Blood supply to stomach
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Excellent - I have a clear anatomical diagram and rich textbook content. Here is the full answer:
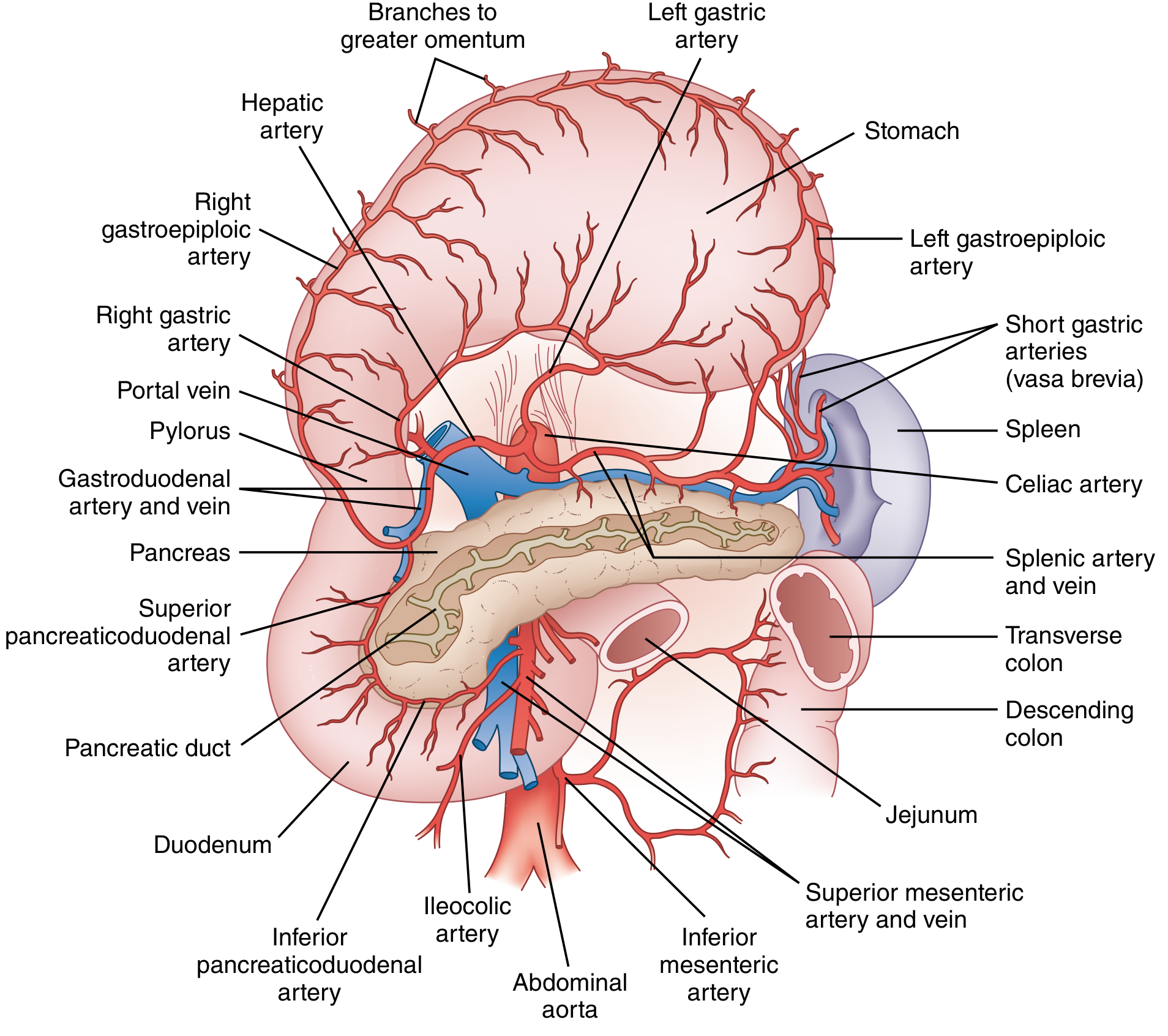
Blood Supply to the Stomach
The stomach is the most richly vascularized segment of the alimentary tract, with a dense intramural anastomotic network. Nearly all of its blood comes from branches of the celiac axis (celiac trunk), the first unpaired branch of the abdominal aorta.
