Kaplan vs kochers approach to elbow
Reading File
Finding Sources
Finding Sources
Searching the Web
Kaplan vs Kocher approach elbow surgical anatomy internervous plane
Reading File
Finding Sources
Reading Web Page
https://www.orthobullets.com/approaches/3068/elbow-kaplan-ap…
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive data from multiple authoritative sources. Here is the full comparison:
Kaplan vs Kocher Approach to the Elbow
Both are lateral approaches used to access the radiocapitellar joint, but they differ in their internervous plane, what they expose best, and the structures at risk.
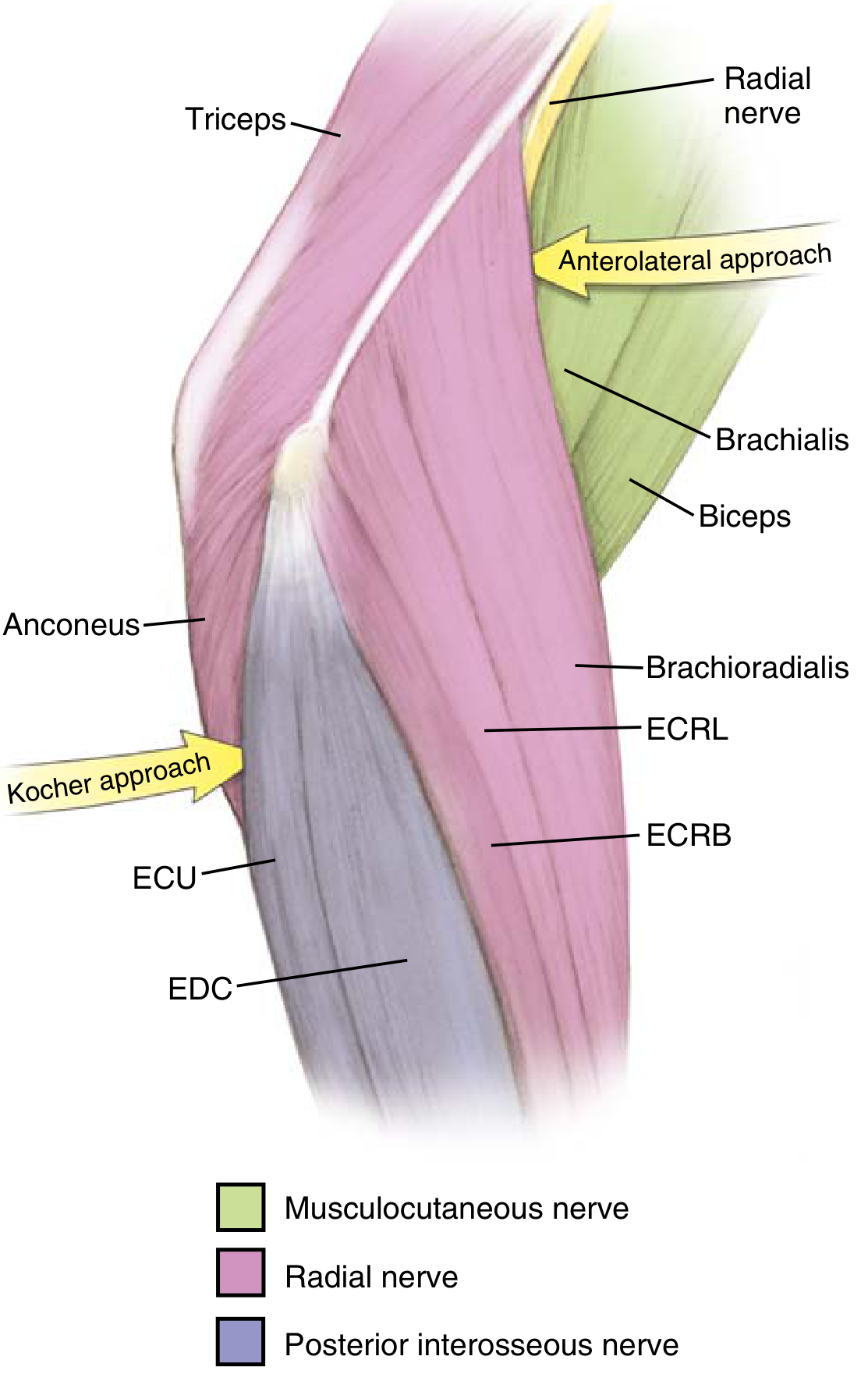
Internervous planes for lateral approaches to the elbow. The Kocher approach uses the anconeus (radial n.) / ECU (PIN) interval posteriorly. The Kaplan approach uses the ECRB (radial n./PIN) / EDC (PIN) interval, which is more anterior. (Miller's Review of Orthopaedics)
Side-by-Side Comparison
| Feature | Kaplan | Kocher |
|---|---|---|
| Position | More anterior (lateral) | More posterior (posterolateral) |
| Internervous plane | ECRB (radial n. / PIN) -- EDC (PIN) | Anconeus (radial n.) -- ECU (PIN) |
| Deep landmark | Supinator / annular ligament | Anconeus / LUCL / ECU |
| Forearm position | Pronation (moves PIN away) | Pronation (moves PIN away) |
| Primary nerve at risk | PIN (greater risk - more anterior) | PIN (lesser risk - ECU provides cover) |
| LCL complex risk | Lower (approach is anterior to LUCL) | Higher (Kocher passes close to LUCL) |
| Extensibility | Distal: Thompson approach (proximal forearm) | Distal: proximal forearm; Proximal: triceps/ECRL interval |
| Exposure | Anterior radial head, capitellum, coronoid (lateral), anterior capsule | Radial head, capitellum, posterior lateral column, LUCL |
Kaplan Approach (Lateral)
Interval: Between ECRB (radial nerve or PIN - variable, cadaveric study: 50% PIN / 35% superficial sensory / 15% radial nerve proper) and EDC (PIN). This is technically the same muscular interval used more distally by the Thompson approach.
