Ventilator modes detailed information
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have all the information needed for a comprehensive, detailed response. Let me compile it.
Ventilator Modes - Detailed Information
Foundational Concepts
Before discussing individual modes, understanding three defining variables is necessary: control variable, breath sequence, and targeting scheme. - Morgan and Mikhail's Clinical Anesthesiology, 7e
1. Control Variable
The control variable is the independent variable the ventilator directly manages:
| Control Variable | What is Fixed | What Varies |
|---|---|---|
| Volume Control (VCV) | Tidal volume (VT) and flow | Airway pressure |
| Pressure Control (PCV) | Inspiratory pressure | Tidal volume and flow |
| Flow Control | Rarely used clinically; flow is derivative of volume | - |
2. Breath Sequence
Defines the pattern of mandatory vs. spontaneous breaths:
| Sequence | Description |
|---|---|
| CMV (Continuous Mandatory Ventilation) | All breaths are mandatory, including any patient efforts |
| IMV (Intermittent Mandatory Ventilation) | Mandatory breaths interspersed with spontaneous ones |
| CSV (Continuous Spontaneous Ventilation) | All breaths are spontaneous; patient controls timing and size |
Combining control variables and breath sequences gives 5 practical breathing patterns: VC-CMV, VC-IMV, PC-CMV, PC-IMV, PC-CSV.
3. Targeting Scheme
The feedback control system used to reach a set value. The most basic type is set-point targeting - the clinician sets a value (e.g., VT and flow for VCV; inspiratory pressure and time for PCV) and the ventilator seeks to deliver it.
Individual Ventilator Modes
A. Controlled Mandatory Ventilation (CMV) - VC-CMV Pattern
- The ventilator cycles at a fixed time interval to deliver a preset VT at a preset rate
- Minute ventilation is completely fixed regardless of patient effort
- Patients cannot breathe spontaneously; awake patients require sedation ± neuromuscular blockade
- Settings limit inspiratory pressure to guard against barotrauma
Best for: Deeply sedated/paralyzed patients; patients with no spontaneous respiratory drive
