture
- Subcoracoid bursa - between the coracoid process and joint capsule
- Subcutaneous acromial bursa - between acromion and skin
Blood Supply
- Anterior and posterior circumflex humeral arteries (branches of axillary artery)
- Suprascapular artery (branch of subclavian/thyrocervical trunk)
Nerve Supply
- Axillary nerve (C5, C6)
- Suprascapular nerve (C5, C6)
- Lateral pectoral nerve (C5, C6, C7)
Movements
| Movement | Primary Muscles |
|---|---|
| Flexion (0-180°) | Deltoid (anterior), pectoralis major, coracobrachialis, biceps brachii |
| Extension | Deltoid (posterior), latissimus dorsi, teres major |
| Abduction | Deltoid (major), supraspinatus (initiates first 15°) |
| Adduction | Pectoralis major, latissimus dorsi, teres major |
| Medial rotation | Subscapularis, pectoralis major, latissimus dorsi, teres major, deltoid (anterior) |
| Lateral rotation | Infraspinatus, teres minor, deltoid (posterior) |
Key rule: Full abduction to 180° requires contributions from both the glenohumeral joint (~120°) and the scapulothoracic articulation (~60°) - the scapulohumeral rhythm (2:1 ratio of GH to scapulothoracic movement).
4. Rotator Cuff
The rotator cuff is formed by four muscles whose tendons blend with and reinforce the fibrous capsule of the glenohumeral joint. The mnemonic is SITS:
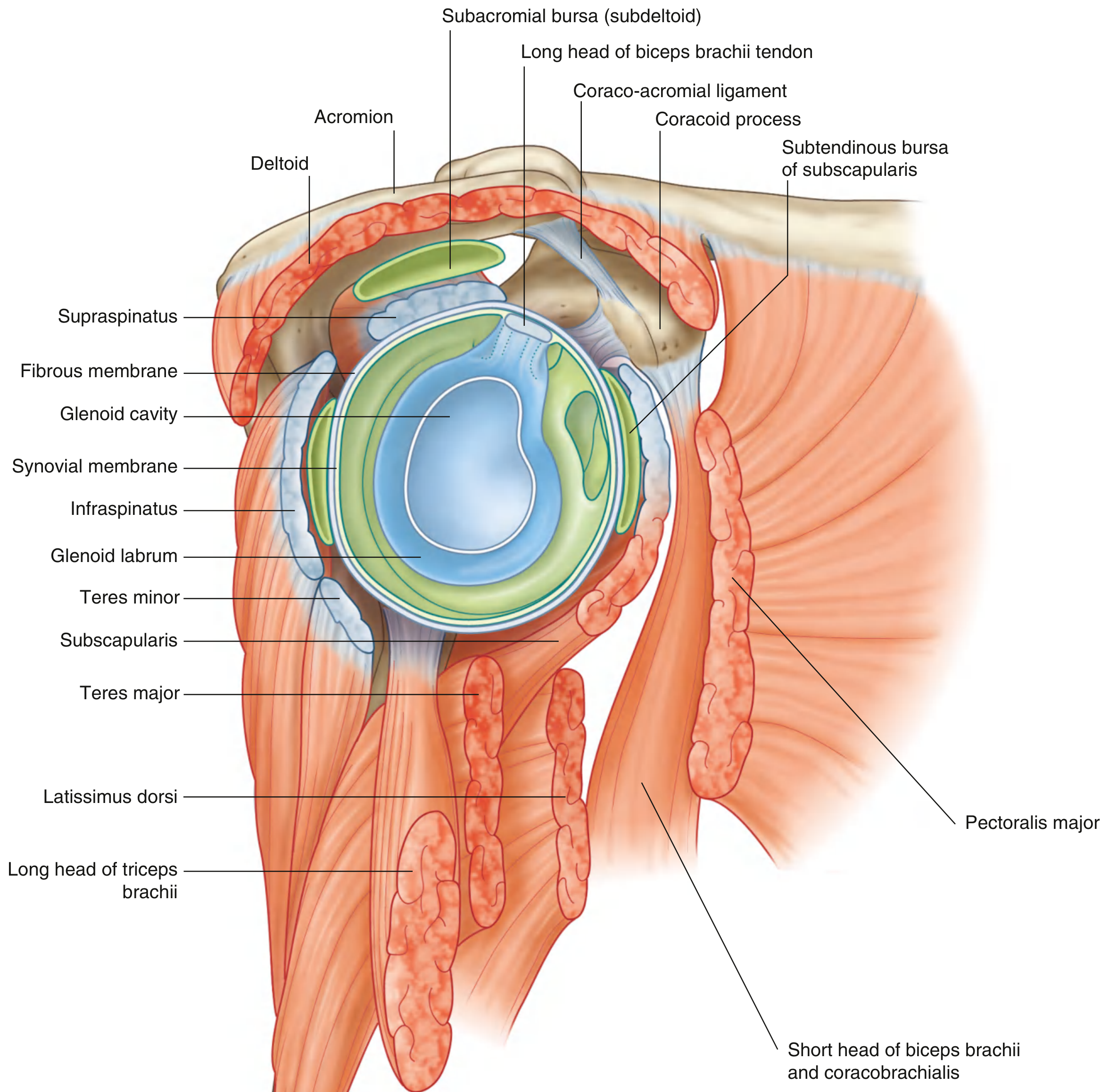
