Phyllode tumors
Reading File
Finding Sources
Searching PubMed
phyllodes tumor breast
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
I have all the material I need. Let me now compile the comprehensive answer.
Phyllodes Tumors
Overview
Phyllodes tumors are fibroepithelial breast neoplasms that arise from intralobular stroma. They account for roughly 2.5% of fibroepithelial lesions (and <0.5% of all breast tumors). The name comes from the Greek phyllodes ("leaf-like"), reflecting the characteristic bulbous, leaf-shaped stromal projections seen histologically and grossly.
They were originally termed cystosarcoma phyllodes by Johannes Muller in 1838, but that name is now abandoned because most are not truly cystic and not true sarcomas.
Pathogenesis / Molecular Biology
Like fibroadenomas, phyllodes tumors carry mutations in:
- MED12 (a transcriptional regulator in the mediator complex)
- RARA (retinoic acid receptor alpha)
...suggesting a shared pathogenesis with fibroadenoma. However, phyllodes tumors additionally acquire mutations in:
- TERT (telomerase gene) - associated with malignant progression
- TP53
- RB
Risk factors are generally unknown, though an association with Li-Fraumeni syndrome has been reported. Malignant phyllodes tumors are overrepresented in Li-Fraumeni kindreds.
Classification (WHO Grading)
Classified as benign, borderline, or malignant based on stromal histologic features:
| Feature | Benign | Borderline | Malignant |
|---|---|---|---|
| Stromal cellularity | Mild increase | Moderate | Marked |
| Stromal atypia | Mild | Moderate | Severe |
| Mitoses (per 10 HPF) | <5 | 5-9 | ≥10 |
| Tumor margin | Pushing | Pushing/focal infiltration | Infiltrative |
| Stromal overgrowth | Absent | May be present | Present |
| Tumor necrosis | Absent | Absent/rare | May be present |
Distribution: ~50% benign, ~25% borderline, ~25% malignant.
Morphology
Gross: Smooth, multinodular, well-demarcated, firm, mobile mass. Average size 4-7 cm; can grow massive (the entire breast). Larger lesions show characteristic bulbous leaf-like protrusions of stroma covered by epithelium extending into cystic spaces.
Histology:
- Benign: resemble fibroadenoma but with more cellular, mitotically active stroma
- Borderline: more prominent stromal atypia, cellularity, and mitotic activity
- Malignant: widely infiltrative, may be indistinguishable from sarcoma when there is marked stromal overgrowth with few residual epithelial elements
The key principle: the leaf-like pattern (phyllodes architecture) is the defining growth pattern - it is not itself a marker of malignancy.
Clinical Features
- Peak age: Sixth decade (10-20 years later than fibroadenoma)
- Presentation: Smooth, multinodular, painless, mobile mass - very similar to a fibroadenoma clinically; patients often report rapid enlargement of a previously stable nodule
- Size: 1-50 cm reported; average 4-7 cm
- Palpable axillary lymphadenopathy in up to 20% of patients, but true lymph node involvement is rare
- Bilateral lesions are rare
Diagnosis
| Modality | Findings |
|---|---|
| Mammography | Well-circumscribed mass; may show a halo; cannot reliably distinguish from fibroadenoma |
| Ultrasound | Smooth multilobulated hypoechoic mass resembling fibroadenoma; may show intramural cysts |
| Core needle biopsy (CNB) | Recommended; however, false-negative rate is 25-30% - histologic distinction between fibroadenoma and phyllodes tumor on CNB is very difficult |
Factors favoring excisional biopsy over observation: older age, new mass in a well-screened patient, rapid growth, size >2.5-3 cm, suspicious CNB, lobulated or cystic features on imaging.
A CNB reported as "cellular fibroepithelial lesion" should be excised for definitive diagnosis and local control - it could represent either a fibroadenoma or a phyllodes tumor.
