Everything about principles of fracture fixation, the implants etc
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
Loading Image
Reading File
I now have extremely rich, comprehensive material from Rockwood and Green's (2025) and Campbell's Operative Orthopaedics (2026). Let me compile this into a definitive, well-structured response.
Principles of Fracture Fixation and Implants
Sources: Rockwood and Green's Fractures in Adults, 10th ed. (2025); Campbell's Operative Orthopaedics, 15th ed. (2026); Bailey and Love's Short Practice of Surgery, 28th ed.; Pye's Surgical Handicraft, 22nd ed.
1. Fundamental Concept: The "Race" Between Healing and Fixation Failure
Fracture fixation is fundamentally a race between bone healing and construct failure. Since fixation constructs experience cyclic loading with every patient movement, a fixation construct that is not adequately durable will eventually fail by mechanical fatigue - unless the bone heals first. The biologic requirements to promote healing and the mechanical requirements to ensure durable fixation must therefore be weighed together.
This gave rise to what has been called the "paradox of internal fixation": rigid fixation restores function, while flexibility is needed to stimulate callus formation and natural bone healing. Both requirements are mutually exclusive to a degree, and the surgeon must consciously choose which healing mode to target.
"Management of a fractured bone requires the combined consideration of biologic and mechanical aspects to create a biomechanically sound fixation construct." - Rockwood & Green's, 2025
2. The Two Modes of Fracture Healing
The first decision in fracture fixation planning is: which healing mode am I targeting?
A. Natural (Secondary) Bone Healing - Callus Formation
- Requires relative stability - controlled interfragmentary motion
- Achieved with: functional bracing, external fixators, intramedullary nails, bridge plating
- Proceeds through inflammation → soft callus → hard callus → remodeling
- Callus bridges the fracture from the outside, not directly across the bone ends
- The extramedullary callus contributes far more to repair than intramedullary callus (bending stiffness increases with 4th power of distance from neutral axis)
| Healing Tissue | Max Strain (%) | Tensile Strength (N/mm²) |
|---|---|---|
| Hematoma | 100 | 0.1 |
| Soft callus | 10-12.8 | 4-19 |
| Hard callus | 2 | ~40 |
| Lamellar bone | 1 | ~100 |
B. Primary (Direct) Bone Healing
- Requires absolute stability - no interfragmentary motion
- Achieved with: compression plating (DCP), lag screw fixation
- Bone heals directly across the fracture by Haversian remodeling without callus
- Requires precise anatomic reduction with interfragmentary compression
- Suppresses natural callus healing
Critical point: A stiff construct with a residual fracture gap leads to atrophic nonunion because there is insufficient motion to stimulate callus yet the gap is not compressed. Clinically, locked plates used with biologic technique for distal femur fractures result in nearly 20% nonunion when overly stiff constructs are used with residual gaps.
3. The AO/ASIF Principles of Osteosynthesis
The four classical principles developed by the AO Group (Arbeitsgemeinschaft für Osteosynthese) remain the foundation:
- Anatomic reduction - particularly important for intra-articular fractures
- Stable fixation - appropriate to the fracture pattern and the healing mode desired
- Preservation of blood supply - to bone fragments and soft tissues (biologic fixation)
- Early, active mobilization - of adjacent muscles and joints
4. General Indications for Internal Fixation
(Pye's Surgical Handicraft; Bailey and Love's)
Indications:
- Position cannot be held by external techniques
- Need to avoid prolonged bed immobilization
- Need for early joint mobilization
- Multiple injuries - early fixation improves survival and reduces morbidity
- Intra-articular fractures requiring anatomic reduction
Advantages:
- Accurate reduction and maintenance of position
- Early patient and joint mobilization
- May encourage union
- Reduces hospital stay
Disadvantages and risks:
- Infection - can prejudice union and cause long-term morbidity
- Operative complications and inadequate fixation
- Implant may require removal; stress protection and osteoporosis under plate
- If fixation is inadequate, the patient has disadvantages of both internal and external fixation with few benefits of either
5. Implants: Screws
A. ASIF/AO Cortical Screws
- Threaded their entire length; available in multiple diameters
- Can function as positional or lag screws for interfragmentary compression (over-drilling the near cortex)
- Originally required pre-tapping; modern screws are self-tapping
B. Cancellous Screws
- Larger threads for more purchase in soft cancellous/metaphyseal bone
- Available in various sizes; the malleolar screw (4.5 mm) has a self-tapping trephine tip
- Washers used to increase interfragmentary compression or reattach ligamentous avulsions
C. Self-Tapping / Self-Drilling Screws
- Small cutting bit at the tip to remove bone debris
- Slightly less pullout strength than tapped screws
- Commonly used for external fixation pins
D. Locking Screws
- Self-tapping screws that lock into the plate head
- Require precise predrilling
