Dysgerminoma treatment
Reading File
Finding Sources
Searching PubMed
dysgerminoma treatment chemotherapy
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Excellent - I have everything I need for a comprehensive answer.
Dysgerminoma - Treatment
Dysgerminoma is the most common malignant ovarian germ cell tumor (~30-40% of all germ cell malignancies), occurring predominantly in women aged 10-30 years. It is the ovarian counterpart of testicular seminoma and shares its excellent chemosensitivity.
Management Algorithm
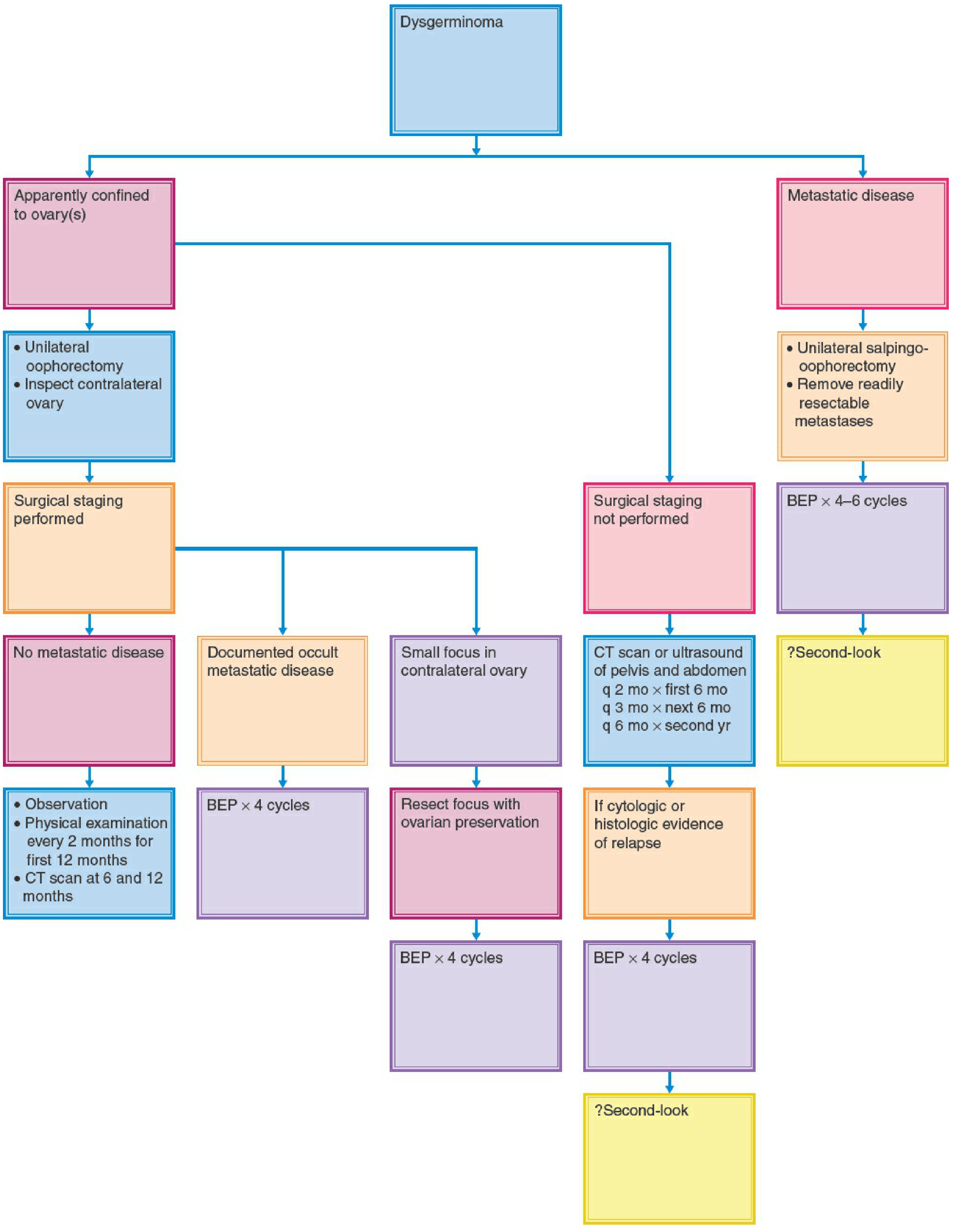
1. Surgery
Surgery is the primary treatment and serves two purposes: resection and staging.
Minimum Operation
- Unilateral oophorectomy (or salpingo-oophorectomy) - fertility-sparing surgery is the standard because the tumor primarily affects young women.
- The contralateral ovary, fallopian tube, and uterus should be preserved even in the presence of metastatic disease, given the excellent chemosensitivity.