Treatment
Surgery is the mainstay for all grades:
- Wide local excision with negative margins (1-2 cm) is standard
- Even large tumors can often be treated with breast-conserving surgery
- Mastectomy may be required for massive tumors or large tumors in small breasts - but should be avoided if possible
- Axillary lymph node dissection is contraindicated (lymphatic spread is rare regardless of grade; SLNB is not routinely performed)
- Re-excision is rarely needed for benign phyllodes, but is recommended for borderline and malignant forms if margins are positive
Adjuvant therapy:
- Adjuvant radiation and chemotherapy are controversial
- For large borderline or malignant tumors, they should be considered
- If systemic therapy is used for malignant phyllodes, guidelines for soft tissue sarcoma apply
Prognosis and Follow-Up
| Grade | Local Recurrence | Metastasis | Notes |
|---|---|---|---|
| Benign | ~10% | None | Margin status predicts recurrence |
| Borderline | Higher | Rare | Margin status key |
| Malignant | High | ~30-35% | Hematogenous; lung is most common site |
Key points:
- Only the neoplastic stromal component metastasizes (not the epithelial component)
- Metastases most commonly go to lungs - chest X-ray every 6 months for 2 years, then annually for malignant cases
- Once metastasis develops, mean overall survival is ~30 months
- Margin status is the most important predictor of local recurrence
- Mortality correlates with size and grade
vs. Fibroadenoma (Key Differences)
| Feature | Fibroadenoma | Phyllodes Tumor |
|---|---|---|
| Age | 20-35 years | 40-50s (sixth decade) |
| Size | Usually <3 cm | Often 4-7 cm, can be very large |
| Growth | Slow | Can be rapid |
| Stroma | Low cellularity | More cellular, mitotically active |
| Treatment | Observation acceptable | Excision always required |
| Mutations | MED12, RARA | MED12, RARA + TERT, TP53, RB |
Recent Evidence (2024-2026)
A recent meta-analysis (Torres et al., 2025) found Ki-67 is useful as a marker to differentiate borderline from benign phyllodes tumors - PMID 39721209. Another meta-analysis (Torres et al., 2026) examined comparative histological features of phyllodes tumor vs. fibroadenoma on core needle biopsies, reinforcing that CNB remains challenging for this distinction - PMID 41979873.
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease (block 11); Mulholland and Greenfield's Surgery: Scientific Principles and Practice, 7e (block 14); Berek & Novak's Gynecology (block 5); Current Surgical Therapy, 14e (block 8)
Fibroadenoma
Finding Sources
Searching PubMed
fibroadenoma breast
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have all the content needed. Here is the comprehensive answer.
Fibroadenoma
Overview
Fibroadenoma is the most common benign solid tumor of the female breast and the most common cause of a breast lump in women aged 15-25. It is a fibroepithelial tumor arising from intralobular stroma - a mixed neoplasm with both proliferating epithelial and stromal components.
Pathogenesis / Molecular Biology
