Ulnar nerve special tests
Reading File
Finding Sources
Finding Sources
Searching the Web
ulnar nerve special tests clinical examination Froment Wartenberg elbow flexion test
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive overview of the special tests used to assess the ulnar nerve, organized by test type and clinical purpose.
Ulnar Nerve Special Tests
Overview of Relevant Anatomy
The ulnar nerve is most commonly compressed at two sites:
- Cubital tunnel (at the elbow) - most common
- Guyon's canal (at the wrist)
The autonomous sensory zone of the ulnar nerve is the middle and distal phalanges of the little finger - complete anesthesia here strongly suggests total nerve division. - Campbell's Operative Orthopaedics 15th Ed 2026
1. Tinel's Sign (Percussion Test)
Purpose: Detect ulnar nerve irritation or compression at the elbow or wrist
Technique: Gently tap with two fingers over anatomic sites of compression - the cubital tunnel (posterior to medial epicondyle), or Guyon's canal at the wrist.
Positive finding: Reproduction of numbness, tingling, or pain in the ulnar nerve distribution (ring and little fingers, medial palm)
Clinical significance: A positive percussion test over the ulnar nerve at the medial epicondyle, combined with a positive elbow flexion test, strongly suggests a significant compressive neuropathy. - Campbell's Operative Orthopaedics 15th Ed 2026, p. 3871
2. Elbow Flexion Test (Hyperflexion Test)
Purpose: Detect cubital tunnel syndrome
Technique: Ask the patient to fully flex the elbow (maximally) with the shoulder flexed at ~90 degrees. Hold the position for up to 3 minutes (often positive within 1 minute). Adding wrist flexion in an ulnar direction further aggravates symptoms by contracting the FCU.
Positive finding: Reproduction of numbness, tingling, or paresthesia in the ring and little fingers (ulnar distribution) within 1-3 minutes.
Mechanism: Full elbow flexion draws the aponeurosis of the two heads of flexor carpi ulnaris (which forms the cubital tunnel roof) taut over the nerve, increasing pressure and compressing it. - Tintinalli's Emergency Medicine; Campbell's Operative Orthopaedics
3. Froment's Sign
Purpose: Assess ulnar neuropathy - specifically adductor pollicis weakness
Technique: Ask the patient to pinch/grasp a sheet of paper (or flat object) between the thumb and lateral border of the index finger using a key pinch.