Fig. 7.28 - Cross-section of the glenohumeral joint showing rotator cuff muscles (Gray's Anatomy for Students)
| Muscle | Origin | Insertion | Nerve | Action |
|---|---|---|---|---|
| Supraspinatus | Supraspinous fossa (medial 2/3) | Superior facet, greater tubercle | Suprascapular (C5, C6) | Abduction (initiates); stabilizes GH joint |
| Infraspinatus | Infraspinous fossa (medial 2/3) | Middle facet, greater tubercle | Suprascapular (C5, C6) | Lateral rotation; stabilizes GH joint |
| Teres minor | Lateral border of scapula (upper 2/3) | Inferior facet, greater tubercle | Axillary (C6, C7) | Lateral rotation; stabilizes GH joint |
| Subscapularis | Subscapular fossa | Lesser tubercle | Upper & lower subscapular (C5, C6, C7) | Medial rotation; stabilizes GH joint |
Function: The rotator cuff creates a compressive force that holds the humeral head into the glenoid fossa, acting as a dynamic stabilizer. It surrounds the posterior, superior, and anterior aspects of the joint. The inferior aspect has no rotator cuff coverage - hence the most common direction of dislocation is anteroinferior.
5. Muscles of the Shoulder Region
Superficial Layer
Trapezius
- Origin: Superior nuchal line, external occipital protuberance, ligamentum nuchae, spinous processes C7-T12
- Insertion: Posterior border of lateral 1/3 of clavicle, acromion, superior edge of spine of scapula