Two-thirds of fibroadenomas carry driver mutations in MED12 - a gene encoding a subunit of the mediator complex, which regulates transcription of RNA polymerase II-dependent genes. Notably, uterine leiomyomas also arise from stromal cells and are strongly associated with MED12 mutations, suggesting a shared mechanism in hormone-responsive stromal tissues.
Additionally, ~one-third of fibroadenomas have mutations in RARA (retinoic acid receptor alpha), an estrogen target gene that cooperates with ER in regulating transcription. This molecular background explains the strong hormonal responsiveness of fibroadenomas.
Morphology
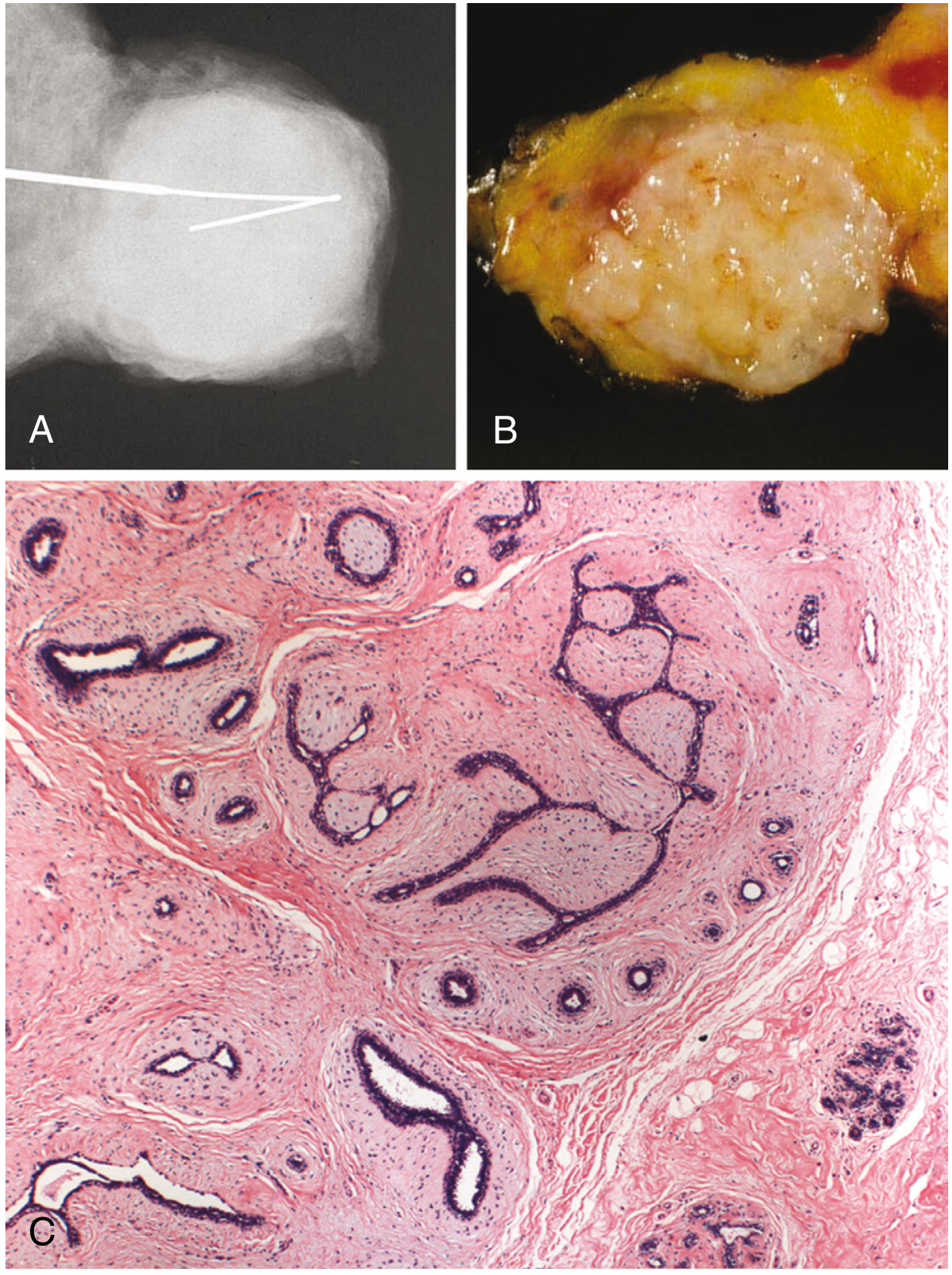
Fig. 23.24 from Robbins Pathologic Basis of Disease - (A) Mammographic appearance, (B) Gross specimen, (C) Histology showing both stromal and epithelial components
Gross:
- Well-circumscribed, encapsulated, rubbery, gray-white nodule
- Bulges above surrounding tissue on cut section
- Often contains slit-like spaces lined by epithelium
- Size: usually 1-3 cm; rarely giant (>5 cm)
Histology - two growth patterns:
- Pericanalicular pattern: delicate, myxoid stroma surrounds patent (open) ducts
- Intracanalicular pattern: stroma compresses and distorts ductal elements into cleft-like or slit-like spaces
In older women, the stroma becomes densely hyalinized and the epithelium atrophic. Calcifications may develop, appearing as "popcorn" calcifications on mammography.
Clinical Features
- Age: Most common in females in their 20s and 30s (15-25 years for first presentation); rarely after menopause
- Presentation: Firm, smooth, rubbery, freely mobile, non-tender mass - classically "breast mouse"
- Often bilobed; a groove can be palpated
- No skin dimpling, no nipple retraction, no inflammatory signs
- Size: Typically 1-3 cm when detected; rarely giant (>5 cm, especially at puberty)
- Multiplicity: Frequently multiple and bilateral
- Hormonal responsiveness:
- May enlarge during pregnancy (sometimes with infarction - can mimic carcinoma)
- Regress after menopause
- Multiple bilateral fibroadenomas seen in ~50% of women on cyclosporin A after renal transplantation (regress on stopping the drug)
Natural History
| Outcome | Frequency |
|---|---|
| Static / cease growth at 2-3 cm | Majority |
| Spontaneous regression | ~15% |
| Progressive growth | 5-10% |
Simple fibroadenoma is not associated with increased cancer risk. However, subtypes carry different risks:
| Subtype | RR for Breast Cancer |
|---|---|
| Simple fibroadenoma | 1.5-1.7× |
| Fibroadenoma with epithelial hyperplasia | 3.4-3.7× |
| Complex fibroadenoma + family history | 3.0-4.0× (especially lobular carcinoma) |
Subtypes
Myxoid fibroadenoma:
- Most are sporadic
- A small proportion are associated with Carney complex - an autosomal dominant condition caused by germline mutations in PRKAR1A
Complex fibroadenoma - defined by the presence of any of:
- Cysts >0.3 cm
- Sclerosing adenosis
- Epithelial calcifications
- Papillary apocrine change
Complex fibroadenomas are associated with slightly increased subsequent breast carcinoma risk, though this may be driven by "at-risk" lesions (e.g., atypical hyperplasia) in the surrounding breast tissue rather than the fibroadenoma itself.
