Can you show me the real image of the pancreatic tail cancer
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have a rich set of real images from authoritative medical textbooks. Here is a comprehensive answer with all the images:
Real Images of Pancreatic Tail Cancer
Here are actual clinical and pathological images from major medical textbooks, covering imaging, histopathology, and multimodality views.
1. CT & MRI: Large Pancreatic Tail Neuroendocrine Tumor with Metastases
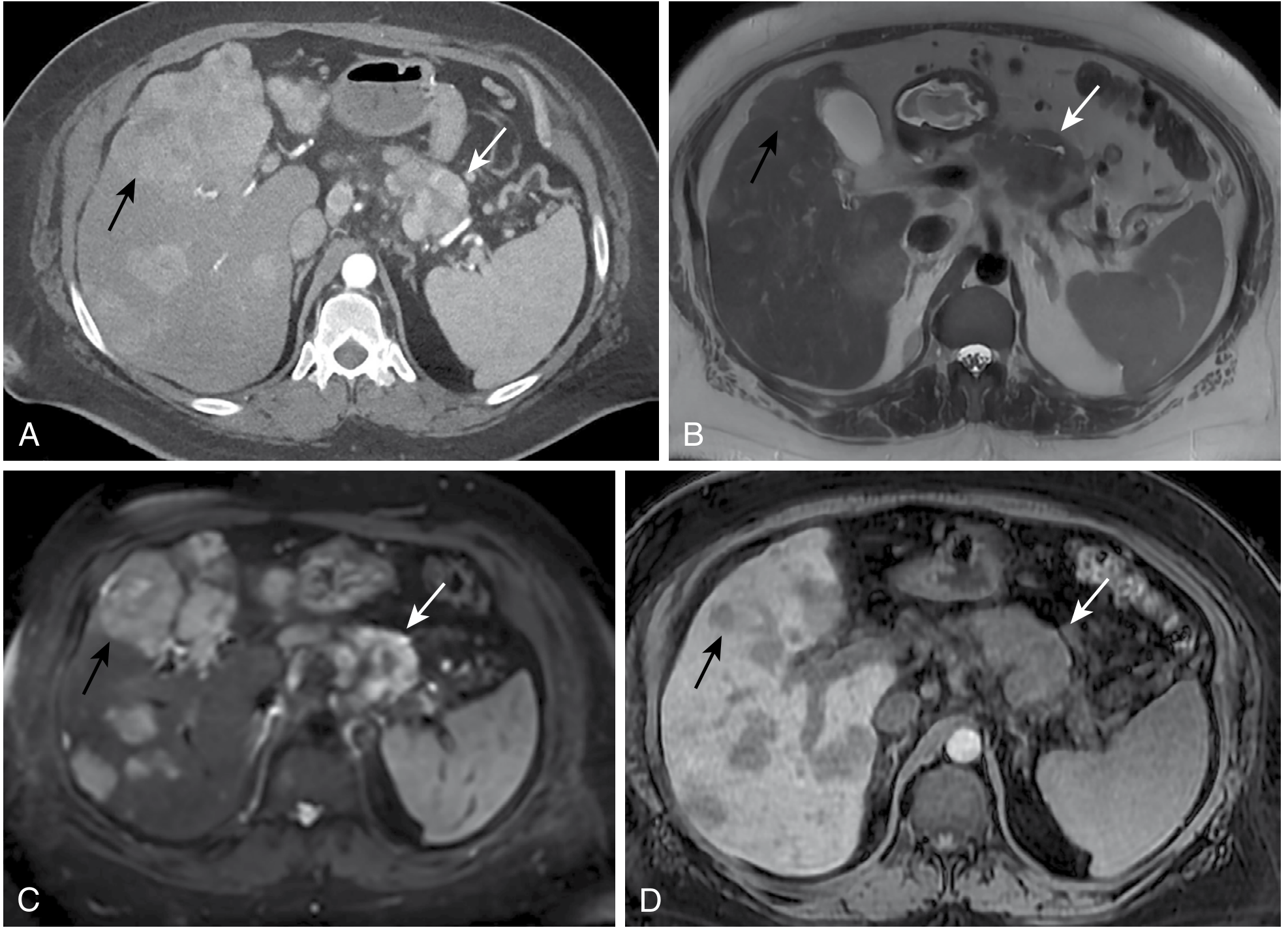
(A) Arterial-phase CT shows a large mass in the pancreatic tail (white arrows) with liver metastases (black arrow). (B) T2-weighted MRI, (C) Diffusion-weighted MRI, (D) T1-weighted MRI showing the same tumor - note diffusion images give the best delineation of liver lesions. - Sabiston Textbook of Surgery, 11e
2. CT Scan of Small Pancreatic Tail Lesion (Incidental Finding)
(A) Axial arterial-phase CT showing an 8-mm arterialy enhancing lesion in the pancreatic tail (arrow). (B) 10-mm lesion in the pancreatic body. (C) T1-weighted MRI of a pancreatic head lesion for comparison. - Sabiston Textbook of Surgery, 11e
