Osteoarthritis
Reading File
Finding Sources
Searching PubMed
"osteoarthritis"[MeSH Terms] AND "treatment"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Searching PubMed
osteoarthritis management
Loading Image
Loading Image
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive data from multiple authoritative textbooks. Let me compile the full answer.
Osteoarthritis (OA)
Definition
Osteoarthritis is characterized by failed repair of synovial joint tissues after intra-articular stress. The resulting breakdown of cartilage and bone leads to pain, stiffness, and functional disability. It is primarily a degenerative disorder of articular cartilage, with inflammation acting as a secondary contributor rather than the primary driver.
- Goldman-Cecil Medicine, p. 2766
- Robbins & Kumar Basic Pathology, p. 790
Epidemiology
- Most common disease of joints; affects >500 million people worldwide
- Women are disproportionately affected
- Prevalence increases exponentially after age 50; ~40% of people over 70 are affected
- Lifetime risk of symptomatic knee OA: ~40% in men, ~47% in women, rising to 60% in those with excess weight
- Globally, OA cases rose 48% from 1990 to 2019; it is now the 15th highest cause of years lived with disability worldwide
- Goldman-Cecil Medicine, p. 2766
Classification
| Type | Description |
|---|---|
| Primary (Idiopathic) | Appears insidiously as an aging phenomenon; oligoarticular, affecting a few weight-bearing joints |
| Secondary | ~5% of cases; occurs in younger individuals with predisposing conditions - joint deformity, prior injury, diabetes, obesity |
- Robbins Basic Pathology, p. 790
Pathogenesis
Biomechanical stress is the principal pathogenic mechanism. Genetic factors, including polymorphisms in genes such as GDF5, RUNX2, SMAD3, and PTHLH (involved in skeletal and bone development), also contribute to susceptibility.
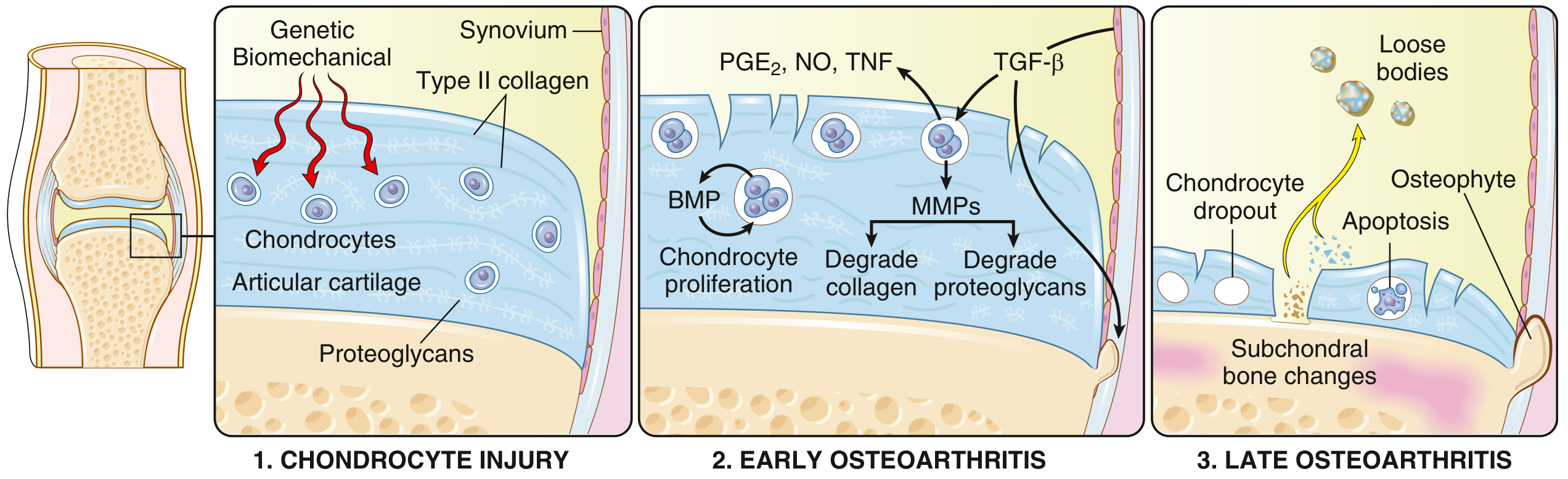
The disease process unfolds in three stages:
-
Chondrocyte Injury - Biomechanical and genetic insults damage chondrocytes; initial proteoglycan loss causes articular cartilage to swell and become susceptible to physical disruption
-
Early OA - Chondrocytes proliferate and attempt repair, but release matrix metalloproteinases (MMPs) that degrade collagen and proteoglycans. Inflammatory mediators - PGE2, nitric oxide, TNF - exacerbate damage; TGF-β attempts repair but cannot compensate
-
Late OA - Chondrocyte dropout via apoptosis; full-thickness cartilage sloughing exposes subchondral bone; osteophyte formation at joint margins; loose bodies ("joint mice") form in the joint space; subchondral bone remodeling and cyst formation
- Robbins Basic Pathology, p. 790-791; Goldman-Cecil Medicine, p. 2767