Incision: 4 cm longitudinal from the tip of the lateral epicondyle toward Lister's tubercle.
Technique:
- Identify and bluntly develop ECRB / EDC interval
- Retract ECRB radially, EDC ulnarly
- Pronate forearm - this moves the PIN ~1 cm further from the radiocapitellar joint (supination brings it ~1 cm closer - dangerous)
- Detach humeral and ulnar heads of supinator to visualize the annular ligament and capsule
- Incise the lateral annular ligament and capsule anterior to the LUCL along the equator of the radiocapitellar joint
Indications:
- Radial head fractures (particularly anterior half involvement)
- Capitellum fractures
- Lateral humeral condyle fractures
- PIN decompression
- Proximal radius tumors
- Septic elbow irrigation/debridement
Dangers:
- PIN - highest risk of any lateral elbow approach due to the more anterior position
- Radial recurrent artery ("leash of Henry") - injury causes hematoma
- Lateral antebrachial cutaneous nerve (in subcutaneous fat distally)
- LCL access is limited - if the LUCL is traumatically disrupted, it is difficult to access and repair via Kaplan; you need to release EDC to visualize it
Key advantage: The more anterior trajectory keeps you away from the LUCL, so the ligament is preserved by default. Miller's notes: "split the annular ligament while remaining anterior to the LUCL."
Kocher Approach (Posterolateral)
Interval: Between anconeus (radial nerve) and ECU (PIN). The ECU muscle belly provides a natural shield over the PIN, making this approach somewhat safer for the nerve than Kaplan.
Incision: "J"-shaped - begins 5 cm proximal over the lateral supracondylar ridge, extends distally along the ridge, then curves medially/posteriorly to the posterior ulna border (Campbell's Operative Orthopaedics).
Technique:
- Identify the ECU / anconeus interval (a thin fat stripe or perforating branches of the posterior interosseous recurrent artery help locate it)
- Bluntly undermine the anconeus to identify the joint capsule and LUCL
- Elevate some common extensor tendon origin off the LUCL
- Make the arthrotomy anterior to the LUCL (to preserve it)
- Pronate forearm to protect PIN; incise annular ligament to expose radial neck
- For posterolateral exposure: second arthrotomy posterior to the LUCL with triceps elevation off the posterolateral column
Indications:
- Radial head fractures and arthroplasty
- Capitellum fractures
- LUCL repair / reconstruction (posterolateral rotatory instability)
- Terrible triad injuries (with lateral ligament repair)
- Radial head excision
- Extensile lateral elbow surgery
Dangers:
- PIN (risk if extending distal to the annular ligament)
- LUCL disruption if arthrotomy made too far posteriorly
- Proximal extension limited by the radial nerve along the humerus
Key advantage: Direct access to LUCL and posterolateral structures. The ECU provides inherent protection to the PIN. Well suited for instability surgery.
Clinical Decision Points
Use Kaplan when:
- Radial head fracture involves the anterior portion (the Kaplan gives better anterior exposure)
- You want to reliably preserve the LUCL (the approach is naturally anterior to it)
- PIN decompression is needed
- The coronoid needs lateral access (combined with radial head excision in terrible triad)
Use Kocher when:
- LUCL repair or reconstruction is the primary goal (posterolateral rotatory instability)
- Radial head arthroplasty (broader posterolateral exposure)
- You need a more extensile lateral exposure of the entire lateral column
- Terrible triad with ligamentous disruption requiring repair
Both can be used in terrible triad injuries if fascial disruption guides the approach (Campbell's: "work through any soft-tissue disruption created by the trauma... if a fascial disruption is not present, use the Kaplan or Kocher approach").
Key Memory Points
| Point | Kaplan | Kocher |
|---|---|---|
| Interval "word" | ECRB -- EDC | Anconeus -- ECU |
| Position | Anterior lateral | Posterior lateral |
| PIN risk | More (no ECU cover) | Less (ECU shields PIN) |
| LUCL access | Limited (approach is anterior to it) | Direct (approach at LUCL level) |
| Forearm position | Pronation to protect PIN | Pronation to protect PIN |
Sources: Miller's Review of Orthopaedics 9th Ed, p. 169-170; Campbell's Operative Orthopaedics 15th Ed 2026, Techniques 1.112 and 62.66; Rockwood & Green's Fractures in Adults 10th Ed 2025, p. 1600; Orthobullets.
This is a shared conversation. Sign in to Orris to start your own chat.