Cushing syndrome
Reading File
Finding Sources
Searching PubMed
"Cushing syndrome"[MeSH Terms] AND diagnosis
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have all the content needed for a comprehensive, well-illustrated answer. Let me compile it.
Cushing Syndrome
Cushing syndrome is the clinical state resulting from chronic exposure to excess glucocorticoids, regardless of the source. It is distinct from Cushing disease, which refers specifically to hypercortisolism caused by an ACTH-secreting pituitary adenoma. Endogenous Cushing syndrome is rare - affecting 5 to 10 individuals per million - but exogenous (iatrogenic) glucocorticoid use is far more common.
Etiology and Classification
The causes are best divided into three groups:
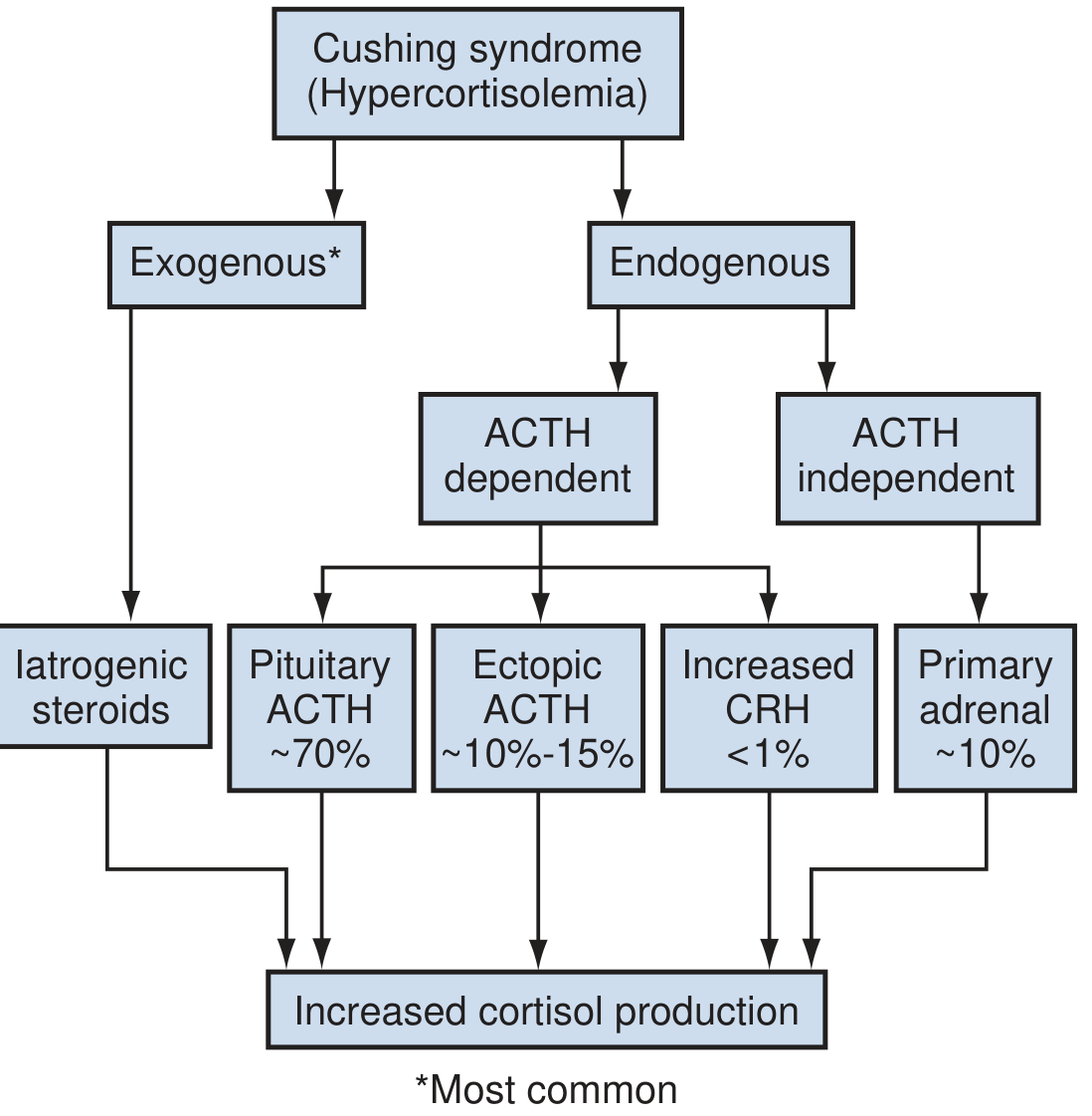
1. Exogenous (Iatrogenic) - Most Common Overall
Synthetic glucocorticoids used to treat inflammatory conditions are the single most common cause worldwide. Even low doses taken orally, topically, or by inhalation can produce the syndrome. Herbal remedies and nasal sprays can be covert sources. - Campbell Walsh Wein Urology, p. 3134
2. ACTH-Dependent (80-85% of endogenous cases)
| Sub-type | Proportion | Mechanism |
|---|---|---|
| Cushing disease (pituitary corticotroph adenoma) | ~70% of endogenous | Pituitary microadenoma secretes excess ACTH. Up to 2/3 of patients are female. Macroadenomas (≥1 cm) in only ~5% of cases. |
| Ectopic ACTH syndrome | ~10-15% of endogenous | ACTH produced by non-pituitary tumors - usually neuroendocrine tumors, bronchogenic carcinoma (small cell), or carcinoid. Nearly always malignant. |
| Ectopic CRH syndrome | <1% | Extremely rare |
3. ACTH-Independent (~15-20% of endogenous cases)
- Primary adrenal adenoma - ~90% of primary adrenal cases; ACTH suppressed (≤5 pg/mL)
- Adrenocortical carcinoma (ACC) - <10%
- Bilateral micronodular or macronodular hyperplasia - <1%
- Primary pigmented nodular adrenocortical disease (PPNAD) - occurs in 30% of Carney complex patients
Sources: Sabiston Textbook of Surgery, p. 1569; Campbell Walsh Wein Urology, p. 3135; Adams and Victor's Principles of Neurology, 12th Ed.
Clinical Features