- The screw-plate construct acts as a fixed-angle device - resistance to pullout is through the entire plate-screw construct, not just bone-screw interface
- Particularly valuable in osteoporotic bone
E. Lag Screws (Principle)
- The most powerful technique for interfragmentary compression
- Near cortex overdrilled (gliding hole) = screw head compresses fragment against far cortex
- Any cortical screw can act as a lag screw
F. Cannulated Screws
- Allow insertion over a guidewire for precise placement
- Used for small fragments, femoral neck fractures, scaphoid fractures

6. Implants: Plates
Principles of Plate Fixation (Campbell's, 2026)
- Plates neutralize deforming forces that screws alone cannot counter
- Adequate screw fixation is required: 6-8 cortices of purchase on both sides of the fracture (except buttress plates)
- Plates should be of sufficient length - the larger the bone and greater the stresses, the longer the plate
- Incorrect screw placement or sequence results in displacement or loss of reduction
- Avoid overtorquing screws; retighten all screws before closure to allow for stress relaxation
- Plates should be contoured to the bone; a poorly fitting plate will displace the fracture as screws are tightened
Tension Band Principle (Pauwels)
- Converts tensile forces to compressive forces on the convex side of an eccentrically loaded bone
- Plate placed on the tension (convex) side - bone receives compressive forces
- If placed on the concave side, the plate bends, fatigues, and fails
Types of Plates (Campbell's Table 58.11)
| Plate Type | Fracture Type / Action | Key Points |
|---|---|---|
| Neutralization | Torsional, bending, shear forces + butterfly/wedge fragments | Used with interfragmentary lag screw; technique same as compression but no compression through plate holes |
| Compression (DCP) | Transverse or short oblique diaphyseal (AO type A); after lag fixation of wedge fragment | Self-compression holes translate the screw as it engages the plate, generating compression; applied to tension side |
| Buttress | Metaphyseal-epiphyseal fractures (tibial plateau, pilon) | Negates compressive + shear forces; plate anchored to main stable fragment; screws inserted toward fracture shoulder |
| Bridge | Comminuted/segmental fractures; bone defects | Spans comminuted zone; indirect reduction; biologic fixation; often requires bone grafting |
Low-Contact DCP (LC-DCP)
- Contoured to reduce contact area under the plate
- Improves periosteal blood supply
- Allows narrow area of circumferential callus to regenerate at the fracture site
- Bidirectional compression through specially designed holes
Locking Plates
- Screw heads lock into threaded holes - the construct acts as a fixed-angle internal fixator
- Particularly useful in: osteoporotic bone, periarticular fractures, periprosthetic fractures, metaphyseal comminution
- Warning: Overly stiff locking plate constructs with residual fracture gaps can cause atrophic nonunion (~20% rate in distal femur)
- Should ideally be used with working length (bridging empty holes near the fracture) to allow controlled motion for callus
7. Implants: Intramedullary (IM) Nails
Principle
- Inserted through the medullary canal (centromedullary)
- Contact bone at multiple points; rely on longitudinal bone-nail contact for axial and rotational stability
- Act as internal splints - load-sharing devices, not load-bearing
- Provide relative stability - natural/callus healing is expected
Key Features
- Interlocking screws - placed near both ends of the nail to resist axial and rotational deformation; allow longer nails; expand indications to metaphyseal fractures
- Reamed vs. unreamed: Reamed nails have larger diameter, tighter fit in medullary canal, better torsional and translational shear stiffness; unreamed nails preserve endosteal blood supply but have lower stiffness
- Dynamization: Removing interlocking screws converts a static to dynamic nail, facilitating telescoping and closer contact of fracture surfaces - but also decreases shear stiffness
Stiffness Considerations
- Unreamed nails have low translational shear stiffness - small forces can cause varus/valgus deformity, especially in fractures away from the isthmus where the canal widens
- Torsional loading creates rotational angles of 6-47 degrees between fracture surfaces with unreamed nails
- Shear motion (translational + rotational) is the principal mechanical concern for intramedullary fixation
Indications
- Method of choice for most long bone diaphyseal fractures (tibia, femur)
- Expanding to include metaphyseal fractures
- Load sharing with bone (versus load-bearing plates)
- Early mobilization possible
8. Implants: External Fixators
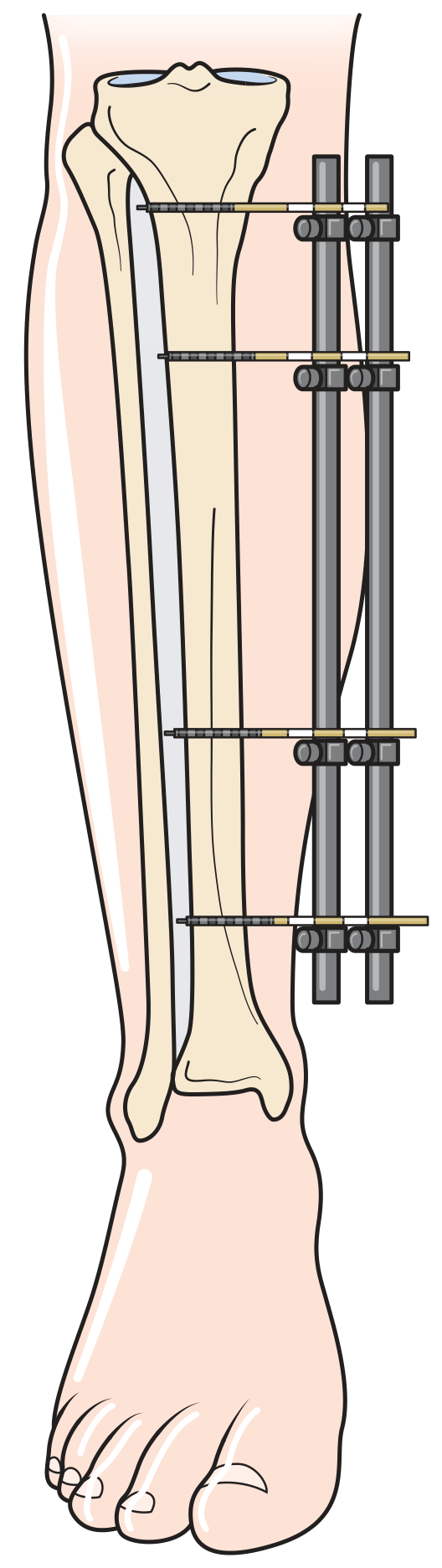
Principle
- Percutaneous pins/wires anchor to bone above and below the fracture; connected by external rods/rings
- Provides relative stability; fractures heal with callus
Types
| Type | Description |
|---|---|
| Monolateral | Half-pins into bone connected by a single rod/bar; uniplanar |
| Circular (Ilizarov) | Circumferential rings secured by tensioned wires and half-pins; multiplanar; more suited for definitive treatment |
| Hybrid | Combination of ring/tubular rod frame with half-pins and fine wires |
