Pulmonary edema
Reading File
Finding Sources
Searching PubMed
"pulmonary edema"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive, multi-source content to compile a thorough answer. Here is the full synthesis:
Pulmonary Edema
Pulmonary edema is a condition in which excess fluid accumulates in the extravascular spaces of the lung - first in the interstitium, then in the alveoli - impairing gas exchange and, if severe and acute, causing death within minutes to hours.
Pathophysiology
Fluid movement across pulmonary capillaries is governed by the Starling equation:
Q = K × [(Pc' - Pi) - σ(πc' - πi)]
Where Q = net flow; Pc' = capillary hydrostatic pressure (normally 7 mmHg); Pi = interstitial hydrostatic pressure (normally -4 to -8 mmHg); πc' = plasma oncotic pressure (~28 mmHg); πi = interstitial oncotic pressure (~14 mmHg); K = filtration coefficient; σ = reflection coefficient for albumin.
Under normal conditions, the small amount of fluid (~10-20 mL/hour) that leaks from capillaries is rapidly removed by pulmonary lymphatics. Edema develops when this lymphatic reserve is overwhelmed. - Morgan & Mikhail's Clinical Anesthesiology
Safety factor: Pulmonary capillary pressure must rise to at least equal plasma colloid osmotic pressure (~28 mmHg) before significant edema develops. This provides an acute safety margin of ~21 mmHg above the normal capillary pressure of 7 mmHg. In chronic conditions (e.g., mitral stenosis), lymphatic vessels expand up to 10-fold, allowing capillary pressures of 40-45 mmHg without lethal edema. In acute decompensation, pressures of 50 mmHg can be fatal within 30 minutes. - Guyton & Hall Textbook of Medical Physiology
Classification and Causes
1. Cardiogenic (Hemodynamic) Pulmonary Edema
Caused by elevated pulmonary capillary hydrostatic pressure (PCWP >18 mmHg). The resulting edema fluid has low protein content (transudate).
| Category | Examples |
|---|---|
| Increased hydrostatic pressure | Left heart failure (most common), mitral stenosis/regurgitation, volume overload, pulmonary vein obstruction |
| Decreased oncotic pressure | Hypoalbuminemia, nephrotic syndrome, liver disease, protein-losing enteropathy |
| Lymphatic obstruction | Rare; lymphangitis carcinomatosa |
Pathologically: alveolar capillary engorgement, intraalveolar transudate (finely granular pale pink material on histology), alveolar microhemorrhages. Chronically: hemosiderin-laden macrophages ("heart failure cells"), fibrosis and brown induration. - Robbins & Cotran Pathologic Basis of Disease
2. Noncardiogenic (Increased Permeability) Pulmonary Edema
Caused by injury to the alveolar-capillary membrane. PCWP is typically normal. The edema fluid has high protein content (exudate). The extreme form is ARDS.
| Category | Examples |
|---|---|
| Direct lung injury | Pneumonia (bacterial/viral), aspirated gastric contents, inhaled toxins (chlorine, SO₂, high-concentration O₂, smoke), radiation, near-drowning, lung trauma |
| Indirect (systemic) injury | Sepsis, severe burns, pancreatitis, polytrauma, transfusion-related (TRALI), chemotherapy (bleomycin), heroin, cocaine, methadone, paraquat |