Positive finding: The patient flexes the thumb at the interphalangeal (IP) joint to substitute the weakened adductor pollicis (ulnar-innervated) with the flexor pollicis longus (FPL - median-innervated). This is the classic compensatory maneuver.
Why it works: A normal adductor pollicis holds the paper with the thumb in extension. When it is weak, FPL takes over and the IP joint flexes noticeably. - Harrison's Principles of Internal Medicine 22E; Bailey and Love's 28th Ed
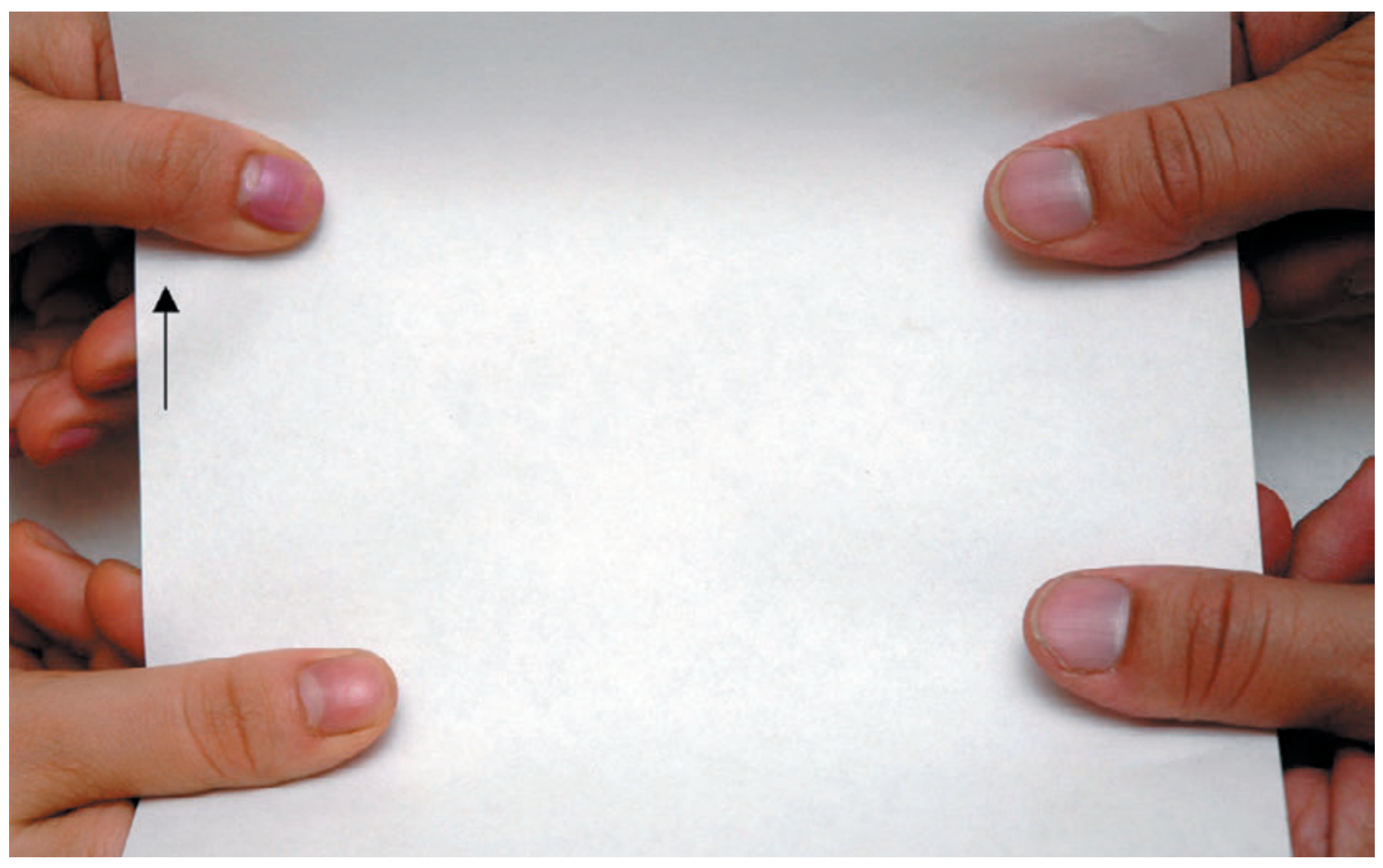
Froment's sign: arrow shows the flexed thumb IP joint (positive test) - Bailey and Love's Short Practice of Surgery 28th Ed
4. Jeanne's Sign
Purpose: Further confirm adductor pollicis weakness (ulnar nerve)
Technique: Observe the thumb during the same key pinch maneuver as Froment's sign.
Positive finding: Hyperextension of the thumb MCP joint during key pinch, due to a weak adductor pollicis muscle (unable to stabilize the MCP joint during pinch). - Miller's Review of Orthopaedics 9th Ed
Note: Froment and Jeanne's signs often occur together in the same patient.
5. Wartenberg's Sign
Purpose: Assess ulnar neuropathy - intrinsic muscle weakness (3rd palmar interosseous)
Technique: Ask the patient to hold their fingers together (adduct the little finger).
Positive finding: The little finger remains in abduction and extension, because the weak 3rd volar interosseous (ulnar nerve) cannot resist the unopposed pull of extensor digiti quinti (radial nerve). - Miller's Review of Orthopaedics 9th Ed; Sabiston Textbook of Surgery
Also note: Wartenberg's sign is distinguished from Wartenberg's syndrome, which is compressive neuropathy of the superficial radial nerve (cheiralgia paresthetica - an entirely different condition).
6. Scratch Collapse Test
Purpose: Identify the site of ulnar nerve compression (cubital tunnel)
Technique (Mackinnon): The examiner lightly scratches the patient's skin over the suspected area of compression while the patient performs resisted bilateral shoulder external rotation.
Positive finding: A brief, transient loss of muscle resistance (collapse of external rotation) is elicited, indicating allodynia from the underlying compression neuropathy. - Campbell's Operative Orthopaedics 15th Ed 2026
7. Shoulder Internal Rotation Test
Purpose: Provocative test for cubital tunnel syndrome (described by Ochi et al.)
Technique: Position the shoulder at 90° abduction with maximal internal rotation, elbow at 90° flexion, wrist neutral, and fingers fully extended.
Positive finding: Reproduction of ulnar symptoms in the hand/ring-little fingers.