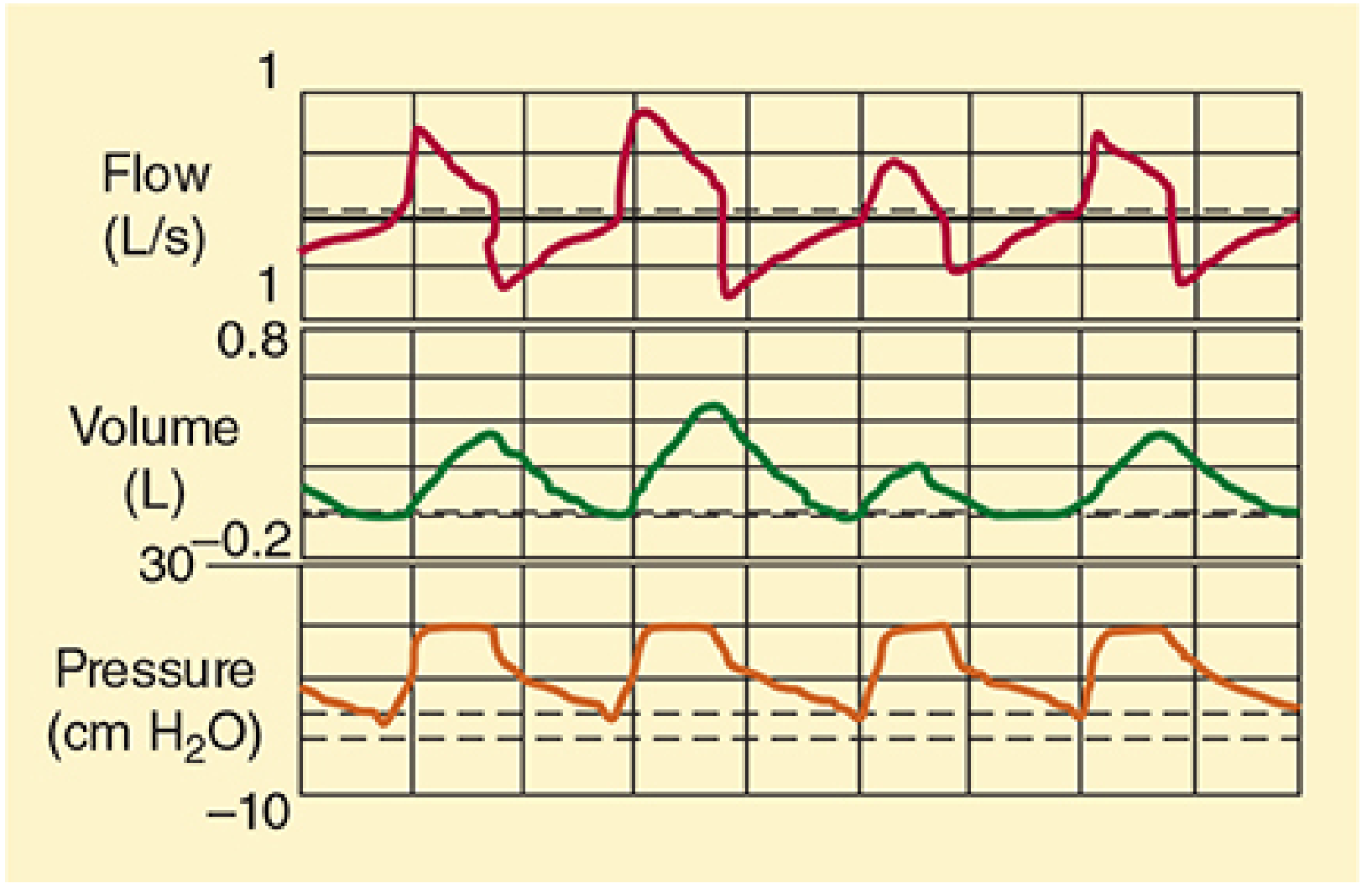
B. Assist-Control Ventilation (AC / A-C) - VC-CMV or PC-CMV Pattern
- A pressure sensor detects patient inspiratory effort and triggers a full preset breath
- A sensitivity control determines the effort threshold required to trigger
- If no effort is detected, the machine delivers breaths at the set backup rate (functions as CMV)
- Can be volume-controlled (AC/VC) or pressure-controlled (AC/PC)
Key clinical point: In AC mode, every patient-triggered breath delivers a full-sized breath regardless of inspiratory effort magnitude. This can cause hyperventilation, air trapping, hypotension, and poor synchrony if the patient is breathing spontaneously. Adequate sedation is therefore important. - Rosen's Emergency Medicine, 10e
Parameters set by clinician (AC/VC): Tidal volume, inspiratory flow, PEEP, respiratory rate
Parameters set by clinician (AC/PC): Target pressure, inspiratory time, PEEP, respiratory rate
Best for: Initial mode of choice in paralyzed/deeply sedated ED/ICU patients
C. Synchronized Intermittent Mandatory Ventilation (SIMV) - VC-IMV or PC-IMV Pattern
- Delivers mandatory breaths at a preset rate, synchronized to coincide with spontaneous inspiratory effort
- Between mandatory breaths, the patient breathes spontaneously without machine assistance
- Synchronization prevents "breath stacking" (delivering a mandatory breath mid-spontaneous breath)
- SIMV rate can be adjusted: high rates (10-12/min) = nearly full support; low rates (1-2/min) = near-independent breathing
Difference from CMV: Patient breathes spontaneously between machine breaths
Difference from IMV: Breaths are synchronized; pure IMV does not time the mandatory breath to patient effort
Weaning: Classic weaning tool - progressively lower the mandatory rate to increase spontaneous workload
Caveat: If rate is too low (e.g., 4/min), weak patients may fatigue from the work of breathing during spontaneous efforts, especially when endotracheal tube resistance is present. Adding pressure support to SIMV offsets this added work.