| Taylor Spatial Frame | Computer-assisted multiaxial correction frame; allows gradual deformity correction |
Factors Maximizing Frame Stability
- Appropriate reduction
- Larger diameter half-pins
- Decreased bone-to-rod distance
- Additional half-pins
- Increased half-pin spacing
- Pins in different planes
- Additional rods
Specific Indications (Bailey and Love's; Campbell's)
- Damage control orthopaedics - rapid stabilization in polytrauma patient not fit for definitive fixation
- Open fractures - severe contamination, extensive soft tissue injury
- Temporary spanning of a dislocated joint after reduction
- Pelvic ring injuries
- Infected fractures / fractures with active infection
- Fractures with significant soft tissue compromise requiring wound access
- Lengthening and deformity correction (Ilizarov)
| Advantages | Disadvantages |
|---|---|
| No interference with fracture site | Pin site infection (up to 30%) |
| Adjustable after application | Cumbersome for patient |
| Soft tissues remain accessible | Soft-tissue tethering |
| Rapid stabilization | Can interfere with subsequent internal fixation |
| Hardware easy to remove | More monitoring required |
Complication: Pin Track Infection
- Most common complication without proper technique
- Up to 30% incidence without meticulous pin site care
- Prevention: proper drilling technique, pin care protocol, antibiotics when indicated
9. Implants: Tension Band Wiring (TBW)
- Combines Kirschner wires (K-wires) with a figure-of-8 cerclage wire
- Classic indications: olecranon fractures, patella fractures, some greater tuberosity fractures
- Converts muscle-pull distraction forces into compression at the fracture surface
- Works best when the opposite cortex is intact to act as a fulcrum
10. Implants: Cerclage Wires and Cables
- Circumferential wires or cables around the bone
- Used for: periprosthetic fractures around stable stems, intraoperative fractures during arthroplasty
- Provide fixation without violating the medullary canal
- Cables less likely to cut through than wires
11. Biomechanical Considerations: Construct Design
Stiffness and Healing
- Too stiff: Suppresses callus formation; atrophic nonunion with residual gap
- Too flexible: Excessive interfragmentary motion prevents tissue differentiation; nonunion
- Optimal: Controlled motion that stimulates callus while remaining durable
Plate Construct Stiffness - Working Length
- The working length is the unsupported span of the plate between the innermost screws on each side
- Longer working length = more flexible construct (promotes callus)
- Shorter working length = stiffer construct (promotes direct healing)
Stress Risers After Implant Removal
- Screw holes left after plate removal create cortical defects
- Holes <10% of outer bone diameter: no change in torsional strength
- Holes 10-20% of bone diameter: large 34% drop in torsional strength
- Linear decrease in strength with larger defects
- After plate removal, patients should be counseled to protect the limb for a period
12. Special Situations
Osteoporotic Bone
- Standard cortical screws have poor pullout strength
- Locking screws/plates preferred - pullout resistance through entire construct
- Consider augmentation with bone cement for isolated areas
Open Fractures
- External fixation preferred initially for grade III B/C injuries
- Allows wound access and management
- Conversion to IM nail or plate possible once wounds are clean (typically 5-14 days)
- Timing of conversion is critical - pin-to-plate conversion increases infection risk
Damage Control Orthopaedics (DCO) vs. Early Total Care (ETC)
- DCO: temporary external fixation first, definitive fixation after resuscitation/stabilization
- ETC: definitive internal fixation within 24 hours in stable polytrauma patients
- The EAST multicenter trial (2023) showed lower extremity fracture fixation technique (DCO vs. ETC) influences neurological outcomes in patients with traumatic brain injury
Summary Table: Implant Choice by Fracture Location and Pattern
| Fracture | Preferred Implant | Principle |
|---|---|---|
| Femoral shaft | Reamed antegrade IM nail | Relative stability / callus |
| Tibial shaft | Locked IM nail | Relative stability / callus |
| Distal radius | Volar locking plate | Fixed-angle; bridge or compression |
| Femoral neck | Cannulated screws / DHS | Lag + neutralization / sliding |
| Intertrochanteric femur | Cephalomedullary nail / DHS | Load-sharing sliding |
| Tibial plateau | Locking buttress plate | Buttress/fixed-angle |
| Olecranon | Tension band wiring / plate | Tension band |
| Patella | TBW / partial patellectomy | Tension band |
| Open fractures, polytrauma | External fixator first | Damage control |
| Deformity/infected bone | Ilizarov / Taylor frame | Distraction osteogenesis |
References:
- Rockwood and Green's Fractures in Adults, 10th ed. 2025 (pp. 22-111)
- Campbell's Operative Orthopaedics, 15th ed. 2026 (Chapter 58)
- Bailey and Love's Short Practice of Surgery, 28th ed. (Chapter 32)
- Pye's Surgical Handicraft, 22nd ed. (Chapter 12)
Everything stepwise simpler with detailed explanation of TKR surgical steps and approach
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
I now have comprehensive, detailed surgical steps from Campbell's Operative Orthopaedics 2026. Let me now compile the full, clear, stepwise answer.