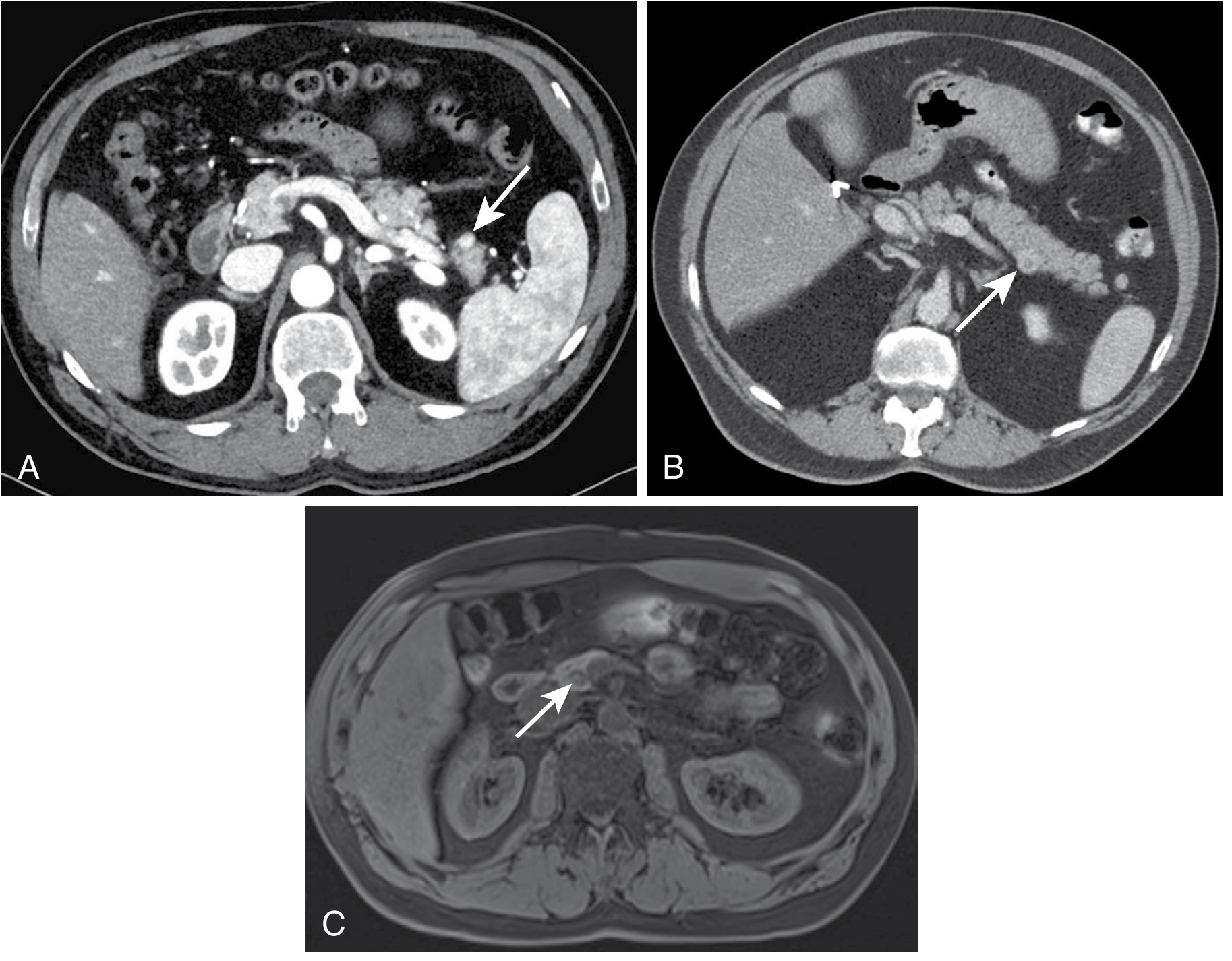
3. Pancreatic Cystic Lesions in the Tail (Including Malignant Transformation)

(A) T2-weighted MRCP showing a lobulated cystic structure in the posterior body - surgical histopathology revealed an infiltrating moderately differentiated adenocarcinoma in a background of IPMN. (B) CT scan showing a well-circumscribed hypodense cyst in the pancreatic tail (arrow) - a mucinous cystic neoplasm (MCN) with low-grade dysplasia. (C) MRI of a lobulated microcystic serous cystadenoma in the tail. - Harrison's Principles of Internal Medicine, 22e
4. Histopathology of Pancreatic Ductal Adenocarcinoma (PDAC)
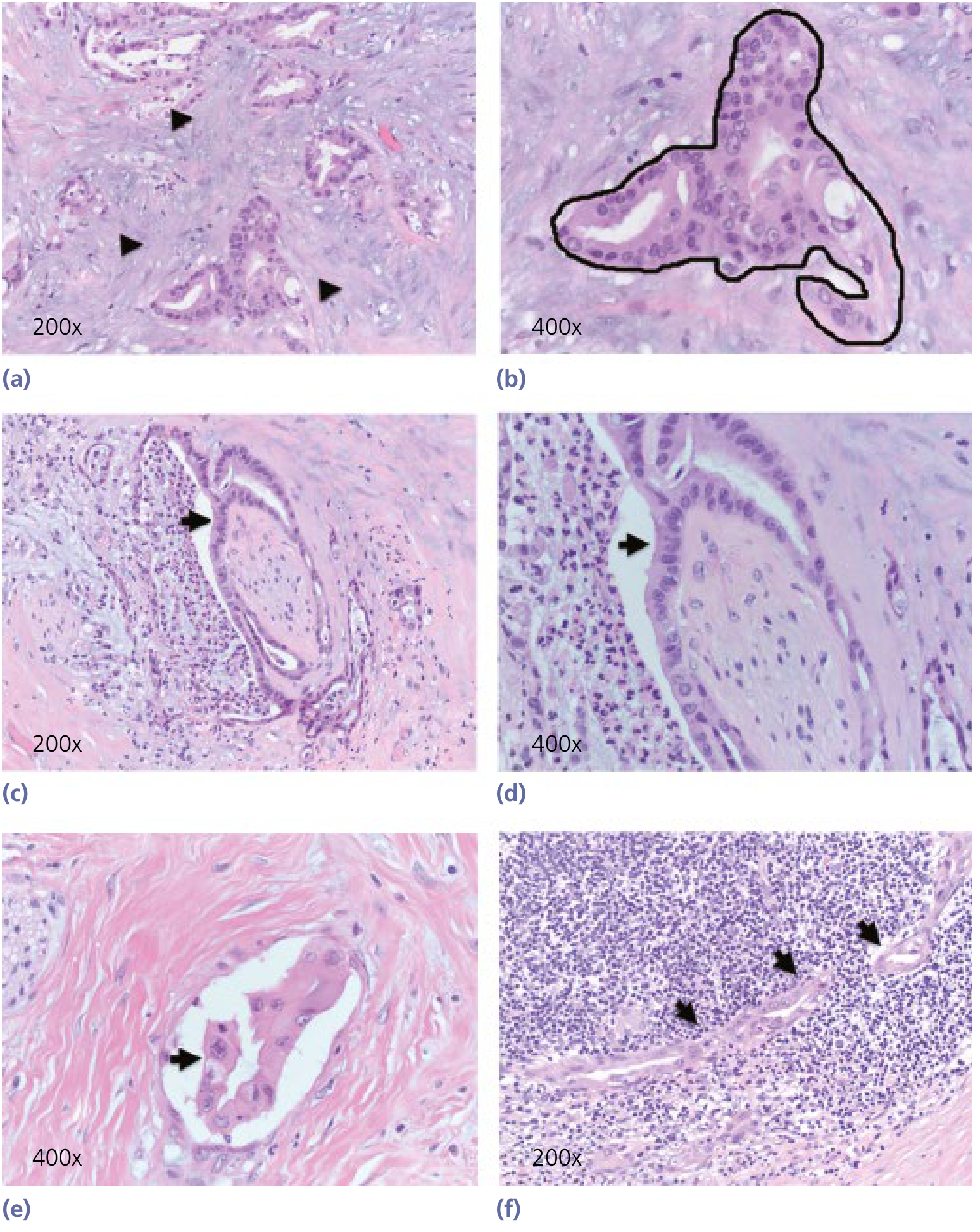
(a) The intense desmoplastic stroma characteristic of pancreatic cancer (arrowheads) at 200x. (b) Infiltrating glands with nuclear hyperchromatism, pleomorphism, and prominent nucleoli at 400x. (c, d) Perineural invasion by cancer cells (arrowheads) - a hallmark and poor prognostic feature. (e, f) Cancer cells invading vascular/lymphatic vessels and lymph nodes (arrowheads). - Yamada's Textbook of Gastroenterology, 7e
Key Points About Pancreatic Tail Cancer
- Only ~15% of pancreatic cancers arise in the body or tail vs. 60-70% in the head
- Tail lesions are often diagnosed late because they don't cause early biliary obstruction or jaundice - symptoms (back pain, weight loss, new-onset diabetes) are non-specific
- On CT, adenocarcinoma appears as a hypoattenuating (low-density) mass - less vascular than surrounding pancreatic tissue
- The signature microscopic feature is dense desmoplastic stroma (fibrous reaction around the tumor)
- Perineural invasion and vascular invasion (seen in panels c-f above) are common and carry poor prognosis
- Treatment for resectable tail cancer is distal pancreatectomy (often with splenectomy)
Sources: Sabiston Textbook of Surgery 11e, Harrison's Principles 22e, Yamada's Textbook of Gastroenterology 7e, Grainger & Allison's Diagnostic Radiology
This is a shared conversation. Sign in to Orris to start your own chat.