- Nerve: Accessory nerve (CN XI) (motor); C3, C4 (proprioception)
- Action: Elevates scapula (upper fibers), retracts scapula (middle fibers), depresses scapula (lower fibers), rotates scapula during arm abduction above horizontal
- Clinical note: Test by asking patient to shrug against resistance
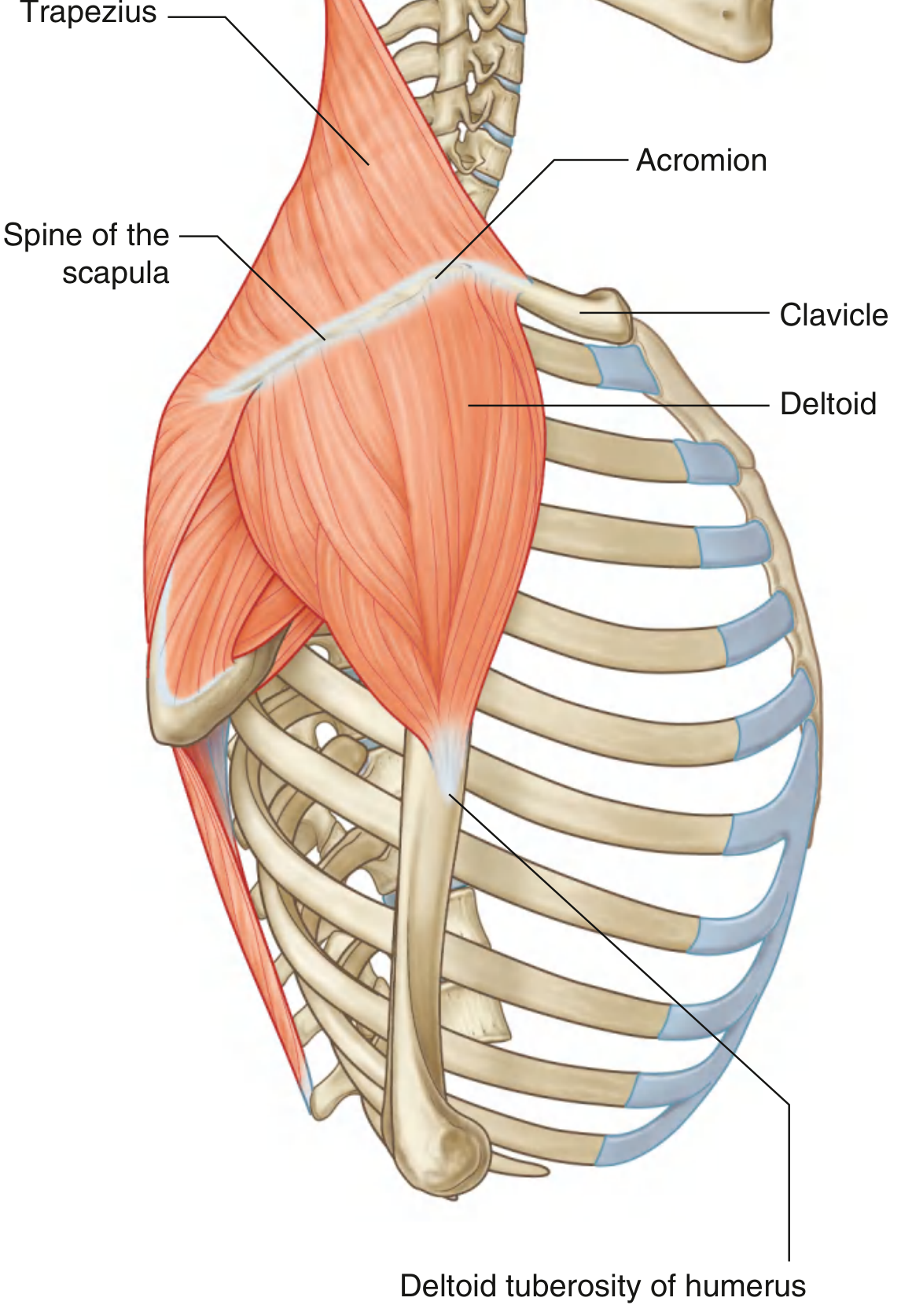
Fig. 7.35 - Trapezius and deltoid muscles (Gray's Anatomy for Students)
Deltoid
- Large, triangular muscle forming the characteristic contour of the shoulder
- Origin: Continuous U-shaped line - anterior border of lateral 1/3 clavicle, lateral margin of acromion, inferior edge of spine of scapula
- Insertion: Deltoid tuberosity of humerus
- Nerve: Axillary nerve (C5, C6) - enters via the quadrangular space with the posterior circumflex humeral artery
- Action: Major abductor of the arm; anterior fibers flex and medially rotate; posterior fibers extend and laterally rotate
Deep Layer - Posterior Scapular Region
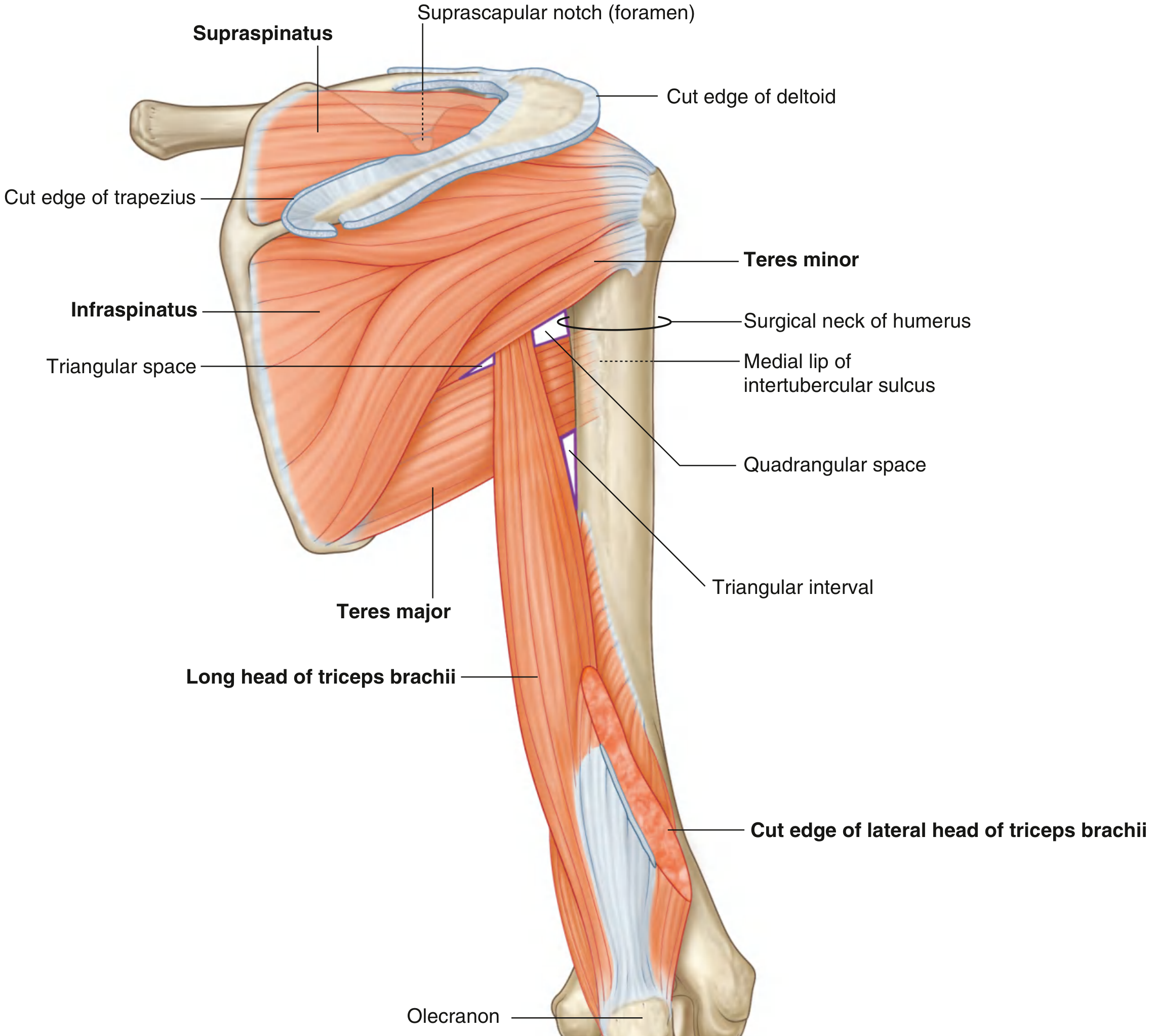
Fig. 7.37 - Posterior scapular region with muscles and spaces (Gray's Anatomy for Students)
Levator scapulae
- Origin: Transverse processes of C1-C4
- Insertion: Medial border of scapula (superior angle to spine)
- Nerve: Dorsal scapular nerve; C3, C4 directly
- Action: Elevates scapula
Rhomboid minor and major
- Origin: Ligamentum nuchae + C7, T1 spines (minor); T2-T5 spines (major)