Parameters: Pressure or volume control, PEEP, backup RR
Best for: Patients with regular but poor spontaneous respiratory effort; weaning
D. Pressure Support Ventilation (PSV) - PC-CSV Pattern
- The ventilator delivers a preset positive pressure with every inspiratory effort
- Is flow-cycled: when inspiratory flow decreases to ~25% of peak flow, the machine cycles to expiration (no fixed inspiratory time)
- Patient controls respiratory rate; VT varies based on lung mechanics, flow, and patient effort
Levels of support:
- Low PSV (5-10 cm H₂O): Overcomes added resistance of endotracheal tube, breathing circuit, and ventilator valves
- High PSV (10-40 cm H₂O): Standalone ventilatory mode for patients with sufficient drive and stable lung mechanics
Advantages:
- Augments spontaneous VT
- Decreases work of breathing (WOB)
- Increases patient comfort
- Patient-initiated (good synchrony)
Disadvantages/Risks:
- No backup rate - if patient fatigues or opioids suppress drive, VT becomes inadequate
- VT not guaranteed; changes in lung mechanics alter delivered volume
Parameters set: Level of pressure support, PEEP
Best for: Spontaneously breathing patients requiring minimal support; weaning; intubated asthmatics
E. Continuous Positive Airway Pressure (CPAP) - CSV Pattern
- Provides a constant elevated baseline pressure throughout both inspiration and expiration
- Patient breathes entirely spontaneously; no mandatory or augmented breaths
- Prevents alveolar collapse, improves V/Q matching, reduces WOB
Parameters: Level of CPAP
Best for: Alert, spontaneously breathing patients with immediately reversible respiratory distress; non-invasive ventilation in COPD exacerbations, acute cardiogenic pulmonary edema (ACPE)
F. BiPAP (Bi-Level Positive Airway Pressure)
- Delivers two pressure levels: IPAP (higher, during inspiration) and EPAP (lower, during expiration)
- Similar indication profile to CPAP but provides additional inspiratory pressure support
- Primarily used as non-invasive ventilation (NIV)
Parameters: IPAP and EPAP
Best for: Similar to CPAP; COPD exacerbations, hypercapnic respiratory failure, obesity hypoventilation
G. Pressure-Controlled Ventilation (PCV) - PC-CMV or PC-IMV Pattern
- Sets a fixed inspiratory pressure; tidal volume is variable (depends on compliance and resistance)
- Breaths are time-cycled and time-triggered
- Longer inspiratory times allow better mixing and recruitment of collapsed alveoli when combined with adequate PEEP
Advantages:
- Limits peak airway pressure → reduces risk of barotrauma and volutrauma
- Decelerating flow pattern may improve gas distribution
Disadvantages:
- VT is not guaranteed - if compliance decreases (e.g., worsening ARDS), adequate VT may not be attained without increasing the pressure limit
- In asthmatics, changing airway resistance can cause dangerously variable tidal volumes
Comparison with PSV: PCV also controls peak airway pressure, but has a mandatory rate and set inspiratory time (not flow-cycled). The ventilator does not cycle to expiration until the preset inspiratory time elapses.
H. Inverse I:E Ratio Ventilation (IRV) - PC-IMV Pattern
Normal I:E ratio is 1:3 or greater; IRV reverses this to >1:1 (e.g., 1.5:1 or 2:1)
Methods to achieve IRV:
- Adding an end-inspiratory pause
- Decreasing peak inspiratory flow in VCV
- Setting a long inspiratory time in PCV (PC-IRV)
Effect: Incomplete exhalation → air trapping → intrinsic PEEP (auto-PEEP) → increased FRC
Purpose: Improves oxygenation in patients with reduced FRC (e.g., ARDS)
Downside: Does not allow spontaneous breathing - requires heavy sedation or neuromuscular blockade
I. Airway Pressure Release Ventilation (APRV) - PC-IMV Pattern
APRV (also called bilevel ventilation) maintains a high baseline PEEP while allowing spontaneous breathing, with intermittent brief pressure releases to augment CO₂ elimination.