| Undetermined origin | High-altitude pulmonary edema (HAPE), neurogenic (CNS trauma), negative-pressure (post-obstruction), re-expansion edema |
Robbins & Cotran; Morgan & Mikhail; Fishman's Pulmonary Diseases
Flash Pulmonary Edema
A specific variant in which alveolar edema develops so rapidly that there is no time for prior interstitial edema to manifest radiographically. It occurs with sudden changes in intravascular volume (trauma resuscitation) or sudden cardiac events (acute MI, arrhythmia). The PCWP may have normalized by the time the patient is catheterized, even though the edema was originally hydrostatic in origin. - Fishman's Pulmonary Diseases; Morgan & Mikhail
Clinical Presentation
Acute pulmonary edema typically presents with:
- Sudden onset severe dyspnea at rest, orthopnea, paroxysmal nocturnal dyspnea
- Tachypnea and tachycardia
- Severe hypoxemia (SaO₂ often <90%)
- Audible crackles (alveolar flooding) and wheezing (peribronchial cuffing - "cardiac asthma")
- Hypertension - due to endogenous catecholamine release
- Pink, frothy sputum in severe cases
- Anxiety, diaphoresis, cyanosis
Physical exam findings (crackles, peripheral edema) correlate poorly with the degree of interstitial edema, especially in CKD patients. - Harrison's Principles of Internal Medicine 22e; Murray & Nadel's
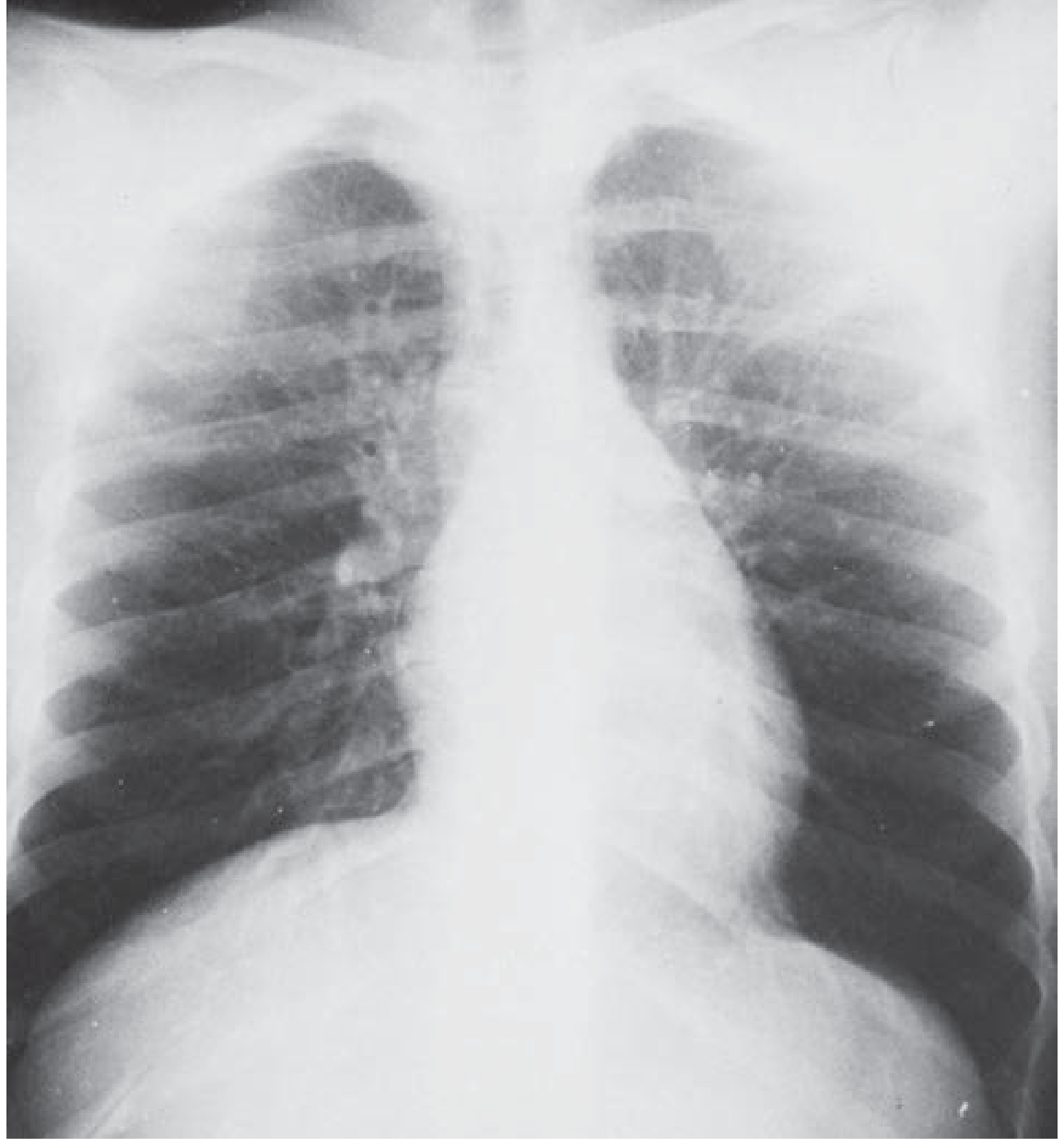
Imaging
Chest X-ray findings by stage:
| Stage | CXR Findings |
|---|---|
| Interstitial edema | Kerley B lines, peribronchial cuffing, vascular redistribution (cephalization), haziness of hilar vessels |
| Alveolar edema | Bilateral airspace opacities (ground-glass or consolidation), symmetric, central/"bat-wing" distribution, lower lung field predominant |
| Associated | Cardiomegaly, pleural effusions |

Lung ultrasound: B-lines (vertical artifacts arising from the pleural line) reflect extravascular lung water and have high sensitivity for pulmonary edema - often superior to CXR, particularly in CKD. Combined with echocardiography, it helps differentiate cardiogenic from noncardiogenic edema. Recent 2025 meta-analysis (PMID: 40334938) confirmed B-line quantification predicts cardiovascular events in acute heart failure. - Fishman's; Murray & Nadel's
Distinguishing Cardiogenic vs. Noncardiogenic
| Feature | Cardiogenic | Noncardiogenic |
|---|---|---|
| PCWP | >18 mmHg | ≤18 mmHg |
| Edema fluid protein | Low (transudate) | High (exudate) |
| BNP/NT-proBNP | Markedly elevated | Normal or mildly elevated |
| Echocardiogram | LV systolic/diastolic dysfunction, valvular disease | Relatively preserved LV function |
| Resolution | Faster (responds to diuretics/nitrates) | Slower; often requires mechanical ventilation |
| CXR | Cardiomegaly, vascular redistribution | Heart size often normal |
ECG should be checked urgently - ST elevation/Q waves indicate acute MI requiring immediate revascularization. - Harrison's 22e
Treatment
Treatment depends on etiology, but several immediate measures apply broadly.