Giant fibroadenoma: >5 cm; occasionally occurs during puberty; rapidly growing; can be enucleated via a submammary incision.
Diagnosis
| Modality | Findings |
|---|---|
| Mammogram | Well-circumscribed, smooth, oblong mass with clear margins; "popcorn" calcifications in older/involuted lesions |
| Ultrasound | Solid, uniformly hypoechoic, smoothly marginated, round or ovoid, wider than tall, no posterior shadowing |
| Core needle biopsy | Recommended if age >25, atypical features, or rapidly growing; classic imaging in a young woman may not require biopsy |
A classic fibroadenoma on imaging in a woman under 25 need not be biopsied but should have short-interval follow-up imaging to confirm stability.
Management
Conservative observation is appropriate for most:
- Serial imaging every 6-12 months to document stability
- ~15% regress spontaneously
Surgical excision is indicated when:
- Size >3-5 cm
- Rapid growth (>20% in 6 months)
- Age >30 years
- Suspicious features on imaging (microlobulation, etc.)
- Atypia on core biopsy
- Family history of breast cancer
- Patient anxiety or preference
- In elderly patients, excision should include a rim of normal tissue (to exclude malignancy or phyllodes tumor at the periphery)
Less invasive alternatives:
- Ultrasound-guided percutaneous vacuum-assisted biopsy
- Percutaneous cryoablation
- Regression with anti-estrogens (tamoxifen, ormeloxifene) has been observed
Key Differentials
| Feature | Fibroadenoma | Phyllodes Tumor | Breast Cyst |
|---|---|---|---|
| Age | 15-35 | 40-50s | 30-50s |
| Consistency | Rubbery, firm | Firm, multinodular | Tense, fluctuant |
| Mobility | Highly mobile | Mobile | Mobile |
| Growth | Slow | May be rapid | Varies |
| Ultrasound | Solid, hypoechoic | Solid, multilobulated ± internal cysts | Anechoic, posterior enhancement |
| Treatment | Observation often OK | Always excise | Aspiration if symptomatic |
Recent Evidence (2024-2026)
A recent systematic review (Math et al., 2026, PMID 41919577) specifically examined the clinical characteristics and management of multiple fibroadenomas, providing updated guidance on this subgroup. A comparative histological meta-analysis (Torres et al., 2026, PMID 41979873) highlights that distinguishing fibroadenoma from phyllodes tumor on core needle biopsy remains histologically challenging.
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease (block 11); Bailey and Love's Short Practice of Surgery, 28e (block 8); Current Surgical Therapy, 14e (block 8); Berek & Novak's Gynecology (block 5)
Difference between phyllodes tumor and fibroadenoma.
Based on the detailed content already retrieved in this session from multiple authoritative textbooks, here is a comprehensive comparison:
Phyllodes Tumor vs. Fibroadenoma
Both are fibroepithelial tumors arising from intralobular stroma of the breast, and both share mutations in MED12 and RARA - suggesting a shared pathogenesis. Despite this, they differ significantly in behavior, histology, and management.