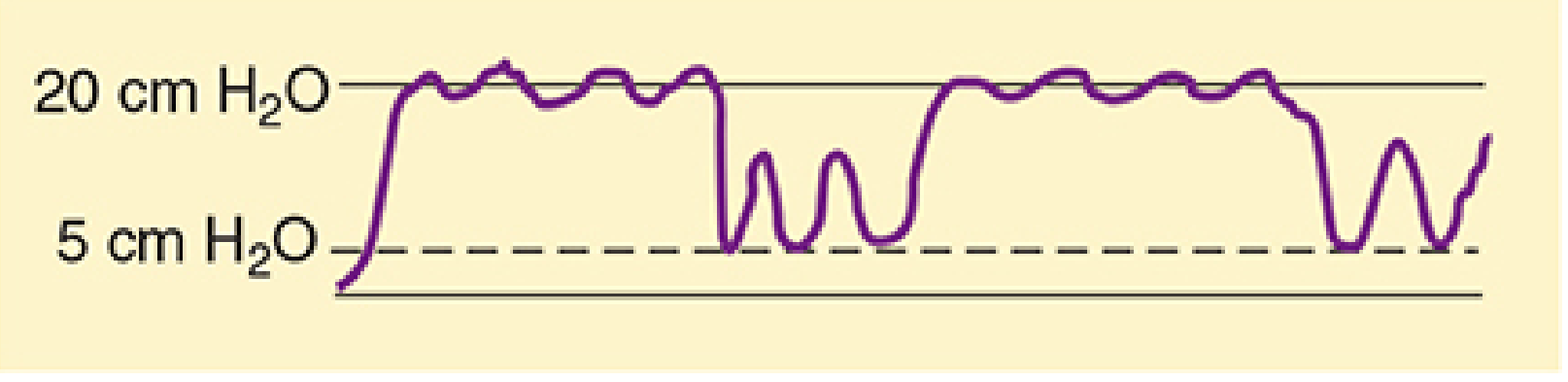
Typical initial settings:
- P-high (minimum PEEP): 10-12 cm H₂O
- P-low (release level): 5-10 cm H₂O
- Release frequency: 10-12/min
- T-low: set to allow only 50-70% of expiratory flow (generates auto-PEEP)
Determinants of minute ventilation: Inspiratory time, expiratory time, high and low PEEP levels, spontaneous respiratory activity
Advantages over PC-IRV:
- Allows spontaneous breathing → less sedation needed
- Less circulatory depression
- Less pulmonary barotrauma
- Attractive alternative for patients with high peak pressures from reduced compliance
Used in: ARDS and refractory hypoxemia as an alternative to conventional PCV-IRV
J. High-Frequency Ventilation (HFV)
Three subtypes, all delivering VT at or below anatomic dead space:
| Type | Rate | Mechanism |
|---|---|---|
| High-Frequency Positive Pressure Ventilation (HFPPV) | 60-120 breaths/min | Small conventional VT at high rate |
| High-Frequency Jet Ventilation (HFJV) | 120-600 times/min (2-10 Hz) | Pulsed jet of high-pressure gas via small cannula; may entrain air (Bernoulli effect) |
| High-Frequency Oscillation (HFO) | 180-3000 times/min (3-50 Hz) | Piston creates to-and-fro gas movement |
Gas exchange mechanism: Exact mechanism unclear; likely a combination of effects including asymmetric velocity profiles, molecular diffusion, and cardiogenic mixing.
Initial HFJV settings: Rate 120-240/min; inspiratory time 33%; drive pressure 15-30 psi
Clinical uses:
- HFJV: Laryngeal, tracheal, bronchial surgical procedures; bronchopleural fistulas; tracheoesophageal fistulas
- HFO: ARDS (to improve oxygenation)
CO₂ elimination: Increased by increasing drive pressure
Oxygenation: Related to mean airway pressure
K. Differential (Independent) Lung Ventilation
- Uses a double-lumen endotracheal tube to ventilate each lung independently via two separate ventilators
- One ventilator acts as "master" (sets rate), the other as "slave" (synchronized to master)
Indications:
- Severe unilateral lung disease
- Bronchopleural fistula
- Situations where conventional PEEP would cause overdistention of the healthy lung
Summary Table: Ventilator Mode Selection
| Mode | Breath Type | Control | Patient Effort Required | Key Use |
|---|---|---|---|---|
| CMV | All mandatory | Volume or Pressure | None | Paralyzed/no drive |
| AC (Assist-Control) | Mandatory (triggered or timed) | Volume or Pressure | Optional (triggers breath) | Initial mode; sedated/paralyzed |
| SIMV | Mandatory + Spontaneous | Volume or Pressure | Yes (spontaneous between mandatory) | Weaning, partial support |
| PSV | All spontaneous (augmented) | Pressure | Yes (triggers and cycles each breath) | Weaning, minimal support |
| CPAP | All spontaneous (no augmentation) | Pressure (baseline only) | Yes (full breathing work) | NIV, alert patients |