Arterial Supply
1. Lesser Curvature Arcade
| Artery | Origin | Course |
|---|---|---|
| Left gastric artery | Directly from celiac trunk | Runs right along lesser curvature; largest artery to the stomach |
| Right gastric artery | Proper hepatic artery (near pylorus) | Runs left along lesser curvature; anastomoses with left gastric |
These two vessels form a continuous anastomotic arcade along the lesser curvature.
- The left gastric is the largest gastric artery. In ~20% of people it gives off an aberrant left hepatic artery that travels in the gastrohepatic ligament - inadvertent ligation can cause hepatic ischemia.
- In 90% of individuals the left gastric arises from the celiac axis; rarely it may arise from the common hepatic artery, splenic artery, or directly from the aorta.
2. Greater Curvature Arcade
| Artery | Origin | Course |
|---|---|---|
| Right gastroepiploic artery | Gastroduodenal artery (behind 1st part of duodenum) | Runs left along greater curvature |
| Left gastroepiploic artery | Splenic artery | Runs right along greater curvature; anastomoses with right gastroepiploic |
These form the gastroepiploic arcade along the greater curvature.
3. Fundus and Proximal Greater Curvature
- Short gastric arteries (vasa brevia) - 4 to 6 branches from the splenic artery; travel in the gastrosplenic (gastrolienal) ligament to supply the fundus and proximal greater curvature.
- Inferior phrenic artery - may contribute small branches to the proximal/fundic stomach.
Venous Drainage
Veins of the stomach generally parallel the arteries and all drain ultimately into the portal venous system.
| Vein | Drains Into |
|---|---|
| Left gastric vein (coronary vein) | Portal vein |
| Right gastric vein | Portal vein |
| Right gastroepiploic vein | Superior mesenteric vein (forms part of Henle's trunk with right colic and anterior superior pancreaticoduodenal veins) |
| Left gastroepiploic vein | Splenic vein |
| Short gastric veins | Splenic vein |
Clinical point - portal hypertension: Retrograde flow through the left gastric (coronary) vein leads to gastroesophageal varices. In splenic vein thrombosis (from pancreatitis or pancreatic tumour), isolated gastric varices form via the gastroepiploic channels - this is treated by splenectomy alone.
Microvascular Anatomy
- Large arteries branch into submucosal arterioles
- ~70-80% of gastric blood flow goes to the mucosal capillary beds surrounding gastric glands
- ~20-30% supplies the muscle layers
- Mucosal capillaries drain into submucosal venous plexuses
- The "alkaline tide" - bicarbonate generated during acid secretion is secreted into capillaries and recycled to buffer surface mucosa
Clinical Significance
-
Remarkable resilience to ischemia: Because of rich anastomoses, the stomach survives ligation of 3 of 4 named arteries, provided the arcades are intact. This is exploited during esophagectomy (stomach pedicled on right gastric + right gastroepiploic) and sleeve gastrectomy.
-
Gastric variceal bleeding: Isolated fundal varices strongly suggest splenic vein thrombosis - splenectomy is curative.
-
Peptic ulcer bleeding: Posterior duodenal ulcers erode the gastroduodenal artery; posterior gastric ulcers can erode the splenic artery - both are surgical emergencies.
-
Gastric conduit for esophageal replacement: The stomach is pedicled on the right gastroepiploic artery (the second largest gastric vessel), with the left gastric, short gastric, and left gastroepiploic vessels all divided.
Sources: Yamada's Textbook of Gastroenterology, 7th ed. | Sabiston Textbook of Surgery, 21st ed. | Schwartz's Principles of Surgery, 11th ed.
This is a shared conversation. Sign in to Orris to start your own chat.