Total Knee Replacement (TKR) - Complete Stepwise Guide
Source: Campbell's Operative Orthopaedics, 15th Ed. 2026 (Chapter 8)
Overview of What TKR Involves
Total Knee Replacement (also called Total Knee Arthroplasty - TKA) removes the damaged surfaces of the distal femur, proximal tibia, and optionally the patella, replacing them with metal and plastic components that recreate a smooth, painless joint. The goal is:
- Eliminate pain
- Restore mechanical alignment (correct varus/valgus deformity)
- Restore range of motion
- Balance soft tissues so the joint is stable throughout the arc of motion
Pre-operative Planning
Before the patient enters the operating room, the surgeon must:
- Review long-standing (hip-to-ankle) radiographs to measure the mechanical and anatomic axes of the femur and tibia
- Determine the valgus correction angle (VCA) for the distal femoral cut - typically 5-7 degrees
- Identify deformity pattern (varus/valgus/flexion contracture)
- Template implant sizes
- Plan the ligament balancing strategy based on the deformity
Patient Positioning
- Patient placed supine on the operating table
- A lateral post or leg holder is placed at the thigh to stabilize the leg during surgery
- The leg is positioned to allow the knee to be flexed to 90 degrees (a foot rest or leg holder is used)
- A pneumatic tourniquet is applied to the proximal thigh (typically inflated to 250-300 mmHg) to create a bloodless field
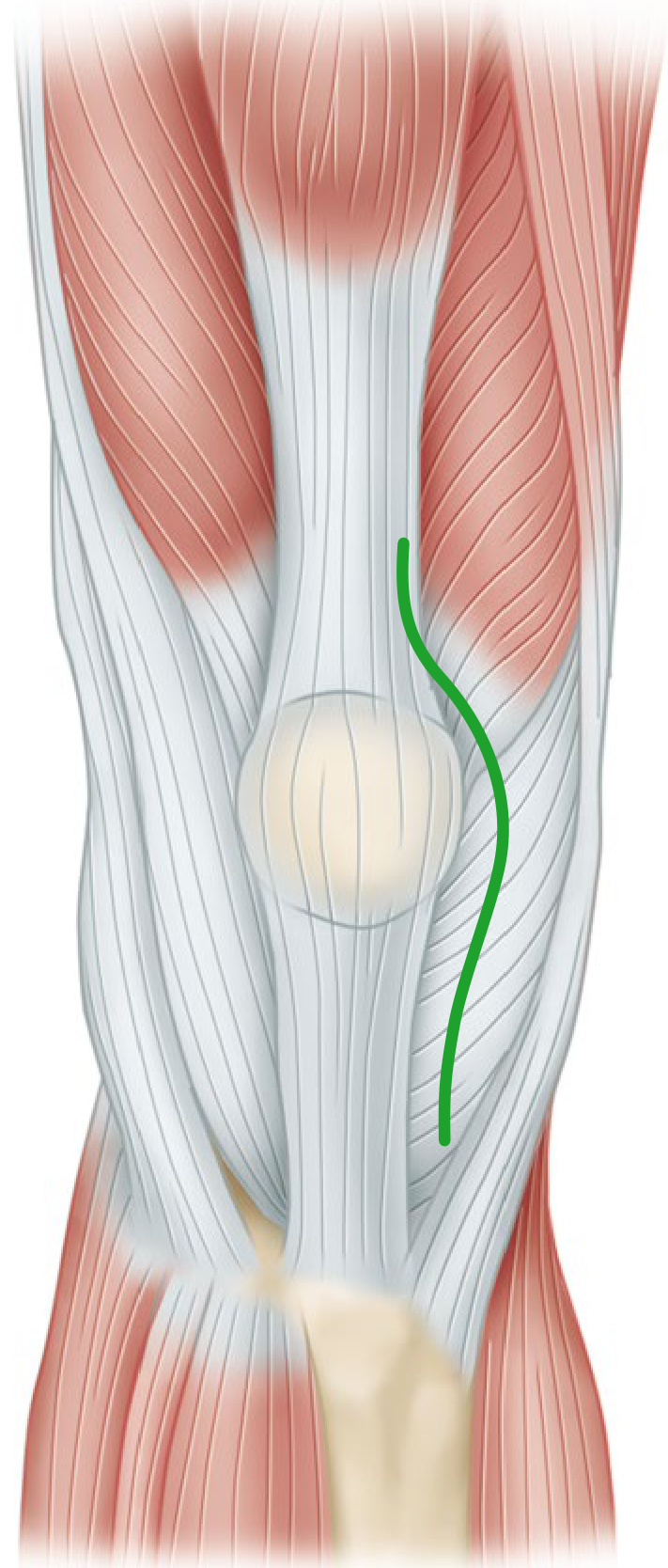
Step 1: Skin Incision
The standard incision is an anterior midline (straight) skin incision.
Key points:
- Incision is made with the knee in flexion so subcutaneous tissue falls medially and laterally, improving exposure
- Runs from approximately 5-8 cm above the superior pole of the patella, over the midline, to 3-4 cm below the tibial tuberosity
- If a previous scar exists, incorporate it - use the most lateral usable scar since blood supply to the anterior knee comes predominantly from the medial side
- Incision must be long enough to avoid excessive skin tension (skin necrosis risk)
- The infrapatellar branch of the saphenous nerve will almost always be divided - warn the patient preoperatively about lateral knee numbness
Step 2: Deep Approach (Arthrotomy)
Several approaches exist. The most common is:
A. Medial Parapatellar Approach (Standard - most common)
- Incise the retinaculum along the medial border of the quadriceps tendon, leaving a 3-4 mm cuff of tendon on the vastus medialis obliquus (VMO) for later re-attachment
- Continue the incision around the medial side of the patella
- Extend 3-4 cm onto the anteromedial tibia along the medial border of the patellar tendon
- Elevate the anteromedial capsule and deep MCL subperiosteally off the tibia to the posteromedial corner
- Extend the knee and evert the patella laterally (or subluxate it if eversion is difficult - in obese patients, develop the lateral subcutaneous flap first)
- Flex the knee to 90 degrees
Danger: Never put excessive tension on the patellar tendon attachment at the tibial tubercle. Avulsion of the patellar tendon is difficult to repair and can be a devastating complication.
B. Subvastus ("Southern") Approach
- Same anterior midline skin incision
- Retinacular incision goes below the VMO - the superficial fascia overlying VMO is incised and the entire extensor mechanism is mobilized posteriorly to the medial intermuscular septum
- VMO origin is lifted off the septum to ~10 cm proximal to the adductor tubercle
- Entire extensor mechanism is dislocated laterally as a unit without cutting it
- Advantage: Preserves extensor mechanism integrity, faster quadriceps recovery, better vascularity to patella, less need for lateral release
- Disadvantage: Limited exposure in obese patients or after previous knee surgery
C. Midvastus Approach
- Same skin incision
- VMO muscle is split in line with its fibers starting at the superomedial border of the patella, extending proximally toward the intermuscular septum
- A safe zone of 4.5 cm from the patella margin can be safely split
- Preserves the supreme genicular artery and quadriceps tendon
- Contraindicated in: obesity, previous tibial osteotomy, preoperative flexion <80 degrees
Step 3: Synovectomy and Joint Preparation
Once inside the joint:
- Remove the ACL (anterior cruciate ligament) - it is always sacrificed in TKA
- Remove the anterior horns of both menisci
- Remove osteophytes from around the femoral condyles, tibial plateau, and intercondylar notch - these cause soft tissue imbalance and component malposition if left
- If a PCL-substituting (posterior-stabilized) design is planned, remove the PCL now or later with the box cut
- Subluxate and externally rotate the tibia - relaxes the extensor mechanism and decreases risk of patellar tendon avulsion
- Excise the infrapatellar fat pad partially or completely to expose the lateral tibial plateau
- Place a levering retractor carefully adjacent to the lateral tibial plateau for exposure
Step 4: Tibial Cut
The proximal tibial cut is made first in most systems (though some systems do femur first).