| BiPAP | All spontaneous (augmented) | Dual pressure (IPAP/EPAP) | Yes | NIV, COPD, hypercapnia |
| PCV | Mandatory (time-triggered) | Pressure | None (mandatory) | Lung protective, ARDS |
| IRV | Mandatory | Pressure (long I-time) | None (requires sedation/paralysis) | ARDS, refractory hypoxemia |
| APRV | Mandatory + Spontaneous | Dual pressure | Yes (spontaneous allowed) | ARDS, avoids barotrauma |
| HFV | Mandatory (very high rate) | Pressure/Flow | None | Airway surgery, fistulas |
Initial Ventilator Settings (Standard ICU Patient)
From - Roberts and Hedges' Clinical Procedures in Emergency Medicine:
- Mode: AC (volume control) preferred for initial settings
- Tidal Volume (VT): 6-8 mL/kg ideal body weight (IBW) - lung protective
- Respiratory Rate: 12-16 breaths/min
- PEEP: Start at 5 cm H₂O, titrate up to improve oxygenation and prevent atelectotrauma
- FiO₂: Start at 1.0 (100%); wean to maintain SpO₂ >90%, PaO₂ >60 mmHg; target FiO₂ <0.4 to prevent O₂ toxicity
Key Mechanics: Cycling (Inspiration → Expiration)
| Cycling Mechanism | Trigger for End-Inspiration | Used In |
|---|---|---|
| Volume-cycled | Preset VT delivered | Most adult ICU ventilators (CMV, AC) |
| Pressure-cycled | Preset pressure reached | Less common now |
| Time-cycled | Preset inspiratory time elapses | PCV, neonates, OR ventilators |
| Flow-cycled | Flow drops to ~25% of peak | PSV |
Sources: Morgan and Mikhail's Clinical Anesthesiology, 7e | Rosen's Emergency Medicine, 10e | Mulholland and Greenfield's Surgery, 7e | Miller's Anesthesia, 10e
How to reduce depression suffering from 2 years
Reading File
Finding Sources
Finding Sources
Searching PubMed
"major depressive disorder"[MeSH Terms] AND "treatment"[MeSH Terms]
Reading File
Reading File
Searching PubMed
"depression" AND "psychotherapy" AND "antidepressant"
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
I now have comprehensive, authoritative content to give a thorough and compassionate answer.
Reducing Depression - A Comprehensive Guide
A note first: Two years is a long time to be suffering. What you're experiencing is a recognized medical condition, not a character flaw or weakness - and it responds to treatment. Everything below is based on current clinical guidelines and textbook psychiatry. Please use this as a starting point to work with a doctor or mental health professional, not as a substitute for one.
Understanding What You're Dealing With
Depression lasting 2 years or more is called Persistent Depressive Disorder (Dysthymia) if it has been at a lower level of severity throughout, or it may be recurrent or chronic Major Depressive Disorder (MDD) if you have had one or more significant episodes. Both are serious, both respond to treatment, and both benefit from a combination of approaches.