Sensitivity: Reported to be more sensitive than the elbow flexion test, with 80% of subjects having symptoms within 10 seconds. - Campbell's Operative Orthopaedics 15th Ed 2026
8. Finger Abduction/Adduction Test (Interosseous Muscle Testing)
Purpose: Assess dorsal and palmar interossei (ulnar nerve)
Technique:
- Have the patient spread (abduct) fingers against resistance - tests dorsal interossei
- Have the patient crisscross fingers - tests palmar interossei
Positive finding: Weakness in either task indicates ulnar nerve dysfunction. - Sabiston Textbook of Surgery
Quick Reference Summary Table
| Test | Structure Tested | Positive Finding | Level Suggested |
|---|---|---|---|
| Tinel's sign | Nerve irritability | Tingling in ulnar distribution | Elbow or wrist |
| Elbow Flexion Test | Cubital tunnel compression | Paresthesia in ring/little fingers | Elbow (cubital tunnel) |
| Froment's sign | Adductor pollicis (motor) | Thumb IP flexion during key pinch | Distal ulnar |
| Jeanne's sign | Adductor pollicis (motor) | Thumb MCP hyperextension during pinch | Distal ulnar |
| Wartenberg's sign | 3rd palmar interosseous (motor) | Little finger abduction/extension | Distal ulnar |
| Scratch Collapse Test | Site of allodynia | Transient loss of ER resistance | Elbow (cubital tunnel) |
| Shoulder Internal Rotation Test | Cubital tunnel compression | Symptoms within 10 sec | Elbow (cubital tunnel) |
| Interosseous testing | Dorsal/palmar interossei | Weakness of abduction/adduction | Distal ulnar |
Key clinical point: In suspected cubital tunnel syndrome, a positive Tinel's sign at the medial epicondyle combined with a positive Elbow Flexion Test strongly supports a compressive neuropathy. Nerve conduction studies should show slowing of ulnar motor NCV across the elbow, though early involvement may show normal velocities. - Campbell's Operative Orthopaedics 15th Ed 2026
Egawa test Card test
Finding Sources
Searching the Web
Egawa test ulnar nerve middle finger interosseous clinical examination
Searching the Web
card test ulnar nerve palmar interosseous finger adduction clinical test
Reading File
Reading Web Page
https://orthofixar.com/special-test/egawa-sign-test
Loading Image
Here is a focused breakdown of both tests:
Egawa Test & Card Test - Ulnar Nerve
Both tests assess the interosseous muscles, which are entirely supplied by the deep branch of the ulnar nerve. They complement each other - one tests the dorsal interossei (abductors), the other the palmar interossei (adductors).
Egawa Test (Egawa Sign)
Purpose: Tests the dorsal interossei - specifically the ability of the middle (3rd) finger to abduct/adduct
Why the middle finger? The middle finger is the only finger where both radial and ulnar deviation (abduction in both directions) are produced by dorsal interossei (1st and 2nd dorsal interosseous on either side). It has no palmar interosseous, making it a pure dorsal interosseous test.
Technique:
- The patient places their hand flat on a table, palm facing down
- The patient is asked to move the middle finger sideways (alternating radial and ulnar deviation - i.e., abducting left and right)
Positive finding: Inability or marked weakness to deviate the middle finger sideways - indicates dorsal interosseous (ulnar nerve) dysfunction
Clinical significance:
- The interossei are among the first muscles affected in ulnar nerve compression, making this test useful for early detection
- Helps localize the lesion to the deep branch of the ulnar nerve
- Can be used serially to monitor progression or recovery
- A positive Egawa sign is typically accompanied by Froment's sign and Wartenberg's sign in established ulnar palsy
Card Test
Purpose: Tests the palmar interossei - the finger adductors
Technique:
- The examiner inserts a card (or piece of paper) between two adjacent extended fingers
- The patient is asked to hold the card as tightly as possible by adducting the fingers
- The examiner then tries to pull the card out
Positive finding: The examiner can easily pull the card free - indicates weak palmar interossei (ulnar nerve palsy)
In a normal hand: The patient grips the card firmly and the examiner cannot easily pull it out.
