Syphillis diagnosis
Reading File
Finding Sources
Searching PubMed
"syphilis"[MeSH Terms] AND "diagnosis"[MeSH Terms]
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive breakdown of syphilis diagnosis, drawn from multiple authoritative textbooks.
Syphilis: Diagnosis
Overview
Diagnosis of syphilis rests on three pillars: clinical recognition by stage, direct detection of the organism, and serologic testing. No single test is sufficient on its own - accurate diagnosis requires combining laboratory results with clinical history and signs.
All patients diagnosed with syphilis should also be tested for HIV infection. - Washington Manual of Medical Therapeutics
1. Clinical Diagnosis by Stage
Recognizing the stage guides which tests to prioritize:
| Stage | Timing | Key Features |
|---|---|---|
| Primary | Weeks after exposure | Painless, indurated, superficial ulcer (chancre); usually single; regional lymphadenopathy |
| Secondary | 2-10 weeks after chancre resolves | Copper-red maculopapular rash (classically involves palms and soles), condylomata lata, mucous patches, constitutional symptoms, diffuse lymphadenopathy |
| Latent (early) | Serologically positive < 1 year, no symptoms | No clinical signs; purely serologic diagnosis |
| Latent (late/unknown duration) | Serologically positive > 1 year | No clinical signs; serologic diagnosis |
| Tertiary | 1-20 years after infection | Gummas, cardiovascular syphilis (aortitis, aortic aneurysm), neurosyphilis |
| Neurosyphilis | Any stage | General paresis, tabes dorsalis, meningovascular disease, ocular syphilis, otosyphilis |
| Congenital | Vertical transmission | Stillbirth, rash, hepatomegaly, "snuffles," saber shins, Hutchinson teeth, 8th nerve deafness |
Secondary syphilis rashes are characteristically non-pruritic and symmetrically distributed. - Symptom to Diagnosis, 4th Edition
2. Direct Detection Methods
Darkfield Microscopy
- Permits definitive diagnosis in primary and secondary syphilis by visual identification of motile spirochetes from lesion exudate (serous fluid, free of red blood cells)
- Spirochetes show characteristic corkscrew morphology and episodic movements
- Limited utility for oral lesions due to presence of saprophytic spirochetes; indirect fluorescent antibody (IFA) test with fluorescein-labeled anti-T. pallidum antibodies is preferred for oral sites
- A negative result warrants repeat testing - Dermatology 2-Volume Set 5e
Polymerase Chain Reaction (PCR)
- Detects T. pallidum DNA; increasingly being employed even for classic presentations
- Particularly useful in: neurosyphilis, congenital syphilis, extra-genital primary syphilis
- In neonates, detection of spirochetemia by PCR can improve sensitivity of congenital syphilis diagnosis
- T. pallidum cannot be routinely cultured in vitro
Histopathology
- Gummas: granulomas with central acellular necrosis + endarteritis obliterans + plasma cell infiltrates
- Warthin-Starry silver stain or immunohistochemistry can identify organisms in tissue
3. Serologic Testing (Most Important in Practice)
Serologic diagnosis requires both non-treponemal AND treponemal tests.
Non-Treponemal Tests (NTTs)
Detect IgG and IgM antibodies against cardiolipin-cholesterol-lecithin antigen (lipoidal material released from damaged host cells and T. pallidum).