Depression severity is categorized as:
- Less severe (mild/subthreshold): significant distress but functional
- More severe (moderate to severe): major impact on daily life, relationships, work
The treatment plan differs based on severity. - Maudsley Prescribing Guidelines in Psychiatry, 15e
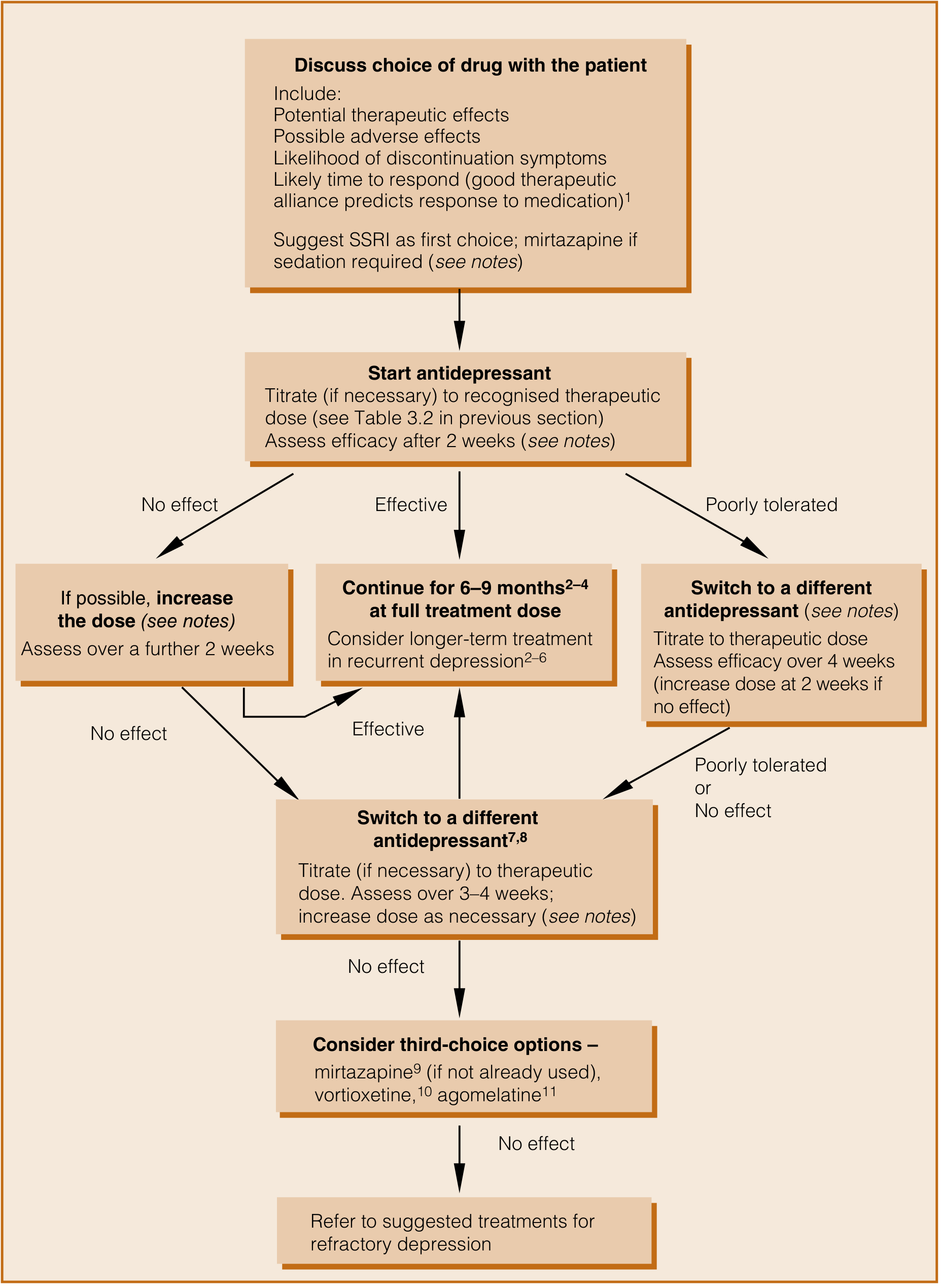
The Treatment Decision Flowchart
Pillar 1: Psychological Therapies (Psychotherapy)
For less severe depression, psychological treatments are the first-line recommendation before medication. Even in more severe depression, combining therapy with medication is more effective than either alone.
| Therapy | What It Does | Evidence |
|---|---|---|
| Cognitive Behavioral Therapy (CBT) | Identifies and changes negative thought patterns and behaviors | Strong; most evidence of all psychotherapies |
| Behavioral Activation | Gradually re-engages with rewarding activities to break the cycle of withdrawal | Strong; particularly useful early |
| Interpersonal Therapy (IPT) | Addresses relationship problems, grief, and role transitions | Good, especially if interpersonal conflict is a trigger |
| Mindfulness-Based Cognitive Therapy (MBCT) | Prevents relapse by building awareness of thought patterns | Strong evidence for relapse prevention |
| Short-term Psychodynamic Therapy | Explores underlying emotional conflicts | Good for complex/chronic depression |
| Guided Self-Help / Counselling | Structured self-management with therapist input | Useful for milder cases |
Practical message: If you have been depressed for 2 years, CBT is the most evidence-backed non-drug treatment you can access. It produces changes that last beyond the end of therapy.