Alignment
- The cut must be perpendicular to the mechanical axis of the tibia in the coronal plane
- A 3-5 degree posterior slope is given (matches the native tibial slope) to allow flexion
- Extramedullary (EM) alignment is preferred for the tibia - the alignment rod points to just medial to the center of the ankle (approximately 2 mm medial to the midpoint of the malleolar axis)
- Intramedullary alignment can also be used but carries a small risk of fat embolism
Amount of Bone Removed
- Usually 8-10 mm from the less-involved (normal) tibial plateau
- Deeper cuts may be needed if there is significant bone loss, but the tibial component should always rest on good cortical bone
Key Pitfall
Bone removed from the proximal tibia affects both the flexion and extension gaps equally - so if you need more space, this is where to remove more bone.
Step 5: Distal Femoral Cut
Alignment
- The cut is made perpendicular to the mechanical axis of the femur
- This requires applying a valgus angle of 5-7 degrees (the VCA) to the anatomic axis of the femur
- This angle is measured preoperatively from long-standing radiographs
- Intramedullary (IM) alignment is standard on the femoral side because landmarks are not palpable
- IM entry point is placed a few mm medial to midline, anterior to the PCL origin
Amount of Bone Removed
- Typically the same thickness as the distal femoral component being implanted (to maintain joint line level)
- For flexion contracture correction: additional 1-2 mm can be resected, but avoid elevating the joint line by more than 4 mm
- For PCL-substituting designs: add 2 mm extra to the distal cut to account for the increase in flexion gap when PCL is sacrificed
Step 6: Femoral Sizing and Rotation - Four-in-One Femoral Cuts
After the distal femoral cut, the femoral sizing guide is placed to determine the correct component size and to set the rotation of the femoral component.
Rotation Landmarks (4 reference methods)
| Reference | Description |
|---|---|
| Transepicondylar axis (TEA) | Line between medial and lateral femoral epicondyles - most reliable |
| AP (Whiteside's) axis | Line from the sulcus of the trochlea to the top of the intercondylar notch; posterior cut perpendicular to this |
| Posterior condyles | Make cut in 3 degrees of external rotation off the posterior condylar line (unreliable in valgus knees with hypoplastic lateral condyle) |
| Tibial cut surface | Parallel to the proximal tibial cut when in extension |
Why does rotation matter? Internal rotation of the femoral component causes lateral patellar tilt and patellofemoral instability. Excessive external rotation widens the medial flexion gap causing flexion instability.
The Four-in-One Cut Block
Once rotation and size are set, a single cutting block makes four simultaneous or sequential cuts:
- Anterior femoral cut - resects the anterior distal femoral cortex
- Posterior femoral cut - resects the posterior femoral condyles
- Anterior chamfer cut - transitions from the distal cut to the anterior cut
- Posterior chamfer cut - transitions from the distal cut to the posterior cut
These 5 surfaces (distal + 4 peripheral cuts) form the shaped bone that accepts the femoral component.
Step 7: Tibial Preparation
- The tibial template is placed on the tibial cut surface to select the appropriate size
- Size to match the tibial cortex while avoiding overhang (overhang causes pain) or underhang (underhang sacrifices stability)
- Rotational alignment of the tibial component is set - typically aligned to the medial one-third of the tibial tubercle or to the junction of the medial and middle thirds
- The keel slot is cut using a punch or saw to accommodate the tibial component's central keel/peg
- Correct rotation is critical - internal rotation of the tibial component lateralizes the tubercle, increases the Q-angle, and causes lateral patellar subluxation
Step 8: Patellar Preparation (If Resurfacing)
Not all surgeons resurface the patella routinely, but when done:
- The patella is held with a clamp and its thickness measured with calipers
- A flat resection is made to remove the articular surface (typically 8-10 mm depth)
- Residual patellar bone thickness should be at least 12-15 mm to avoid fracture risk
- The patellar component (a polyethylene button) is centered on the bone, but should be medialized to approximate the median eminence (not centered on the cut surface - centering forces the bone to track with a higher Q-angle)
- An overall patellar thickness (bone + implant) equal to original thickness is the goal - increasing it anteriorly causes instability or limited flexion
Step 9: Trial Reduction and Gap Balancing
Before cementing the final components, trial components are inserted to assess:
Checking the Gaps
Two gaps must be equal and rectangular:
| Gap | How to check | What it means |
|---|---|---|
| Extension gap | Full extension with spacer/tensioner | Must equal flexion gap for stability |
| Flexion gap | 90 degrees flexion with trial components | If larger than extension gap, knee will be loose in flexion |
A symmetric rectangular flexion = extension gap is the goal.