- Insertion: Medial border of scapula
- Nerve: Dorsal scapular nerve (branch of brachial plexus)
- Action: Retract and elevate the scapula
Teres major
- Origin: Posterior surface of inferior angle of scapula
- Insertion: Medial lip of intertubercular sulcus
- Nerve: Inferior subscapular nerve (C6, C7)
- Action: Medial rotation and extension of the arm
- Note: NOT a rotator cuff muscle; does not blend with the joint capsule
Serratus anterior
- Origin: Lateral surfaces of ribs 1-8
- Insertion: Costal surface of medial border of scapula
- Nerve: Long thoracic nerve (C5, C6, C7) - very long course, vulnerable to injury
- Action: Protracts scapula; holds medial border against thoracic wall; rotates scapula (with trapezius) for arm elevation above horizontal
- Clinical: Injury causes "winging of the scapula" (medial border protrudes posteriorly)
6. Gateways: Spaces and Foramina
These are passages through which neurovascular structures travel between regions.
Suprascapular Foramen
- Formed by the suprascapular notch + superior transverse scapular ligament
- Suprascapular nerve passes through the foramen
- Suprascapular artery and vein pass superior to the ligament (above the foramen)
- Mnemonic: "The army goes over the bridge, the nerves go under" (artery over, nerve under the ligament)
Quadrangular Space
Boundaries:
- Superior: Teres minor