Pillar 2: Antidepressant Medication
Antidepressants are recommended for moderate to severe depression and for dysthymia. About 50% of people respond to their first antidepressant. - Maudsley Prescribing Guidelines, 15e
First-Line: SSRIs (Selective Serotonin Reuptake Inhibitors)
NICE guidelines and most international bodies recommend starting with a generic SSRI.
Common SSRIs and their typical doses:
| Drug | Starting Dose | Usual Therapeutic Dose | Notes |
|---|---|---|---|
| Sertraline | 50 mg/day | 50-200 mg/day | Most commonly used first-line globally |
| Escitalopram | 10 mg/day | 10-20 mg/day | Good tolerability; some dose-response benefit |
| Fluoxetine | 20 mg/day | 20-60 mg/day | Long half-life; fewer withdrawal symptoms |
| Citalopram | 20 mg/day | 20-40 mg/day | Well tolerated |
| Paroxetine | 20 mg/day | 20-50 mg/day | More sedating; harder to stop |
Important facts about SSRIs:
- Start low, titrate slowly - minimizes early side effects that cause people to stop
- Full therapeutic effect takes 4-6 weeks - do not give up before this
- If no improvement whatsoever by 2 weeks, early re-evaluation is warranted
- Only ~30% of those with no significant improvement at 2 weeks ultimately respond to that drug
- Continue at full therapeutic dose for 6-9 months after remission to prevent relapse
What If the First SSRI Doesn't Work?
A network meta-analysis of antidepressants found that drugs with dual action on both serotonin AND norepinephrine are among the most effective (SNRIs/dual-action agents). - Maudsley Prescribing Guidelines, 15e
Second-line options:
| Drug | Class | Notes |
|---|---|---|
| Venlafaxine (SNRI) | Serotonin + Norepinephrine | More effective at higher doses; dose-response relationship |
| Duloxetine (SNRI) | Serotonin + Norepinephrine | Also used for pain comorbidity |
| Mirtazapine | NaSSA | Sedating - useful if insomnia is a major symptom; often combined with SSRIs |
| Bupropion | NDRI | Good for fatigue, low energy; also helps if sexual side effects from SSRIs are a problem |
| Vortioxetine | Multimodal | Some cognitive benefits; strongest evidence for switching after one failed treatment |
Pillar 3: Augmentation Strategies (When Antidepressants Alone Are Insufficient)
If a single antidepressant provides only partial response after 2-4 weeks at therapeutic dose, augmentation (adding a second agent) is a widely-used strategy:
| Augmenting Agent | Evidence | Notes |
|---|---|---|
| Aripiprazole (2-20 mg/day) | Strong - supported by multiple meta-analyses | Low doses effective; good tolerability |
| Quetiapine | Strong | Also helps sleep; sedation can be advantageous |
| Lithium | Good, well established | Requires blood level monitoring; best for recurrent depression |
| Mirtazapine (added to SSRI) | Strong combination evidence (SSRI + mirtazapine = "California Rocket Fuel") | Dual mechanism; used when partial response |
| Thyroid hormone (T3) | Some evidence | Particularly useful if fatigue is dominant |
| Esketamine/Ketamine (nasal) | Emerging strong evidence | Licensed for treatment-resistant MDD; rapid onset (hours) |
Pillar 4: Lifestyle - The Most Underutilized Treatment
These are not "soft" options - each has robust biological mechanisms and clinical evidence:
Exercise
- One of the most evidence-backed interventions for mild-moderate depression
- Aerobic exercise (30 min, 3-5 times/week) is as effective as antidepressants in some mild-moderate depression studies
- Mechanism: increases BDNF, normalizes HPA axis, releases endorphins and endocannabinoids
- Start small - even a 10-minute daily walk is a meaningful beginning
Sleep
- Depression and poor sleep reinforce each other in a destructive cycle
- Maintaining a consistent sleep-wake time (even on weekends) is one of the most impactful changes you can make
- Avoid screens 1 hour before bed; avoid alcohol (disrupts REM sleep, worsens depression next day)
- Addressing insomnia directly - through CBT for insomnia (CBT-I) or short-term medication if needed - often improves depression substantially
Social Connection
- Isolation deepens depression; even brief social contact (a short walk with a friend, a phone call) activates reward circuits