Side-by-Side Comparison
| Feature | Fibroadenoma | Phyllodes Tumor |
|---|---|---|
| Incidence | Most common benign breast tumor | Rare; ~2.5% of fibroepithelial lesions; <0.5% of all breast tumors |
| Age at presentation | 15-35 years (peak 20s-30s) | 40-50s; sixth decade (10-20 years later than fibroadenoma) |
| Growth rate | Slow; most stabilize at 2-3 cm | Can grow rapidly; average size 4-7 cm; may become massive |
| Bilaterality | Frequently multiple and bilateral | Rarely bilateral; usually isolated |
| Surface / consistency | Rubbery, firm, smooth | Smooth, multinodular, bosselated surface |
| Mobility | Highly mobile ("breast mouse") | Mobile, rarely infiltrates skin until late |
| Pain / skin changes | Painless; no skin changes | Painless; overlying skin may ulcerate from pressure necrosis in very large lesions |
| Hormonal responsiveness | Yes - enlarges in pregnancy, regresses post-menopause | Less prominent |
| Capsule | Well-encapsulated | Well-demarcated but may be infiltrative (malignant type) |
| Mutations | MED12, RARA | MED12, RARA + TERT, TP53, RB (additional mutations drive malignant progression) |
Histological Differences
| Histological Feature | Fibroadenoma | Phyllodes Tumor |
|---|---|---|
| Stroma | Delicate, myxoid, low cellularity | Hypercellular, mitotically active |
| Growth patterns | Pericanalicular or intracanalicular | Leaf-like (phyllodes) stromal projections covered by epithelium |
| Stromal atypia | Absent | Present (increases with grade) |
| Mitotic rate | Very low | Varies by grade (see below) |
| Stromal overgrowth | Absent | Present in malignant forms |
| Tumor margins | Sharply delimited, pushing | Pushing (benign) → infiltrative (malignant) |
| Metastatic component | N/A | Only the stromal component metastasizes (not epithelium) |
Phyllodes Grading by Histology
| Grade | Mitoses (per 10 HPF) | Stroma | Margins |
|---|---|---|---|
| Benign | <4-5 | Mildly cellular | Pushing |
| Borderline | 5-9 | Moderately cellular, moderate atypia | Pushing ± focal infiltration |
| Malignant | ≥10 | Markedly cellular, severe atypia, overgrowth | Infiltrative |
Imaging Differences
| Modality | Fibroadenoma | Phyllodes Tumor |
|---|---|---|
| Mammogram | Well-circumscribed, smooth, oblong mass; "popcorn" calcifications in older lesions | Well-circumscribed mass; may show a halo; cannot reliably be distinguished from fibroadenoma |
| Ultrasound | Solid, uniformly hypoechoic, wider than tall, no posterior shadowing | Smooth multilobulated mass; may show intramural cysts (a distinguishing clue) |
| Core biopsy | Often diagnostic | False-negative rate 25-30%; reported as "cellular fibroepithelial lesion" when distinction is uncertain |
The key imaging clue favoring phyllodes over fibroadenoma: older patient + larger size + lobulated mass + internal cysts on ultrasound + rapid growth history.
Natural History and Cancer Risk
| Fibroadenoma | Phyllodes Tumor | |
|---|---|---|
| Cancer risk | Simple: 1.5-1.7× RR; Complex + FHx: 3-4× | Malignant form: ~30-35% develop distant metastases |
| Local recurrence | Rare after excision | Up to 10% (benign); higher for borderline/malignant |
| Metastasis | None | Hematogenous (lung most common) in malignant type; lymphatic spread is rare for ALL grades |
| Spontaneous regression | ~15% | Does not regress |
Management Differences
| Decision | Fibroadenoma | Phyllodes Tumor |
|---|---|---|
| Observation | Acceptable for classic lesions <3 cm in young women | Never - all phyllodes tumors require excision |
| Surgical excision | Indicated for size >3-5 cm, rapid growth, atypia, age >30, patient preference | Always - wide local excision with 1-2 cm clear margins |
| Margin requirement | Simple excision sufficient | Negative margins mandatory; re-excision recommended for borderline/malignant if margins involved |
| Mastectomy | Not needed | Reserved for massive tumors or large tumors in small breasts |
| Axillary surgery | Not indicated | Contraindicated (SLNB not routinely performed; ALND contraindicated) |
| Adjuvant therapy | Not applicable | Considered for large borderline/malignant tumors; chemotherapy follows sarcoma guidelines |
| Follow-up | Serial imaging to confirm stability | Chest X-ray every 6 months × 2 years, then annually (malignant type) |
The Clinical Dilemma
The single most important practical point: fibroadenoma and phyllodes tumor are clinically and radiologically indistinguishable in many cases. Even core needle biopsy has a 25-30% false-negative rate for phyllodes. The distinction hinges on:
- Age - phyllodes more likely in a woman >35-40
- Rapid growth - a history of sudden enlargement of a "stable" nodule strongly favors phyllodes
- Size - >2.5-3 cm in a well-screened patient raises suspicion
- CNB result - a "cellular fibroepithelial lesion" on CNB should be excised regardless
When in doubt, excise - because observing an undiagnosed phyllodes tumor risks local recurrence and, in malignant cases, metastatic spread.
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease; Mulholland and Greenfield's Surgery, 7e; Berek & Novak's Gynecology; Current Surgical Therapy, 14e; Bailey and Love's Short Practice of Surgery, 28e
This is a shared conversation. Sign in to Orris to start your own chat.