- Inferior: Teres major
- Medial: Long head of triceps brachii
- Lateral: Surgical neck of humerus
Contents: Axillary nerve + posterior circumflex humeral artery and vein
Clinical: Axillary nerve injury in anterior shoulder dislocation (humeral head compresses nerve inferiorly as it passes through this space)
Triangular Space
Boundaries:
- Superior: Teres minor
- Inferior: Teres major
- Lateral: Long head of triceps brachii (medial margin)
Contents: Circumflex scapular artery and vein
Triangular Interval
Boundaries:
- Superior: Inferior margin of teres major
- Medial: Long head of triceps brachii (lateral margin)
- Lateral: Shaft of humerus
Contents: Radial nerve + profunda brachii artery (deep artery of arm)
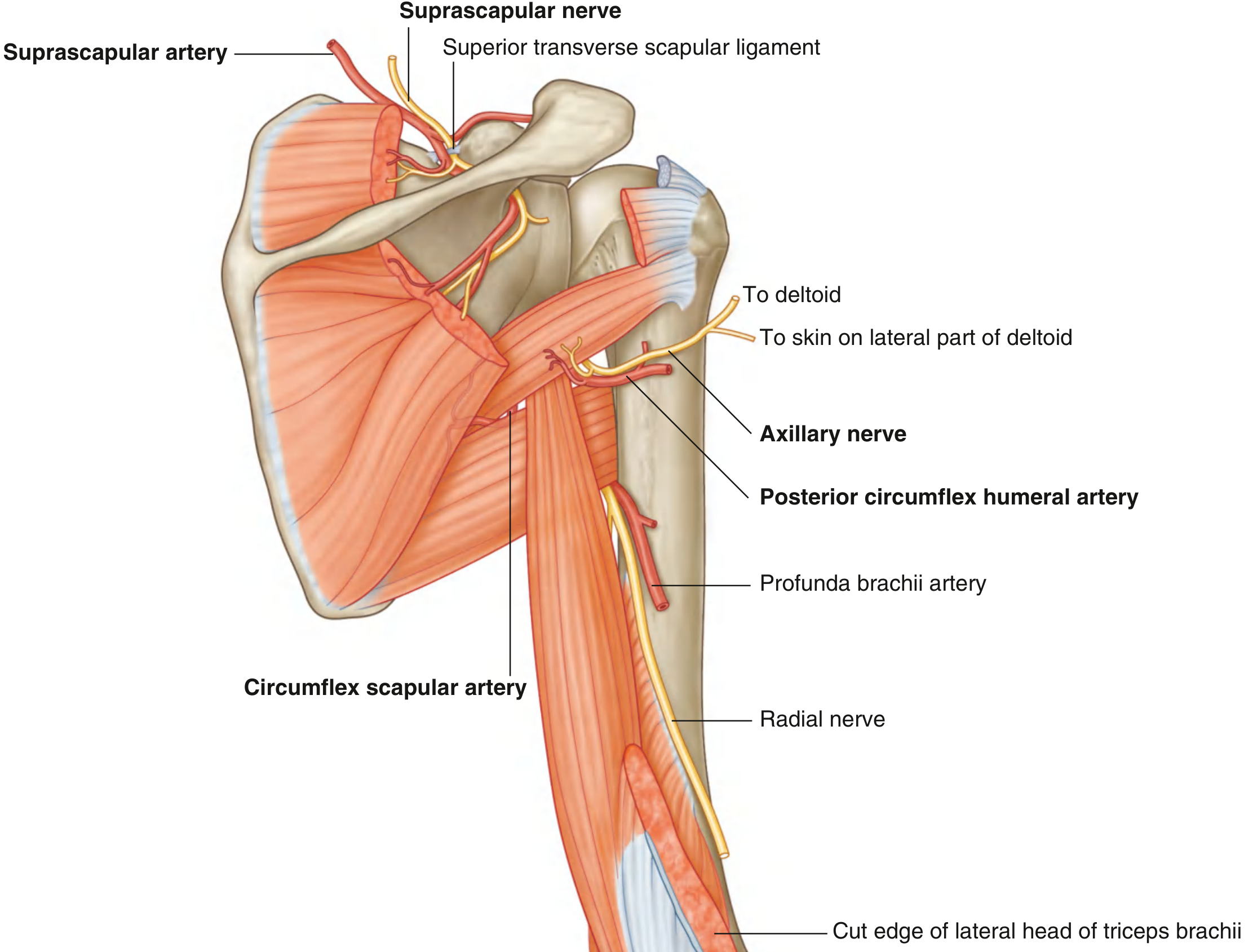
Fig. 7.38 - Neurovascular supply of the posterior scapular region (Gray's Anatomy for Students)
7. Acromioclavicular (AC) Joint
- Synovial plane joint between the lateral end of clavicle and the acromion
- Has an incomplete fibrocartilaginous articular disc (meniscus)
- Allows gliding movements during scapular rotation
Ligaments:
- AC ligament (fibrous capsule) - limits anterior-posterior translation
- Coracoclavicular ligament - the main suspensory ligament; has two parts:
- Conoid ligament (medial, cone-shaped) - limits superior displacement of clavicle
- Trapezoid ligament (lateral, quadrilateral) - limits lateral displacement