Morphology
Key pathological findings:
- Fibrillation of articular cartilage (early - surface irregularities)
- Bone eburnation - polished ivory appearance of exposed subchondral bone
- Subchondral cysts - synovial fluid forced into bone via a ball-valve mechanism through small fractures
- Osteophytes - bony outgrowths at joint margins, capped by fibrocartilage/hyaline cartilage that ossifies
- Loose bodies (joint mice) - dislodged cartilage/bone fragments in the joint
- Mild synovitis - only modest synovial congestion and fibrosis with scattered chronic inflammatory cells (unlike RA)
The synovial fluid in OA is non-inflammatory with fewer than 2,000 leucocytes/μL; basic calcium phosphate crystals are often present.
- Robbins Basic Pathology, p. 790-791; Goldman-Cecil Medicine, p. 2770
OA vs. Rheumatoid Arthritis - Key Differences
| Feature | Osteoarthritis | Rheumatoid Arthritis |
|---|---|---|
| Primary pathology | Mechanical injury to articular cartilage | Autoimmunity |
| Inflammation | Secondary; exacerbates damage | Primary cause of cartilage destruction |
| Joints | Weight-bearing (knees, hips) | Small joints of fingers first; then multiple joints |
| Pathology | Cartilage degeneration, osteophytes, subchondral cysts; minimal inflammation | Inflammatory pannus invading cartilage; joint fusion (ankylosis) |
| Serum antibodies | None | ACPA, rheumatoid factor |
| Extra-articular disease | No | Yes (lungs, heart, other organs) |
- Robbins Basic Pathology, p. 790 (Table 19.2)
Clinical Features
Symptoms:
- Joint pain that worsens with use (mechanical pattern)
- Brief morning stiffness (typically <30 minutes - distinguishes OA from RA, where stiffness is prolonged)
- Crepitus on movement
- Limitation of range of motion
- Spinal involvement: osteophytes impinging on foramina cause cervical/lumbar nerve root compression, radicular pain, muscle spasms, neurologic deficits
Signs on examination:
- Joint line tenderness
- Bony swelling (osteophytes) and soft tissue swelling (effusion)
- Crepitus (especially under patella)
- Loss of range of motion
- Deformity (varus/valgus in knee), muscle weakness and atrophy in advanced disease
- Hip OA: early restriction of internal rotation with end-range pain
Joints commonly involved:
- Hips, knees
- Lower lumbar and cervical vertebrae
- Proximal and distal interphalangeal joints of the fingers
- First carpometacarpal joints
- First tarsometatarsal joints
Heberden nodes = osteophytes at the distal interphalangeal joints (more common in women)
Bouchard nodes = osteophytes at the proximal interphalangeal joints
Important note: The level of disease severity on radiographs does not correlate well with pain and disability.