| Test | Notes |
|---|---|
| RPR (Rapid Plasma Reagin) | Most common; flocculation test; used for screening and monitoring |
| VDRL (Venereal Disease Research Laboratory) | Standard; used for CSF testing in neurosyphilis |
| USR, RST, TRUST | Less commonly used variants |
Key properties of NTTs:
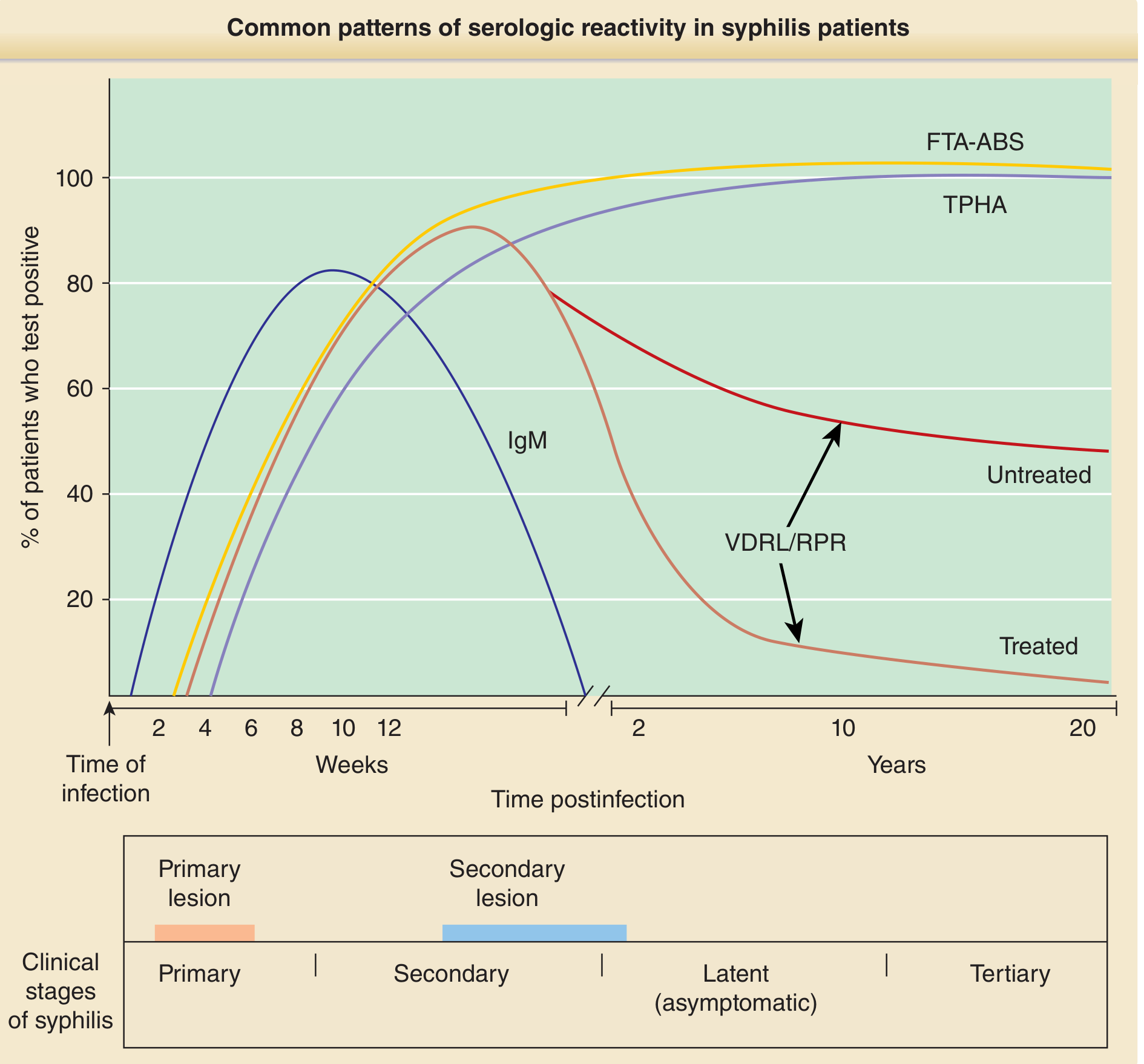
- Become reactive ~4-5 weeks after infection; 100% sensitivity by ~12 weeks
- Results reported as titers (1:2, 1:4, 1:8...); RPR and VDRL titers cannot be directly compared
- Revert to non-reactive in 25-30% of untreated late latent syphilis cases
- A fourfold (two-dilution) decline in titer = successful treatment
- A fourfold increase in titer = relapse or reinfection
- A day-of-treatment titer must be obtained before starting therapy to allow future comparison
- False positives occur (see below)
Treponemal Tests (TTs)
Detect antibodies specific to T. pallidum antigens.