AC Joint Injury (Shoulder Separation):
- Minor injury: tears AC ligament only (Grade I-II) - coracoclavicular ligaments intact
- Severe injury: tears both AC and coracoclavicular ligaments (Grade III+) - clavicle elevated on X-ray
8. Sternoclavicular (SC) Joint
- The only synovial joint connecting the upper limb to the axial skeleton
- Between the medial end of clavicle, manubrium sterni, and first costal cartilage
- Has a complete fibrocartilaginous articular disc that divides the joint into two cavities
Ligaments:
- Anterior and posterior sternoclavicular ligaments
- Interclavicular ligament (between both clavicles across the jugular notch)
- Costoclavicular ligament (strongest; from first rib/costal cartilage to inferior clavicle)
Movements: Elevation/depression, protraction/retraction, rotation of clavicle
Dislocation:
- Anterior dislocation: more common
- Posterior dislocation: less common but dangerous - the clavicle can compress great vessels (subclavian/brachiocephalic), trachea, or esophagus in the root of the neck
9. Clinical Correlates
Glenohumeral Dislocation
- Most mobile joint = most commonly dislocated joint in the body
- Anterior (anteroinferior) dislocation (95%): Usually from a fall on an outstretched hand or forced external rotation. The humeral head moves inferiorly into the subcoracoid position.