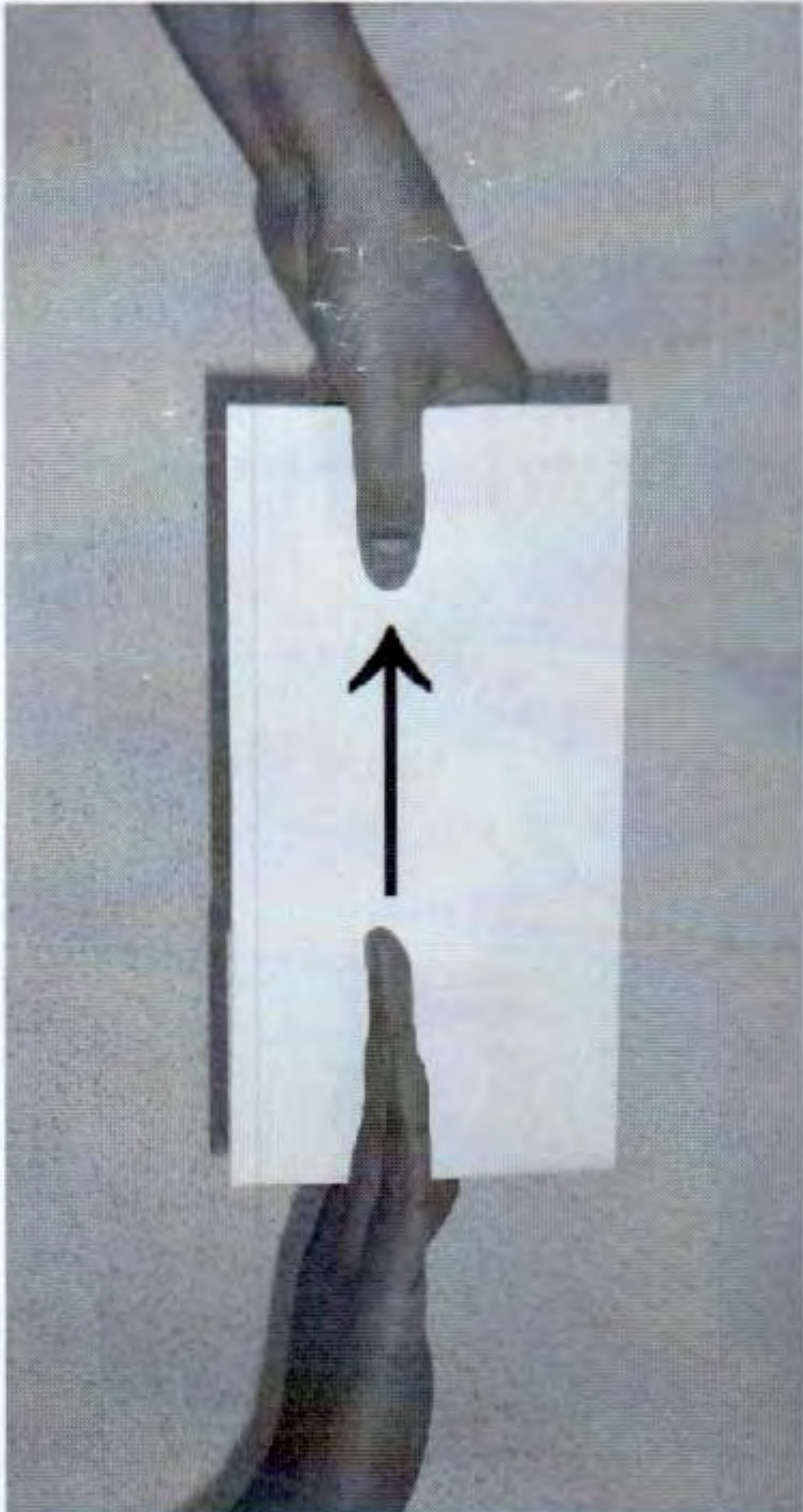
Card test - the card is held between two extended fingers; the examiner attempts to pull it out to assess palmar interosseous strength - S Das Manual on Clinical Surgery 13th Ed
Clinical note: The test can be performed between any two adjacent fingers. Testing between the ring and little fingers is particularly sensitive for early ulnar palsy.
Side-by-Side Comparison
| Feature | Egawa Test | Card Test |
|---|---|---|
| Muscle tested | Dorsal interossei | Palmar interossei |
| Action tested | Finger abduction | Finger adduction |
| Finger used | Middle finger specifically | Any two adjacent fingers |
| Hand position | Palm down, flat on table | Fingers extended, upright |
| Patient action | Move middle finger sideways | Hold card between fingers |
| Examiner action | Observes movement | Pulls card out |
| Positive result | Cannot deviate middle finger | Card easily pulled out |
| Nerve tested | Deep branch, ulnar nerve | Deep branch, ulnar nerve |
Key teaching point: Together, these two tests cover the complete interosseous motor function of the ulnar nerve:
- DAB - Dorsal interossei ABduct (Egawa test)
- PAD - Palmar interossei ADduct (Card test)
Both test the deep branch of the ulnar nerve, so they are affected in both high ulnar palsy (above elbow) and low ulnar palsy (Guyon's canal). They are not useful for distinguishing the level of the lesion - Froment's sign and FCU/FDP testing are needed for that. - S Das Manual on Clinical Surgery 13th Ed; Orthofixar
This is a shared conversation. Sign in to Orris to start your own chat.