Staging Procedure
A careful surgical staging should include:
- Inspection and palpation of all peritoneal surfaces
- Biopsy of any suspicious lesions
- Unilateral pelvic lymphadenectomy + para-aortic node sampling (para-aortic spread to the renal vessel level is characteristic)
- Inspection of the contralateral ovary - dysgerminoma is the only germ cell tumor with significant bilateral rates (10-15%)
Special Considerations
- Gonadal dysgenesis / Y chromosome: Both gonads must be removed (>50% risk of malignancy in gonadoblastomas left in situ), but the uterus can be preserved for future embryo transfer.
- Bulky resectable disease (e.g., omental cake): Cytoreductive resection is reasonable even if of unproven survival benefit.
2. Stage I Disease - Observation vs. Adjuvant Therapy
About 65% of dysgerminomas are Stage I at diagnosis.
| Situation | Approach |
|---|---|
| Stage I, fully staged, no adverse features | Observation (physical exam q2 months × 12 months; CT at 6 and 12 months) |
| Stage I, surgical staging NOT performed | Close surveillance with CT/US pelvis+abdomen q2mo × 6mo, q3mo × 6mo, q6mo × year 2 - then BEP if relapse |
| Capsular rupture or higher stage | Adjuvant chemotherapy |
| Small contralateral ovarian focus | Resect with ovarian preservation, then BEP ×4 |
Stage I dysgerminoma does not require adjuvant chemotherapy when properly staged and there are no adverse features.
3. Chemotherapy
Platinum-based chemotherapy is the treatment of choice for metastatic or high-risk disease, with the major advantage of preserving fertility (unlike radiation).
Standard Regimen: BEP
| Drug | Dose/Schedule |
|---|---|
| Bleomycin | 30,000 IU on days 1, 8, 15 every 3 weeks |
| Etoposide | 100 mg/m²/day × 5 days every 3 weeks |
| Cisplatin | 20 mg/m²/day × 5 days (or 100 mg/m²/day × 1 day) every 3 weeks |
- Stage I (occult metastases): BEP × 3-4 cycles
- Advanced disease (Stages III-IV): BEP × 4-6 cycles
Outcomes with BEP
20 evaluable patients with Stages III-IV dysgerminoma treated in GOG protocols: 19/20 alive and disease-free at 6-68 months follow-up. This confirms that even advanced-stage, incompletely resected dysgerminoma has an excellent prognosis with EP-based chemotherapy.
Alternative Regimens
- EP (etoposide + cisplatin) - used when bleomycin toxicity is a concern
- EC (etoposide + carboplatin) - alternative, used in select settings
- VBP (vinblastine, bleomycin, cisplatin) - older regimen, rarely used now
- VAC (vincristine, actinomycin D, cyclophosphamide) - historical; VAC consolidation after BEP is no longer used
4. Radiation Therapy
- Dysgerminomas are exquisitely radiation-sensitive (doses of 2,500-3,500 cGy can cure even gross metastatic disease).
- However, radiation almost always causes permanent infertility and is rarely used as first-line treatment in the modern era.
- BEP chemotherapy is at least as effective without the fertility cost.
- Radiation may still be considered in recurrent/refractory disease after chemotherapy failure.
5. Tumor Markers
Monitor throughout treatment and follow-up:
- LDH - most useful marker for pure dysgerminoma
- beta-hCG - elevated when syncytiotrophoblastic giant cells are present (~10-15% of cases)
- AFP - should be normal in pure dysgerminoma; elevation suggests mixed germ cell tumor (EST component), which changes management
- CA-125 - less specific
6. Recurrent Disease
- Recurrence after surgery alone responds well to BEP
- Recurrence after BEP: use salvage regimens (TIP - paclitaxel/ifosfamide/cisplatin, or high-dose chemotherapy with stem cell rescue)
- Second-look surgery: its role is uncertain (?second-look noted in advanced disease, but not standard)
7. Prognosis
| Stage | 5-Year Survival |
|---|---|
| Stage I | >95% |
| Stage II-III | 85-95% with BEP |
| Stage IV | ~75-85% with BEP |
Overall, dysgerminoma has the best prognosis of all malignant ovarian germ cell tumors, and even advanced disease is potentially curable.
Sources:
- Berek & Novak's Gynecology, pp. 2381-2387
- Harrison's Principles of Internal Medicine, 22E, p. 2171
Recent Literature Note: A 2026 systematic review (PMID 41317609) addresses post-treatment hormone replacement therapy and fertility preservation in Swyer syndrome with dysgerminoma - relevant for the subset of patients with gonadal dysgenesis requiring bilateral gonadectomy.
This is a shared conversation. Sign in to Orris to start your own chat.