- Risk of axillary nerve injury (deltoid weakness, loss of sensation over the "regimental badge" area of lateral deltoid)
- Bankart lesion: tear of the anteroinferior glenoid labrum (with or without bony fragment)
- Hill-Sachs lesion: compression fracture of the posterolateral humeral head from impaction on the glenoid rim
- Recurrent instability treated with capsular repair/Latarjet procedure (coracoid transfer)

Fig. 7.32 - Anteroinferior glenohumeral dislocation (Gray's Anatomy for Students)
- Posterior dislocation (<5%): Associated with epileptic seizures or electrocution (strong bilateral muscle contractions). Often missed on AP X-ray (requires axillary/Y-view).
Clavicle Fractures
- Most common site: middle third (80-85%)
- Mechanism: fall onto outstretched hand or direct blow
- Lateral third fractures are less common but may involve coracoclavicular ligaments
Rotator Cuff Pathology
- Supraspinatus is the most commonly affected tendon - passes through the subacromial space beneath the coraco-acromial arch (fixed dimensions)
- Impingement syndrome: Narrowing of the subacromial space causes repetitive mechanical irritation of the supraspinatus tendon during arm elevation. Causes include subacromial bone spurs, thickened AC ligament, subacromial bursitis, or muscle swelling.
- Tendinopathy: Poor blood supply to supraspinatus (critical zone ~1 cm from insertion) makes it susceptible to degenerative change; calcium can deposit (calcific tendinitis)
- Rotator cuff tear:
- Partial-thickness or full-thickness
- Most common in older patients (>40 years)
- Full-thickness tears may be asymptomatic
- MRI is gold standard for diagnosis
Subacromial (Subdeltoid) Bursitis
- Inflammation of the bursa between supraspinatus/deltoid and acromion
- Causes painful glenohumeral movements
- Treated with corticosteroid + local anesthetic injection under image guidance
Axillary Nerve Injury
- Most common with anterior glenohumeral dislocation or surgical neck of humerus fracture
- Results in: weakness of deltoid (abduction impaired), weakness of teres minor, loss of sensation over the lateral deltoid (upper lateral cutaneous nerve of arm)
- Test: Assess shoulder contour (loss of deltoid roundness in complete paralysis)
10. Summary: Key Nerve-Structure Relationships
| Nerve | Root | At-Risk When... | Tests |
|---|---|---|---|
| Axillary nerve | C5, C6 | Anterior GH dislocation, surgical neck fracture | Deltoid power (abduction), lateral deltoid sensation |
| Suprascapular nerve | C5, C6 | Suprascapular notch entrapment | Infraspinatus/supraspinatus power |
| Long thoracic nerve | C5, C6, C7 | Neck dissection, stab wound | Serratus anterior (scapular winging) |
| Accessory nerve (CN XI) | - | Posterior triangle surgery | Trapezius power (shoulder shrug) |
| Radial nerve | C5-C8 | Triangular interval, spiral groove | Wrist extension, triceps power |
Source: Gray's Anatomy for Students, p. 826-839 | General Anatomy and Musculoskeletal System (THIEME Atlas of Anatomy) | Rockwood and Green's Fractures in Adults, 10th ed. 2025
This is a shared conversation. Sign in to Orris to start your own chat.