Anterior midline swelling of neck
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
I now have comprehensive information from multiple authoritative sources. Let me compile the full answer.
Anterior Midline Swelling of the Neck
Midline neck swellings are best understood by their anatomical level - from above downwards - and by their key clinical features (movement with swallowing, movement with tongue protrusion, transillumination, etc.).
Classification: From Above Downwards
(S. Das - Manual on Clinical Surgery)
| Level | Swelling |
|---|---|
| Submental/Suprahyoid | Ludwig's angina, enlarged submental lymph nodes, sublingual dermoid, lipoma |
| Hyoid region | Thyroglossal cyst, subhyoid bursitis |
| Below hyoid | Goitre (thyroid isthmus/pyramidal lobe), enlarged lymph nodes, lipoma |
| Suprasternal/retrosternal | Retrosternal goitre, thymic swelling |
| Anywhere in midline | Dermoid cyst |
Key Differentials in Detail
1. Thyroglossal Duct Cyst (Most Important)
The most common congenital cystic mass in the neck and the second most common benign neck mass after benign lymphadenopathy.
Embryology: The thyroid gland descends from the foramen caecum at the base of the tongue to the lower anterior neck via the thyroglossal duct, which normally involutes by the 8th-10th week of gestation. If any portion persists, secretions from the epithelial lining produce a cyst.
Distribution of location:
- 65% below the hyoid bone
- 15% at the level of the hyoid bone
- 75% are in the midline; up to 2 cm off-midline is possible
Clinical features:
- Painless midline neck mass, mostly in children
- Moves upward on swallowing AND on tongue protrusion - this is the hallmark sign
- May become infected (pain, redness, swelling) and rupture, forming a discharging sinus
- Rarely causes dysphagia or dyspnoea
- 1% risk of malignancy (classically papillary thyroid carcinoma)
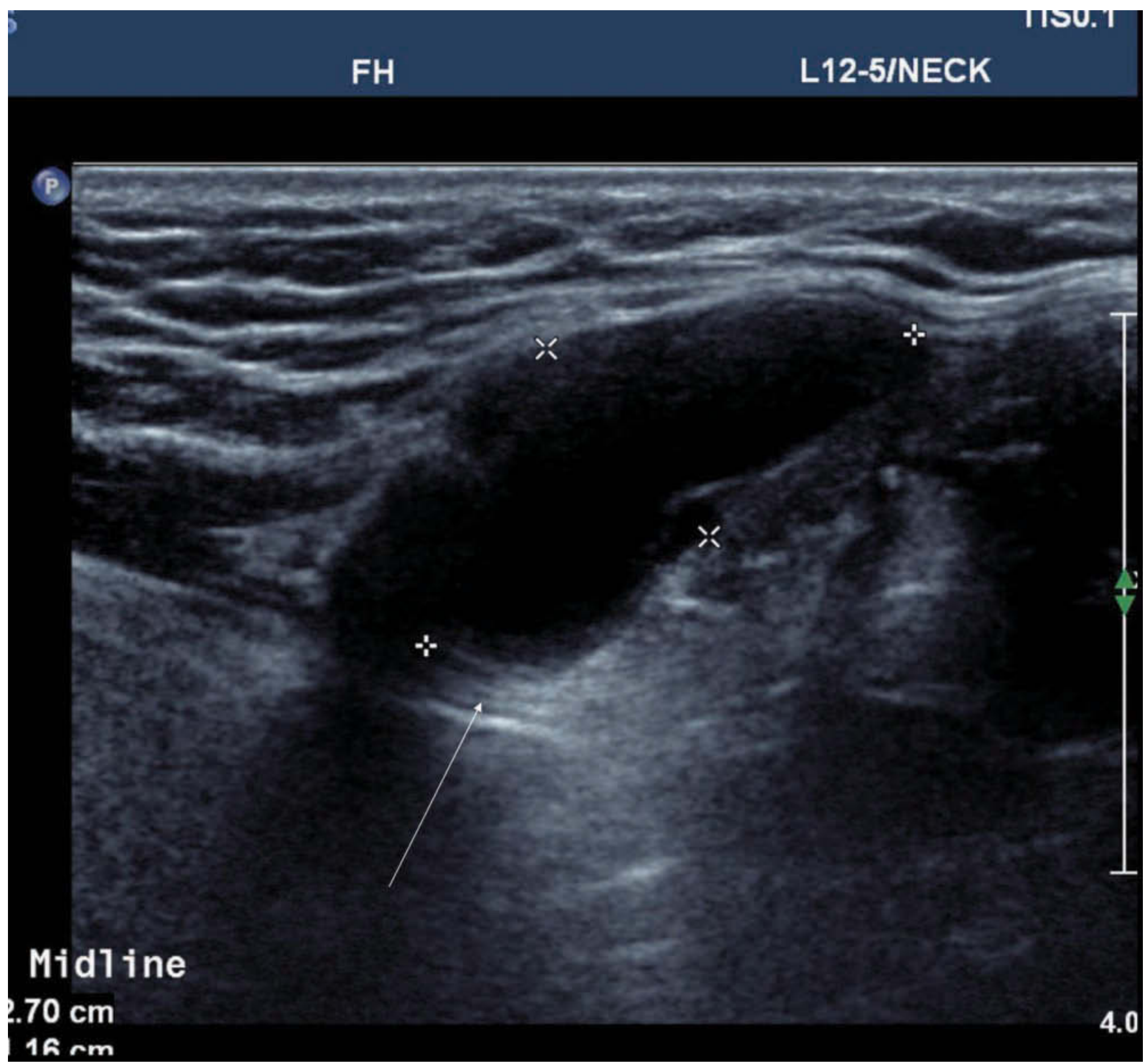
Imaging:
- Ultrasound: homogeneous anechoic cystic mass with posterior wall enhancement (see image below), or pseudosolid if infected/hemorrhagic
- CT/MRI: invariably high T2 signal; variable T1 depending on protein content
- Must confirm presence of normal thyroid tissue in the normal location (rare cases represent the only functioning thyroid tissue)
Treatment: Sistrunk's Operation
- Excision of the cyst + central body of the hyoid bone + the entire suprathyoid tract through to the tongue base (foramen caecum)