| Gap Problem | Cause | Fix |
|---|---|---|
| Flexion gap > extension gap | Too much posterior femoral resection; PCL too tight | Use smaller femoral component (anterior reference); adjust rotation; check PCL |
| Extension gap > flexion gap | Too much distal femoral resection; flexion contracture | Downsize tibial insert; check posterior capsule |
| Both gaps too small | Not enough bone removed | Remove more proximal tibia equally |
| Both gaps too large (lax) | Too much bone removed | Use thicker tibial polyethylene insert |
Soft Tissue Balancing in Varus Knee (most common deformity)
Medial structures are contracted. Release in sequence (stepwise - only release what is needed):
- Deep MCL off the tibia subperiosteally (already done during exposure)
- Posteromedial capsule
- Semimembranosus insertion
- Posterior oblique ligament
- Superficial MCL (if still tight)
- Pes anserinus (rarely needed)
Soft Tissue Balancing in Valgus Knee
Lateral structures are contracted. Release stepwise:
- Lateral capsule (posterolateral corner)
- Pie-crusting of the iliotibial band (ITB) - multiple small perforations rather than complete release
- Popliteus tendon - increases flexion gap laterally more than extension gap
- If still unbalanced: posterior capsule off lateral femoral condyle
- Lateral head of gastrocnemius
- As last resort: MCL advancement on medial side
"No-Thumb" Patellar Tracking Test
- With trial components in place and the knee taken through a full range of motion, the patella should track centrally in the trochlear groove without the surgeon holding it
- If it tracks laterally: consider lateral retinacular release, check femoral and tibial component rotation
Step 10: Cementation and Final Implantation
Cementation (most common)
- Irrigate and dry all bony cut surfaces meticulously - bone must be dry for cement to bond
- Mix polymethylmethacrylate (PMMA) bone cement to the appropriate consistency ("doughy" phase)
- Apply cement to the cut bone surfaces (not just the implant)
- Tibial component first - seat the tray firmly, ensuring correct rotation; remove cement squeeze-out with a curette
- Femoral component next - seat firmly using a femoral punch; remove excess cement, especially posteriorly
- Extend the knee with a trial spacer to confirm complete seating of the femoral component
- Cement the patellar component if used
- Retighten all components once cement has hardened
- Use a tibial spacer of adequate thickness to hold the knee in full extension during cement curing - too thin causes posterior liftoff
Key rule: Follow the specific instructions for the bone cement being used - small variations in technique directly affect long-term survivorship.
Cementless Fixation (alternative)
- Requires more accurate bone cuts - no cement to compensate for gaps
- Relies on intimate apposition (bone-prosthesis gaps >0.5 mm fill with fibrous tissue, not bone)
- Trial tray is tested by pressing the periphery - any movement = revise the surface
- Bone ingrowth is maximal around fixation screws and pegs; these are essential for initial stability
Final Polyethylene Insert
- After the metal components are cemented, the final polyethylene tibial insert is snapped/locked into the tibial tray
- Remove all bone and cement debris before inserting the poly - third-body wear is a long-term failure mechanism
Step 11: Wound Closure
- Release the tourniquet after implantation; pack with moist sponges
- Identify and cauterize bleeding geniculate arteries (medial and lateral)
- Suction drains are no longer routinely recommended - no difference in infection or hematoma rates; drained patients actually receive more blood transfusions
- Close the retinaculum/quadriceps mechanism with interrupted or continuous strong absorbable sutures - the medial parapatellar incision is closed layer by layer, restoring the VMO cuff
- Close subcutaneous tissue
- Close skin with staples or sutures
- Sterile dressing; compression bandage applied
Summary: The Surgical Sequence at a Glance
PATIENT SETUP
↓
1. Tourniquet inflation
↓
2. Anterior midline skin incision (knee in flexion)
↓
3. Medial parapatellar arthrotomy (or subvastus / midvastus)
↓
4. Patellar eversion; ACL excision; meniscectomy; osteophyte removal
↓
5. TIBIAL CUT → perpendicular to mechanical axis, 3-5° posterior slope
↓
6. DISTAL FEMORAL CUT → 5-7° valgus angle via IM alignment
↓
7. FEMORAL SIZING + ROTATION → TEA / Whiteside's axis reference; 3° ER off posterior condyles
↓
8. FOUR-IN-ONE FEMORAL CUTS (anterior, posterior, chamfers)
↓
9. TIBIAL PREPARATION → size, rotation, keel slot
↓
10. PATELLAR RESURFACING (optional)
↓
11. TRIAL REDUCTION → check gaps, balance ligaments (varus = medial release; valgus = lateral release/pie-crust)
↓
12. PATELLAR TRACKING TEST ("no thumb" test)
↓
13. CEMENTATION → tibia first → femur → patella
↓
14. FINAL POLY INSERT
↓
15. TOURNIQUET DOWN → hemostasis
↓
16. LAYERED WOUND CLOSURE
Key Numbers to Remember
| Parameter | Value |
|---|---|
| Valgus correction angle (distal femoral cut) | 5-7 degrees |
| Posterior tibial slope | 3-5 degrees |
| Femoral rotation off posterior condyles | 3 degrees external rotation |
| Joint line elevation limit | No more than 4 mm |
| Residual patellar bone after resection | Minimum 12-15 mm |
| PCL: if >75% released, switch to PS design | >75% released = instability risk |
| Bone-prosthesis gap for ingrowth success | <0.5 mm |
Source: Campbell's Operative Orthopaedics, 15th Ed. 2026, Chapter 8 (Techniques 8.1-8.9)
Reload
I'm here and ready! What would you like to explore next?
Same as above tkr
Here is the full TKR guide again, compiled from Campbell's Operative Orthopaedics 15th Ed. (2026):
Total Knee Replacement (TKR) - Complete Stepwise Guide
What Is TKR?
