Tear sensation from neck vertebra to left arm, forearm and index finger tell me which nerve can be comprase with photo
Reading File
Finding Sources
Finding Sources
Searching the Web
C6 nerve root compression cervical radiculopathy dermatome diagram arm index finger
Reading File
Finding Sources
Searching the Web
C6 nerve root dermatome diagram cervical radiculopathy anatomy photo
Loading Image
Loading Image
Loading Image
Here is a complete answer with visuals from the medical library and anatomy references:
C6 Nerve Root Compression - Cervical Radiculopathy
The Nerve: C6 Root (compressed at the C5-C6 disc level)
Your symptom pattern - tearing pain from the neck, radiating down the arm, forearm, and into the index finger - is the classic presentation of C6 nerve root compression. This is the most common level of cervical radiculopathy.
Dermatome Map (C6 highlighted in blue)
The image below shows how each cervical nerve root maps to a skin region. Notice C6 covers the radial (outer) forearm, thumb, and index finger - exactly your symptom distribution:

Anatomy of the Trapped Nerve
At the C5-C6 level, the disc herniates or bone spurs form, compressing the C6 nerve root as it exits the foramen:

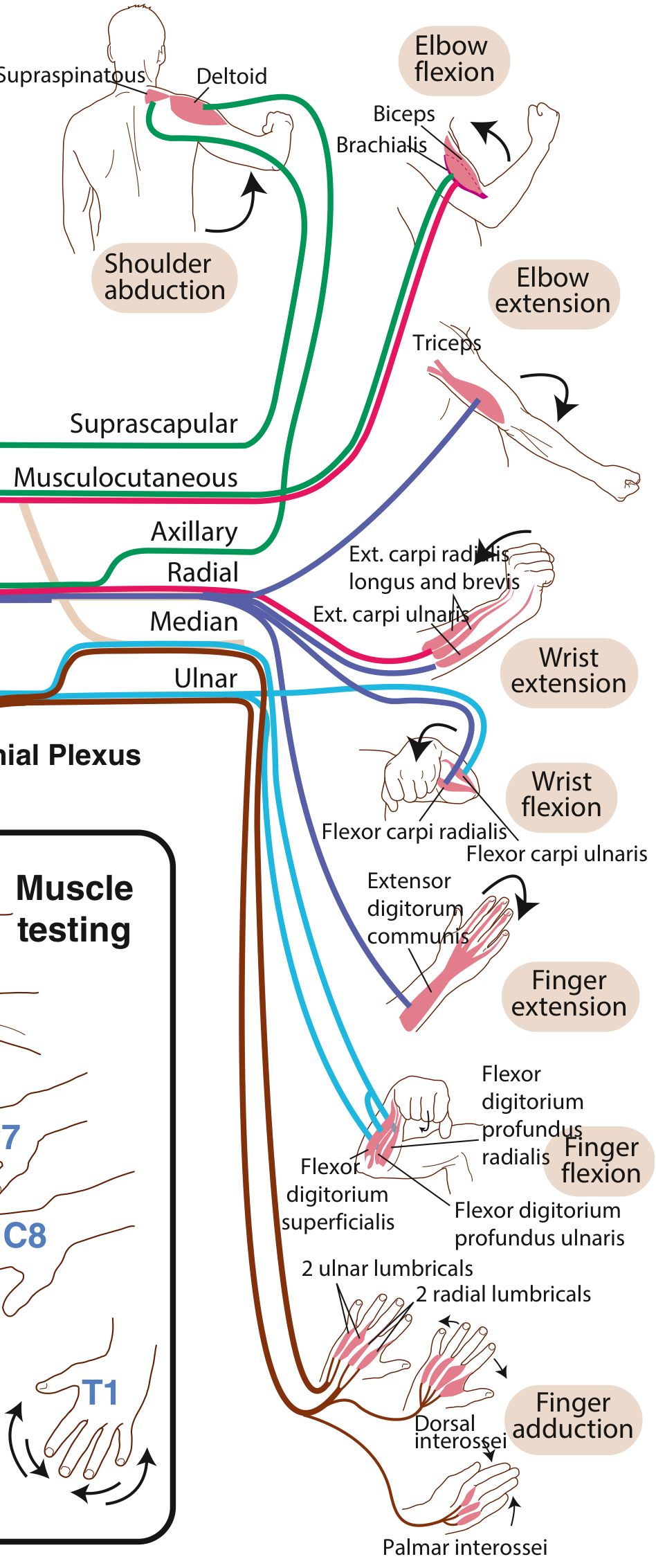
Brachial Plexus - Muscle and Nerve Connections
This diagram (from Miller's Review of Orthopaedics) shows how the brachial plexus connects cervical roots to muscles - C6 feeds the biceps, brachioradialis, and wrist extensors:
Complete Cervical Root Compression Table
From Miller's Review of Orthopaedics, Table 8.2:
| Disc Level | Nerve Root | Muscles Affected | Sensory Loss | Reflex Lost |
|---|---|---|---|---|
| C3-C4 | C4 | Scapular muscles | Lateral neck, shoulder | None |
| C4-C5 | C5 | Deltoid, biceps | Lateral arm | Biceps |
| C5-C6 (most common) | C6 | Wrist extensors, biceps, triceps (supination) | Radial forearm, thumb, index finger | Brachioradialis |
| C6-C7 | C7 | Triceps, wrist flexors (pronation) | Middle finger | Triceps |
| C7-T1 | C8 | Finger flexors, interossei | Ulnar hand, ring and small finger | None |
| T1-T2 | T1 | Interossei | Ulnar forearm | None |
Key Clinical Features of C6 Compression
| Feature | Finding |
|---|---|