| Test | Notes |
|---|---|
| FTA-ABS (Fluorescent Treponemal Antibody Absorbed) | Highly sensitive; earliest to become reactive |
| TPPA (T. pallidum Particle Agglutination) | Widely used confirmation test |
| TPHA / MHA-TP | Detect antibodies to surface proteins of T. pallidum |
| TP-EIA / Multiplex Flow Immunoassay | Used in reverse sequence screening algorithms |
Key properties of TTs:
- More specific than NTTs; false positives are rare
- IgM and IgG antibodies usually detectable by end of week 4
- Remain positive indefinitely after treatment (serofast) - except in very early syphilis
- Cannot differentiate active from past treated infection
- Sensitivity by stage: 70-100% (primary), 100% (secondary and latent), ~95% (late)
- 90% of patients are TPHA-positive at the time they present with a chancre
Serologic Reactivity Over Time
4. Testing Algorithms
Traditional (Forward) Algorithm
- Screening: NTT (RPR or VDRL)
- Confirmation if positive: Treponemal test (FTA-ABS, TPPA)
Reverse Sequence Algorithm (Increasingly Used)
- Screening: Treponemal EIA or multiplex flow immunoassay
- If reactive: quantitative RPR/VDRL
- If reactive on both: confirms syphilis
- If only treponemal reactive: T. pallidum particle agglutination (TPPA) as a second treponemal test to resolve discordance; ~3% of cases fall into this discordant category
Advantage of reverse sequence: May detect early primary syphilis that NTTs would miss (NTTs can be seronegative in very early primary syphilis). - Washington Manual; Fitzpatrick's Dermatology
5. Neurosyphilis Diagnosis
- Indication for LP: All patients with neurologic, ophthalmic, or otologic symptoms
- CSF VDRL: Highly specific but low sensitivity (a negative VDRL does NOT rule out neurosyphilis)
- CSF abnormalities: elevated protein, pleocytosis (WBC > 5/mm³)
- Some experts recommend LP in HIV+ patients with tertiary disease, treatment failure, or late latent syphilis, though evidence for improved outcomes is limited
6. Congenital Syphilis Diagnosis
- Maternal serology: reactive treponemal and non-treponemal tests
- Infant testing: Quantitative NTT on infant serum (not cord blood - cord blood may give false positives from maternal contamination)
- Treponemal tests in infants are difficult to interpret due to transplacental transfer of maternal IgG
- Additional workup: darkfield/PCR of lesions, CSF VDRL + cell count + protein, long-bone X-rays (periostitis), LFTs, ophthalmologic and auditory brainstem response testing
Stigmata of late congenital syphilis (Hutchinson's triad):
- Hutchinson teeth (notched, peg-shaped incisors)
- Interstitial keratitis
- Eighth-nerve deafness
7. False Positives in Non-Treponemal Tests
Causes of biologic false-positive RPR/VDRL include:
| Acute (< 6 months) | Chronic (> 6 months) |
|---|---|
| Viral infections (EBV, HIV, hepatitis) | SLE and other autoimmune diseases |
| Bacterial infections | Antiphospholipid syndrome |
| Malaria | Chronic liver disease |
| Pregnancy | Aging |
| Recent immunization | Intravenous drug use |
- Treponemal tests have very high specificity; biologic false positives rarely occur with them
- Concurrent positive NTT and TT confirms syphilis; discordant results require clinical judgment
8. Treatment Monitoring
- Repeat nontreponemal tests (RPR) at 3, 6, and 12 months after treatment
- In HIV+ patients: every 3 months for 1 year
- Inadequate response = failure to achieve fourfold decline in titer by 12 months (primary/secondary/early latent) or 24 months (late latent/unknown duration)
- Treponemal tests are not used for monitoring - they remain positive regardless
Sources:
- Dermatology 2-Volume Set 5e (Bolognia), pp. 1753-1754
- Fitzpatrick's Dermatology, pp. 3191-3192
- Washington Manual of Medical Therapeutics, p. 624
- Symptom to Diagnosis: An Evidence-Based Guide, 4th ed., p. 527
This is a shared conversation. Sign in to Orris to start your own chat.