TKR removes the damaged surfaces of the distal femur, proximal tibia, and optionally the patella, replacing them with metal and polyethylene components. The goals are:
- Eliminate pain
- Restore mechanical alignment (correct varus/valgus deformity)
- Restore range of motion
- Balance soft tissues for stability throughout the arc of motion
Pre-operative Planning
- Long-standing hip-to-ankle radiographs to measure mechanical vs. anatomic axes
- Calculate the Valgus Correction Angle (VCA) for the distal femoral cut - typically 5-7 degrees
- Identify deformity pattern: varus / valgus / flexion contracture
- Template implant sizes
- Plan ligament balancing strategy
- Choose implant type: Cruciate-Retaining (CR) vs. Posterior-Stabilized (PS)
Patient Setup
- Supine position on the operating table
- Lateral post or leg holder at the thigh for stability
- Leg positioned to allow 90 degrees of knee flexion
- Pneumatic tourniquet on the proximal thigh (250-300 mmHg) for a bloodless field
STEP 1: Skin Incision
Standard: Anterior Midline (straight) Incision
- Make the incision with the knee in flexion - subcutaneous tissue falls aside, improving exposure
- Runs from ~5-8 cm above the superior pole of the patella to 3-4 cm below the tibial tuberosity
- If a previous scar exists, incorporate it - use the most lateral usable scar (blood supply to anterior knee comes from the medial side)
- Incision must be long enough to avoid skin tension and necrosis
- The infrapatellar branch of the saphenous nerve will be cut in most cases - warn the patient about lateral knee numbness preoperatively
STEP 2: Deep Approach (Arthrotomy)
Three approaches exist, all using the same anterior midline skin incision:
A. Medial Parapatellar Approach - Standard (Most Common)
| Step | Action |
|---|---|
| 1 | Incise the retinaculum along the medial border of the quadriceps tendon |
| 2 | Leave a 3-4 mm cuff of tendon on the VMO for re-attachment at closure |
| 3 | Continue incision around the medial border of the patella |
| 4 | Extend 3-4 cm onto the anteromedial tibia along the medial border of the patellar tendon |
| 5 | Elevate anteromedial capsule + deep MCL subperiosteally off the tibia to the posteromedial corner |
| 6 | Extend the knee; evert the patella laterally (or subluxate if eversion is difficult) |
| 7 | Flex the knee to 90 degrees |
Critical warning: Never put excessive tension on the patellar tendon attachment at the tibial tubercle - avulsion is very difficult to repair and is a devastating complication.
B. Subvastus ("Southern") Approach
- The VMO is mobilized off the medial intermuscular septum - the entire extensor mechanism is dislocated laterally as a unit without cutting it
- Advantage: Faster quadriceps recovery, better patellar vascularity, less lateral release needed
- Disadvantage: Limited exposure in obese patients or after previous knee surgery
C. Midvastus Approach
- VMO muscle is split in line with its fibers from the superomedial patellar border proximally
- Safe zone: 4.5 cm from the patella margin
- Preserves the supreme genicular artery
- Contraindicated in: obesity, previous high tibial osteotomy, preoperative flexion <80 degrees
STEP 3: Joint Preparation (Inside the Knee)
Once the joint is open:
- Remove the ACL - always sacrificed in TKR
- Remove anterior horns of both menisci
- Remove osteophytes around the femoral condyles, tibial plateau, and intercondylar notch (osteophytes cause soft tissue imbalance and component malposition)
- If using a PS design, remove the PCL now (or later with the box cut)
- Subluxate and externally rotate the tibia - relaxes the extensor mechanism, reduces patellar tendon avulsion risk
- Partially or fully excise the infrapatellar fat pad to expose the lateral tibial plateau
- Place retractors around the tibial plateau
STEP 4: Proximal Tibial Cut
Alignment
- Cut must be perpendicular to the mechanical axis of the tibia (coronal plane)
- 3-5 degrees of posterior slope in the sagittal plane (mirrors native tibial slope, aids flexion)
- Extramedullary (EM) alignment rod preferred for tibia - tip aimed 2 mm medial to the center of the ankle
- Intramedullary tibial alignment can be used but carries a small fat embolism risk
Amount of Bone Removed
- Usually 8-10 mm from the less-involved (less damaged) tibial plateau
- The tibial component must rest on good cortical bone
- Tibial bone removal affects flexion AND extension gaps equally - if more space is needed in both gaps, remove more here
STEP 5: Distal Femoral Cut
Alignment
- Cut perpendicular to the mechanical axis of the femur
- Applied valgus angle = VCA (5-7 degrees) measured off the anatomic axis
- Intramedullary (IM) alignment is standard on the femoral side (landmarks not palpable externally)
- IM rod entry point: few mm medial to midline, anterior to PCL origin
Amount of Bone Removed
- Same thickness as the distal femoral component to maintain joint line level
- For flexion contracture: additional 1-2 mm can be resected; do not elevate the joint line by >4 mm
- For PS design: add 2 mm extra to the distal cut (compensates for flexion gap increase when PCL is sacrificed)
STEP 6: Femoral Sizing and Setting Rotation
A sizing guide is placed on the distal femoral cut to determine component size and set rotation.
Rotation Reference Landmarks
| Method | Description | Notes |
|---|---|---|
| Transepicondylar axis (TEA) | Line between medial and lateral epicondyles | Most reliable |
| Whiteside's AP axis | Line from trochlear sulcus to top of intercondylar notch; cut perpendicular to it | Very reliable |
| Posterior condylar line | 3 degrees external rotation off posterior condyles | Unreliable in valgus (hypoplastic lateral condyle) |
| Tibial cut surface | Make cut parallel to tibial cut with knee in extension | Used as a check |
Why rotation matters: Internal rotation of the femoral component → lateral patellar tilt → patellofemoral instability. Excessive external rotation → medial flexion gap opens up → flexion instability.
The Four-in-One Femoral Cutting Block
Once size and rotation are confirmed, the 4-in-1 cutting block makes:
- Anterior femoral cut - resects anterior distal femoral cortex
- Posterior femoral cut - resects posterior condyles
- Anterior chamfer cut - transition slope
- Posterior chamfer cut - transition slope
These 4 cuts + the prior distal femoral cut create the 5-surfaced bone bed for the femoral component.
Avoid notching the anterior femoral cortex - this is a stress riser that predisposes to periprosthetic fracture.
STEP 7: Tibial Preparation
- Place the tibial template on the cut surface - size to match the cortex without overhang (pain) or underhang (instability)
- Set rotational alignment - aligned to the medial 1/3 of the tibial tubercle
- Cut the central keel/peg slot with a punch or oscillating saw to accept the tibial component
- Internal rotation of the tibial tray → lateralizes tibial tubercle → increases Q-angle → lateral patellar subluxation (avoid this)
STEP 8: Patellar Resurfacing (If Performed)
- Measure native patellar thickness with calipers
- Make a flat resection removing the articular surface (typically 8-10 mm)
- Minimum residual bone: 12-15 mm (to prevent patellar fracture)
- Place the polyethylene patellar button - medialized, not centered (centering increases the Q-angle)
- Final patellar thickness = bone + implant should equal original patellar thickness
STEP 9: Trial Reduction and Gap Balancing
Insert trial components (no cement) to verify:
The Two Gaps
| Gap | Position | What it means |
|---|---|---|
| Extension gap | Knee in full extension | Distance between distal femoral and proximal tibial cuts |
| Flexion gap | Knee at 90 degrees | Distance between posterior femoral and proximal tibial cuts |
Goal: Both gaps must be equal AND rectangular (not trapezoidal).