| Pain pattern | Neck → shoulder → outer arm → radial forearm → thumb + index finger |
| Sensory loss | Thumb and index finger, radial forearm |
| Weakness | Wrist extension, biceps, forearm supination |
| Reflex lost | Brachioradialis (the hallmark reflex for C6) |
| Provocative test | Spurling's test (neck extension + rotation toward painful side reproduces arm pain) |
| Relieving sign | Shoulder abduction sign - placing the hand on top of the head reduces pain (reduces nerve tension) |
Common Causes
- Disc herniation at C5-C6 (most common in younger patients, acute onset)
- Cervical spondylosis (bone spurs + foraminal narrowing, common in older patients, gradual onset)
- Foraminal stenosis (degenerative narrowing of the exit canal for the nerve)
Quick Memory Trick
- Index finger numb → C6
- Middle finger numb → C7
- Ring + little finger numb → C8
Your index finger involvement points directly at C6, and the brachioradialis reflex test at the wrist is the key clinical sign to check. An MRI of the cervical spine at the C5-C6 level will confirm the compression.
In this case when pt neck down,tear sensation present till the finger and pain is very mild
Finding Sources
Finding Sources
Searching the Web
Lhermitte sign neck flexion electric shock sensation fingers spine causes diagnosis
Reading File
Reading File
Loading Image
This changes the diagnosis significantly. The key finding here is not radiculopathy anymore.
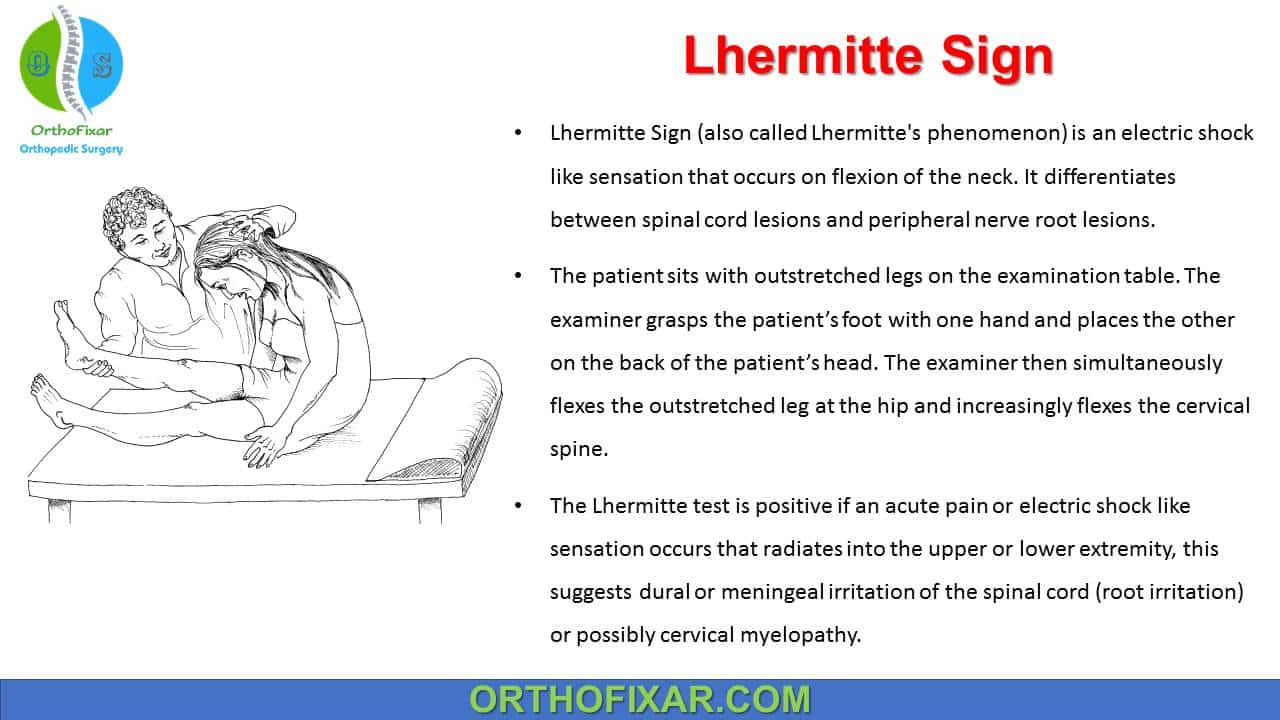
Lhermitte's Sign (Lhermitte's Phenomenon)
What It Is
When neck flexion (chin to chest) triggers a sudden electric shock / tearing sensation radiating down the spine into the arms and fingers, with minimal pain - this is called Lhermitte's Sign (pronounced "lair-MEET's sign"), also known as the "Barber Chair Phenomenon".
Why It Happens - The Mechanism
The sensation originates from the posterior columns of the cervical spinal cord - the sensory tracts that carry vibration and proprioception. When these demyelinated or damaged fibers are mechanically stretched by neck flexion, they fire abnormally, generating the shock-like sensation.
"An electric shock-like sensation provoked by neck flexion that spreads to the arms, down the spine, and even into the legs is thought to originate in the posterior columns of the cervical spinal cord (Lhermitte sign)."