1. Positioning
- Sit the patient upright, legs dangling - reduces venous return and preload
2. Oxygenation & Ventilation
- Target SaO₂ ≥ 92% (avoid hyperoxia >98%)
- High-flow nasal cannula (HFNC): preferred for acute hypoxemic respiratory failure with normal PaCO₂
- NIV (CPAP/BiPAP): useful adjunct; reduces work of breathing, improves oxygenation, decreases need for intubation; beneficial effect on cardiogenic edema is widely accepted
- Invasive mechanical ventilation with PEEP: indicated when NIV fails; PEEP (1) reduces preload and afterload, (2) redistributes lung water from intra-alveolar to extraalveolar space, (3) prevents atelectasis
3. Reduction of Preload
| Agent | Dose | Notes |
|---|---|---|
| Furosemide (1st line) | ≤0.5 mg/kg IV (1 mg/kg if renal insufficiency or diuretic resistance) | Also a venodilator; acts before diuresis begins |
| Sublingual nitroglycerin | 0.4 mg × 3 every 5 min | First-line for acute cardiogenic PE; rapid preload reduction |
| IV nitroglycerin | 5-10 µg/min, titrate up | If SL NTG insufficient and BP allows |
| IV nitroprusside | 0.1-5 µg/kg/min | Potent venous + arterial vasodilator; use with continuous arterial BP monitoring; avoid in low coronary perfusion states |
| Morphine | 2-4 mg IV bolus | Transient vasodilator; reduces dyspnea/anxiety; use with caution - registry data showed increased mortality |
| ACE inhibitors | Low dose, short-acting | Reduce preload + afterload; reduce mortality in MI with HF |
| Nesiritide (BNP) | IV infusion | Potent arterio-venous vasodilator; reserve for refractory cases; avoid in ischemia/MI |
4. Inotropic Support (when cardiogenic shock accompanies edema)
- Dobutamine, dopamine: sympathomimetic inotropes
- Milrinone (PDE-3 inhibitor): inotrope + vasodilator; 50 µg/kg bolus then 0.25-0.75 µg/kg/min
5. Renal Replacement Therapy
- Indicated for refractory volume overload with metabolic acidosis (pH <7.15-7.25), persistent hyperkalemia, or hypoxemia
- In ESRD patients: hemodialysis is the definitive treatment; dialysis peritoneal does not remove volume fast enough for acute PE; aggressive medical therapy is unlikely to suffice without dialysis
6. Treat the Underlying Cause
- Acute MI - urgent revascularization (PCI)
- Arrhythmia - cardioversion or rate control
- Hypertensive crisis - IV antihypertensives
- HAPE - oxygen + descent to lower altitude (nifedipine as adjunct; nitrates/furosemide are NOT indicated)
- Infection/sepsis - antibiotics, source control
Harrison's Principles of Internal Medicine 22e; Morgan & Mikhail's Clinical Anesthesiology; Rosen's Emergency Medicine; Tintinalli's Emergency Medicine; Katzung's Pharmacology
Special Considerations
Chronic Kidney Disease / ESRD
Pulmonary edema in CKD is often multifactorial: elevated hydrostatic pressure (fluid overload/CHF) + reduced oncotic pressure (hypoalbuminemia) + increased capillary permeability (uremia). Physical signs and even CXR findings may be misleading; lung ultrasound is more sensitive. Uremic cardiomyopathy with LV dysfunction may be partially reversible with dialysis or transplantation. - Murray & Nadel's
High-Altitude Pulmonary Edema (HAPE)
A noncardiogenic edema; first-line treatment is descent + oxygen. Nifedipine can be used as an adjunct to reduce pulmonary arterial pressure. Unlike cardiogenic PE, nitroglycerin and furosemide are not appropriate as primary treatment. - Rosen's Emergency Medicine
Negative-Pressure (Post-Obstructive) Pulmonary Edema
Occurs after sudden relief of upper airway obstruction. The large negative intrathoracic pressure generated against a closed glottis draws fluid into alveoli. Common after laryngospasm. Treatment is generally supportive with oxygen and NIV; most resolve quickly. - Morgan & Mikhail's
Summary
| Aspect | Key Point |
|---|---|
| Mechanism | Starling forces imbalance (↑Pc' or ↑permeability) overwhelms lymphatic clearance |
| #1 cause | Left-sided heart failure (cardiogenic) |
| PCWP cutoff | >18 mmHg = cardiogenic |
| Immediate therapy | Sit upright, O₂/HFNC/NIV, SL nitroglycerin, IV furosemide |
| Do NOT give furosemide in | HAPE, neurogenic PE (not appropriate etiology) |
| Morphine caution | Registry data suggests possible harm |
| ESRD | Dialysis is definitive; aggressive medical Rx is a bridge only |
| Lethal course | Capillary pressure 25-30 mmHg above safety factor → death in <30 min |
This is a shared conversation. Sign in to Orris to start your own chat.