- This is hard when depressed because the very symptom of depression is withdrawal - Behavioral Activation therapy is specifically designed to help you re-engage despite not "feeling like it"
Nutrition
- Mediterranean-style diet (vegetables, legumes, fish, olive oil, less processed food) is associated with lower rates of depression and better treatment outcomes
- Minimize alcohol - it is a CNS depressant and will worsen depression even though it briefly feels like relief
Sunlight / Light Therapy
- Bright light therapy (10,000 lux lamp, 30 min every morning) is proven for seasonal depression and has benefit in non-seasonal depression too
- Sunlight exposure during the day also regulates circadian rhythm and melatonin
Pillar 5: Neuromodulation - When Medication and Therapy Are Insufficient
For depression lasting 2+ years that hasn't responded to multiple treatments:
| Treatment | How It Works | Evidence |
|---|---|---|
| ECT (Electroconvulsive Therapy) | Brief electrical stimulation under anesthesia | Most effective treatment for severe/treatment-resistant depression; rapid onset; use when life is at risk or rapid response needed |
| rTMS (Repetitive Transcranial Magnetic Stimulation) | Magnetic pulses to prefrontal cortex | Non-invasive; good evidence; used when medications fail |
| VNS (Vagus Nerve Stimulation) | Implanted device stimulates vagal nerve | NICE-recommended for treatment-resistant depression |
| Esketamine (Spravato) nasal spray | NMDA receptor antagonism | Licensed for treatment-resistant MDD; effects felt in hours; supervised in clinic |
| Psilocybin-assisted therapy | Serotonergic psychedelic with therapy | Recent meta-analysis (BMJ 2024) shows significant efficacy; still emerging/research setting |
What to Do If You've Already Tried Antidepressants
Depression that has persisted for 2 years despite some treatment is called Treatment-Resistant Depression (TRD) if it has failed to respond to at least 2 adequate antidepressant trials. "Adequate" means:
- Full therapeutic dose
- At least 4-6 weeks at that dose
The most important next steps for TRD:
- Re-examine the diagnosis - rule out bipolar depression (which doesn't respond to standard antidepressants and can actually be worsened by them)
- Rule out physical causes - hypothyroidism, vitamin D deficiency, sleep apnea, anemia, chronic pain, inflammatory conditions
- Consider augmentation with aripiprazole, quetiapine, or lithium
- Try esketamine if available - it produces responses in days, not weeks
- Refer to a psychiatrist or specialist mood disorder clinic if not already under specialist care
Duration of Treatment
| Situation | Recommended Duration |
|---|---|
| First episode, responded to treatment | At least 6-9 months after remission |
| Two or more episodes (recurrent) | At least 2 years, often indefinite |
| Chronic/persistent depression | Long-term or indefinite treatment |
Stopping too early is the most common reason depression returns. - Maudsley Prescribing Guidelines, 15e
A Note on Hope
About 50% of people respond to their first antidepressant. If the first doesn't work, the chances of eventually achieving remission are still good - most people will find an effective treatment by working through a systematic, evidence-based approach. The fact that you've been suffering for 2 years is not a sign that your depression is untreatable - it may simply mean that you haven't yet found the right combination or haven't had access to the right care.
If you are having thoughts of harming yourself, please reach out to a crisis line immediately:
- International Association for Suicide Prevention: https://www.iasp.info/resources/Crisis_Centres/
- In most countries, calling emergency services (911/999/112) will connect you to mental health crisis support
Sources: Maudsley Prescribing Guidelines in Psychiatry, 15e | Kaplan & Sadock's Comprehensive Textbook of Psychiatry | NICE Guidelines on Depression | JAMA Psychiatry (2023) meta-analysis [PMID: 37672261] | BMJ psilocybin meta-analysis (2024) [PMID: 38692686]
This is a shared conversation. Sign in to Orris to start your own chat.