- Bradley and Daroff's Neurology in Clinical Practice
Key Distinction from Radiculopathy
| Feature | Lhermitte's Sign | C6 Radiculopathy |
|---|---|---|
| Trigger | Neck flexion (chin to chest) | Neck extension/rotation (Spurling's) |
| Pain level | Mild / transient - lasts seconds | Moderate to severe, persistent |
| Sensation quality | Electric shock, buzzing, tearing | Aching, burning, lancinating |
| Location of problem | Spinal cord (posterior columns) | Nerve root (C5-C6 foramen) |
| Duration | Lasts only seconds after movement | Can be constant or prolonged |
| Fingers | Both arms/fingers often affected | Usually one side, dermatomal pattern |
Causes - Important Red Flags
Lhermitte's sign is not a diagnosis itself - it is a sign of a posterior cervical cord lesion. The causes must be investigated urgently:
| Cause | Notes |
|---|---|
| Multiple Sclerosis (MS) | Most common cause - demyelinating plaques in cervical cord |
| Cervical Spondylotic Myelopathy | Cord compression from disc/bone spurs - mechanical |
| Radiation myelopathy | After neck/head radiation therapy |
| Subacute Combined Degeneration | Vitamin B12 deficiency damaging posterior columns |
| Foramen magnum tumors | Meningioma, neurofibroma compressing upper cord |
| Transverse myelitis | Inflammatory cord lesion |
| Chiari malformation | Downward herniation of cerebellum |
| Atlantoaxial subluxation | E.g., in rheumatoid arthritis |
Clinical Bottom Line
This patient's symptom pattern - neck DOWN → tearing/electric shock → fingers, mild pain - is a positive Lhermitte's sign, pointing to a spinal cord lesion (not just a nerve root). The most important next step is:
- MRI cervical spine with contrast - look for MS plaques, cord compression, tumor
- Vitamin B12 level - to rule out subacute combined degeneration
- Neurological exam - check for upper motor neuron signs (hyperreflexia, Babinski, spasticity, gait disturbance) which would confirm myelopathy
- Ophthalmology referral - if MS suspected (optic neuritis)
The presence of upper motor neuron signs + Lhermitte's sign = myelopathy until proven otherwise → urgent MRI.
This is a shared conversation. Sign in to Orris to start your own chat.