The clinical picture reflects widespread glucocorticoid excess across multiple organ systems.

Same patient before (A) and one year after (B) developing Cushing syndrome, and (C) extensive purple abdominal striae.
Cardinal Features
- Central (truncal) obesity - face, neck, trunk, and abdomen; limbs spared
- Moon face - wide, round face
- Buffalo hump - dorsocervical fat pad (can be treated with liposuction)
- Purple-red striae - atrophic, wide, purplish; abdomen, buttocks, thighs, breasts, upper arms
- Skin fragility - easy bruising, thin "cigarette paper" texture, Liddle sign (skin peels with adhesive tape removal)
- Proximal muscle weakness (myopathy) - a prominent neurological feature
- Hypertension - present in >70% of cases; leads to fivefold excess cardiovascular mortality if untreated
- Osteoporosis - dorsal kyphosis, back pain, vertebral fractures
- Glucose intolerance/Diabetes mellitus - develops in ~20%
- Hypertrichosis and acne (especially in women), thinning of scalp hair
- Hypokalemia - more pronounced in ectopic ACTH syndrome
- Menstrual irregularities and loss of libido
- Psychological disturbances - depression, cognitive impairment
Ectopic ACTH - Distinguishing Features
Ectopic ACTH syndrome tends to present with more rapid onset, greater proximal weakness, more prominent skin pigmentation (from ACTH's MSH-like activity), more severe hypokalemia and hypertension, and ACTH levels typically >20 pg/mL that are not suppressed by dexamethasone. - Adams and Victor's Neurology, p. 395
HPA Axis Physiology (Relevant Background)
- Hypothalamus releases CRH (under circadian control from the suprachiasmatic nucleus) → stimulates anterior pituitary corticotrophs → release ACTH → adrenal zona fasciculata secretes up to 20 mg cortisol/day
- Cortisol completes the negative feedback loop by inhibiting CRH and ACTH
- Cortisol peaks ~1 hour after waking; nadir around midnight - loss of this circadian rhythm is a hallmark of Cushing syndrome
- Without ACTH, adrenal cortical cells undergo apoptosis (except mineralocorticoid-producing zona glomerulosa cells)
Diagnosis
Diagnosis proceeds in two steps: (1) confirm excess cortisol, then (2) identify the cause.