Gap Problem Troubleshooting
| Problem | Cause | Solution |
|---|---|---|
| Flexion gap > Extension gap | Excessive posterior femoral resection OR tight PCL | Downsize femoral component (anterior reference); PCL release/recession |
| Extension gap > Flexion gap | Excessive distal femoral resection | Use thicker tibial insert; check posterior capsule release |
| Both gaps too small | Insufficient bone removal | Remove more tibial bone (affects both equally) |
| Both gaps equal but lax | Too much bone removed | Use thicker polyethylene insert |
Soft Tissue Balancing: Varus Knee (Most Common - ~70% of TKRs)
Medial structures are contracted. Release in stepwise sequence (only release what is needed):
- Deep MCL off the tibia (done during exposure)
- Posteromedial capsule
- Semimembranosus insertion
- Posterior oblique ligament
- Superficial MCL
- Pes anserinus (rarely needed)
Soft Tissue Balancing: Valgus Knee
Lateral structures are contracted. Release stepwise:
- Posterolateral capsule
- Pie-crusting of the ITB - multiple small punctures (preferred over complete release)
- Popliteus tendon (increases flexion gap > extension gap laterally)
- Posterior capsule off lateral femoral condyle
- Lateral head of gastrocnemius
- If still unbalanced: MCL advancement on the medial side
Peroneal nerve warning: Acute correction of severe combined valgus + flexion contracture can stretch the common peroneal nerve. If nerve palsy develops postoperatively, flex the knee to relieve traction.
Patellar Tracking - "No Thumb" Test
- Take the knee through full range of motion with trial components in place
- Release the patella - it should track centrally in the trochlear groove without being held
- Lateral tracking → consider:
- Lateral retinacular release
- Check femoral and tibial component rotation (internal rotation is the most common cause)
STEP 10: Cementation and Final Implantation
Preparation
- Irrigate copiously and thoroughly dry all cut bone surfaces - bone must be dry for cement to bond
- Use a pulsatile lavage system
Cementing Sequence (Tibia First)
| Order | Component | Key Points |
|---|---|---|
| 1st | Tibial tray | Apply cement to bone surface; seat firmly; confirm rotation; remove all excess cement |
| 2nd | Femoral component | Apply cement to bone surface; seat firmly with femoral impactor; remove posterior cement carefully |
| 3rd | Patellar button | Cement to resected patellar surface |
| 4th | Extend knee | With trial spacer in place to ensure complete femoral seating; spacer must be thick enough to hold extension (thin spacer → posterior tibial liftoff) |
Remove ALL bone and cement debris before inserting the final polyethylene - third-body debris causes accelerated wear.
Cementless Fixation (Alternative)
- More demanding bone cuts - no cement to compensate for gaps
- Bone-prosthesis gap >0.5 mm fills with fibrous tissue, not bone ingrowth
- Press-fit pegs and screws are essential for initial stability
- Test the tibial tray: press on the periphery - any rocking motion = revise the surface
Final Polyethylene Insert
- Snap/lock the tibial poly insert into the tibial tray
- Confirm it locks securely and does not toggle
STEP 11: Wound Closure
- Release the tourniquet - pack with moist sponges; allow hemostasis
- Identify and cauterize bleeding geniculate arteries (medial and lateral)
- Drains - no longer routinely recommended; no proven benefit; drained patients receive more blood transfusions
- Close the quadriceps mechanism/retinaculum with strong interrupted/continuous absorbable sutures
- Close subcutaneous tissue
- Close skin with staples or sutures
- Compression dressing applied
Complete Surgical Sequence at a Glance
SETUP: Supine, tourniquet, 90° knee flexion possible
↓
STEP 1: Anterior midline skin incision (knee in flexion)
↓
STEP 2: Medial parapatellar arthrotomy → patellar eversion
↓
STEP 3: ACL excision, anterior meniscectomy, osteophyte removal
↓
STEP 4: TIBIAL CUT → perpendicular to tibial axis, 3-5° posterior slope
↓
STEP 5: DISTAL FEMORAL CUT → 5-7° valgus, IM rod alignment
↓
STEP 6: FEMORAL SIZING + ROTATION → TEA / Whiteside's axis
→ Four-in-one cuts (anterior, posterior, chamfers)
↓
STEP 7: TIBIAL PREPARATION → size, rotation, keel slot
↓
STEP 8: PATELLAR RESURFACING (if performed)
↓
STEP 9: TRIAL REDUCTION
→ Check extension gap = flexion gap (rectangular)
→ Ligament balancing (varus = medial release / valgus = lateral pie-crust)
→ "No thumb" patellar tracking test
↓
STEP 10: CEMENTATION → tibia first → femur → patella
→ Final poly insert locked in
↓
STEP 11: TOURNIQUET DOWN → hemostasis → layered wound closure
Key Numbers to Memorize
| Parameter | Value |
|---|---|
| Valgus correction angle (distal femoral cut) | 5-7 degrees |
| Posterior tibial slope | 3-5 degrees |
| Femoral rotation off posterior condyles | 3 degrees external rotation |
| Maximum joint line elevation | 4 mm |
| Minimum residual patellar bone | 12-15 mm |
| PCL: switch to PS design if released | >75% released |
| Max bone-prosthesis gap for ingrowth | <0.5 mm |
| Safe VMO split zone (midvastus) | 4.5 cm from patella |
Source: Campbell's Operative Orthopaedics, 15th Ed. 2026, Chapter 8 (Techniques 8.1-8.9)
Everything about types and details about non union
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
Communication skills in clinical practice - anesthesiology
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.