- Robbins Basic Pathology, p. 791; Goldman-Cecil Medicine, p. 2768-2769
Diagnosis
Diagnosis is clinical, based on:
- Symptoms: pain, brief morning stiffness, functional limitation
- Examination: crepitus, restricted/painful movement, joint tenderness, bony enlargement
Plain radiographs are not required for a typical presentation but can be used for:
- Atypical presentations
- Diagnostic uncertainty
- Pre-operative planning
X-ray findings in OA:
- Joint space narrowing (cartilage loss)
- Subchondral sclerosis
- Subchondral cysts
- Osteophytes at joint margins
Lab tests are not needed for routine diagnosis. They may help exclude coexistent inflammatory disease:
- RF, CRP, ESR to exclude RA
- Synovial fluid crystal analysis to exclude gout/CPPD
Synovial fluid: Non-inflammatory (<2,000 WBC/μL); basic calcium phosphate crystals often present
- Goldman-Cecil Medicine, p. 2769-2770
Clinical Phenotypes (Goldman-Cecil)
Modern understanding recognizes several OA phenotypes:
- Chronic pain phenotype - central sensitization predominates
- Inflammatory phenotype - prominent synovitis, effusion
- Metabolic syndrome phenotype - obesity, diabetes, dyslipidemia-driven
- Bone and cartilage metabolism phenotype - genetic/structural drivers
- Mechanical overload phenotype - injury, malalignment-related
- Minimal joint disease phenotype - symptoms disproportionate to structural damage
Management
Management should be individually tailored, focusing on core treatments first.
Non-pharmacologic (First-line / Core Treatments)
| Intervention | Evidence Level (AAOS) |
|---|---|
| Patient education programs | Strong - Recommended |
| Exercise (supervised, unsupervised, aquatic) | Strong - Recommended |
| Self-management programs | Strong - Recommended |
| Sustained weight loss (target BMI <25; start with 5-10% loss) | Moderate - Recommended |
| Canes | Moderate - Recommended |
| Brace treatment | Moderate - Recommended |
| Neuromuscular training + exercise | Moderate - Recommended |
| Lateral wedge insoles | Not Recommended |
A 2025 BMJ network meta-analysis (PMID: 41093618) compared exercise modalities in knee OA, providing updated evidence on optimal exercise types.
Pharmacologic
| Drug | Notes |
|---|---|
| Topical NSAIDs | Preferred over oral NSAIDs (safer, recommended first-line especially in knee OA) |
| Oral NSAIDs | First-line systemic analgesic; use lowest effective dose |
| Oral acetaminophen | Recommended for mild-moderate pain |
| Intra-articular corticosteroids | Short-term pain relief; moderate evidence |
| Oral narcotics / tramadol | Not Recommended (AAOS) |
| Hyaluronic acid injections | Not Recommended (AAOS) |
- Goldman-Cecil Medicine: "NSAIDs are usually advocated as first-line therapy" for analgesics, but topical and OTC options are preferred over systemic treatments owing to safety concerns
- Miller's Review of Orthopaedics, p. 468 (AAOS Evidence-Based CPG)
Interventional / Surgical
| Procedure | Evidence |
|---|---|
| Joint replacement | For severe disease where functional status interferes with daily living and conservative treatment fails |
| Arthroscopic partial meniscectomy | Recommended for meniscal tears with concomitant mild-moderate OA |
| Arthroscopy with lavage/debridement | Not Recommended |
Therapies with Limited Evidence (May be considered selectively)
Platelet-rich plasma, acupuncture, TENS, extracorporeal shockwave therapy, glucosamine/chondroitin supplements, high tibial osteotomy (in properly selected unicompartmental cases)
Prognosis
- No treatments currently prevent or halt OA progression - management is symptom-focused
- 80% of affected individuals suffer limitations in movement; 25% have difficulty with major activities of daily living
- Joint fusion (ankylosis) does not occur in OA (unlike RA)
- Radiographic severity poorly predicts functional outcomes
Sources:
- Robbins & Kumar Basic Pathology, pp. 790-791
- Goldman-Cecil Medicine, Chapter 241 (Hunter DJ), pp. 2765-2772
- Miller's Review of Orthopaedics 9th Ed., p. 468 (AAOS Guideline Table 5.7)
- Recent evidence: Comparative efficacy of exercise modalities in knee OA - BMJ 2025 (Network Meta-Analysis, PMID 41093618)
This is a shared conversation. Sign in to Orris to start your own chat.