Step 1 - Confirm Hypercortisolism (Screening Tests)
| Test | Details |
|---|---|
| 24-hour urinary free cortisol (UFC) | Should be done at least twice. Unequivocally elevated (>3× normal) confirms the diagnosis. Normal 24-hr cortisol: ~12-40 µg; some assays allow up to 100 µg. |
| Late-night salivary cortisol | Loss of nocturnal nadir. A cutoff of 550 ng/mL has sensitivity 93%, specificity 100%. Two measurements recommended. |
| 1-mg overnight dexamethasone suppression test (DST) | 1 mg dexamethasone at 11 PM; cortisol measured at 8 AM. Level <50 nmol/L essentially rules out Cushing syndrome (except iatrogenic). |
| Low-dose DST (2-day) | 0.5 mg every 6 hours for 48 hours; used for confirmation. |
Step 2 - Determine the Cause
Measure plasma ACTH:
- Undetectable ACTH (≤5 pg/mL) → ACTH-independent → CT/MRI adrenal imaging
- Normal or elevated ACTH → ACTH-dependent → pituitary MRI + high-dose DST
High-dose DST (8 mg):
- Corticotroph adenomas (Cushing disease) are suppressed → ≥90% reduction in urinary cortisol
- Ectopic ACTH sources lack feedback inhibition → no suppression
- Only 60-70% sensitivity, so not used in isolation
Inferior Petrosal Sinus Sampling (IPSS) - Gold Standard for ACTH-dependent:
- ACTH measured in inferior petrosal sinus (drains pituitary) vs. peripheral blood, after CRH stimulation
- Central : peripheral ACTH gradient (>2 basal or >3 post-CRH) = Cushing disease
- Absence of gradient = ectopic ACTH source → CT chest/abdomen, somatostatin receptor scintigraphy
Pituitary MRI:
- Only ~50% of corticotroph microadenomas visible
- A mass >6 mm with high-dose DST suppression justifies proceeding to pituitary surgery
Sources: Sabiston Textbook of Surgery, p. 1569-1570; Campbell Walsh Wein Urology; Adams and Victor's Neurology
Treatment
Treatment is directed at the underlying cause.
Cushing Disease (Pituitary Adenoma)
- Transsphenoidal pituitary microsurgery - treatment of choice for microadenomas not extending beyond the sella
- Remission confirmed by subnormal morning cortisol on postoperative day 1-2
- If surgery fails or is not feasible: stereotactic radiosurgery (gamma knife), or medical therapy
- Bilateral adrenalectomy is a last resort (Nelson syndrome - pituitary tumor enlargement - can follow)
Primary Adrenal Disease
- Unilateral adrenalectomy for solitary adenoma or carcinoma
- Perioperative stress-dose steroids: hydrocortisone 100 mg IV every 8 hours for 24 hours
- Post-op steroid taper to physiologic replacement over weeks; HPA axis recovery may take >1 year
Ectopic ACTH Syndrome
- Resection of the ACTH-secreting tumor where possible
- Bilateral adrenalectomy if tumor localization fails
Medical Therapy (adjunct or bridge)
- Ketoconazole - inhibits adrenal steroidogenesis; used in treatment/diagnosis (also used in the low-dose DST for cortisol assay)
- Metyrapone, mitotane, etomidate - additional steroidogenesis inhibitors
- Mifepristone - glucocorticoid receptor antagonist
Exogenous Cushing Syndrome
- Taper and discontinue the causative glucocorticoid if clinically feasible
- Note: serum cortisol is very low in iatrogenic cases (adrenal suppression), so the overnight DST is not useful here
Post-operative Management
- All patients require glucocorticoid supplementation post-surgery (risk of adrenal crisis)
- HPA axis recovery can take 6 months to >1 year, especially with longer duration of disease
Sources: Sabiston Textbook of Surgery, p. 1570; Adams and Victor's Neurology; Campbell Walsh Wein Urology; Lippincott Pharmacology
Pseudo-Cushing Syndrome
Alcohol abuse can produce a clinical picture that closely mimics Cushing syndrome - the pseudo-Cushing syndrome. Chronic major depression can also elevate cortisol. Key distinguishing feature: correction of the underlying condition reverses biochemical abnormalities. - Andrews' Diseases of the Skin
Prognosis
When left untreated, Cushing syndrome carries fivefold excess mortality, primarily from cardiovascular complications (hypertension, diabetes, atherosclerosis). Early identification and treatment of the cause is therefore important. - Sabiston Textbook of Surgery
Recent evidence note: A 2024 meta-analysis (PMID 38888685) addresses the diagnostic challenge of differentiating true Cushing syndrome from non-neoplastic hypercortisolism (functional/pseudo-Cushing states). A separate 2024 meta-analysis (PMID 39086899) examined surgical vs. conservative approaches in mild autonomous cortisol secretion (formerly "subclinical Cushing"), supporting surgical management in select patients for metabolic benefit.
This is a shared conversation. Sign in to Orris to start your own chat.