- Removal of the hyoid body is essential because the duct is intimately related to it; failure to do so causes recurrence
- Complete excision minimizes recurrence from small side branches of the tract
2. Goitre (Thyroid Swelling)
- Moves up on swallowing but does NOT move on tongue protrusion
- Can involve the isthmus or pyramidal lobe presenting as a midline mass
- May extend retrosternally (retrosternal goitre)
- Confirmed on ultrasound; thyroid function tests and FNAC required
3. Dermoid Cyst
- Can occur anywhere in the midline
- Sublingual dermoid: in the submental region above the hyoid
- Does NOT move with swallowing or tongue protrusion
- Doughy consistency, may contain hair/teeth/sebum
- Does not transilluminate (cf. cystic hygroma)
4. Subhyoid Bursitis
- Located at the level of the hyoid bone
- Moves on swallowing
- Can mimic a thyroglossal cyst clinically
5. Ludwig's Angina
- Acute, life-threatening bilateral cellulitis of the floor of mouth and submental space
- Tender, boardlike swelling in the submental region
- Associated with dental infection (usually lower 2nd/3rd molars)
- Elevation of tongue, drooling, risk of airway compromise
6. Submental Lymph Nodes
- Enlarged lymph nodes in the submental triangle
- Reactive (dental/lip/tongue infection) or malignant (floor of mouth Ca)
- Multiple, discrete or matted
- Do not move with swallowing or tongue protrusion
7. Cystic Hygroma (Lymphatic Malformation)
- Congenital lymphatic malformation; presents at birth or in infancy
- Soft, compressible, brilliantly transilluminant (pathognomonic)
- Increases in size on crying/coughing
- Often bilateral, may extend to face/tongue/floor of mouth
- Management: complete excision or sclerotherapy (OK-432, bleomycin)
Diagnostic Approach Summary
| Feature | Thyroglossal cyst | Goitre | Dermoid | Cystic hygroma |
|---|---|---|---|---|
| Moves with swallowing | Yes | Yes | No | No |
| Moves with tongue protrusion | Yes | No | No | No |
| Transilluminates | No | No | No | Yes |
| Age | Children (any age) | Any | Any | Infancy/birth |
| Consistency | Cystic | Firm/rubbery | Doughy | Soft/compressible |
Sources
- Sabiston Textbook of Surgery, Chapter on Thyroglossal Duct Cyst
- Bailey and Love's Short Practice of Surgery, 28th Ed., Thyroglossal Duct Cysts
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, TDC and neck swelling imaging
- S. Das - Manual on Clinical Surgery, 13th Ed., Differential Diagnosis of Neck Swellings
This is a shared conversation. Sign in to Orris to start your own chat.