A patient with , fever and guiddines and a known case of seizures has come she is given levipil,what does it do and why is sh admitted,can't she be treated on opd basis
Reading File
Finding Sources
Finding Sources
Searching the Web
levetiracetam Levipil mechanism of action seizure treatment fever admission criteria
Reading File
Reading File
Reading File
I have enough information to give a thorough answer. Here it is:
Levipil (Levetiracetam) - What It Does
Levipil is the brand name for levetiracetam, a second-generation anti-seizure drug (ASD).
Mechanism of Action
Levetiracetam has a novel and unique mechanism compared to older anti-epileptic drugs:
- Primary target: SV2A (Synaptic Vesicle Protein 2A) - It binds selectively to this protein on synaptic vesicles in neurons. SV2A acts as a master regulator of synaptic vesicle exocytosis.
- By binding SV2A, levetiracetam modulates the release of neurotransmitters (both glutamate and GABA) from vesicles, reducing excessive neuronal firing.
- It also inhibits calcium influx via N-type calcium channels and from intracellular calcium stores, further reducing neuronal excitability.
- Unlike older drugs, it does NOT work primarily through sodium channels or GABA enhancement.
(Goodman & Gilman's Pharmacological Basis of Therapeutics)
Pharmacokinetics (why it's useful)
- Rapidly and nearly completely absorbed orally
- Not bound to plasma proteins
- Half-life: 6-8 hours
- Excreted primarily unchanged in urine (65%)
- No CYP450 interactions - does not interact with most other drugs, which is a major advantage
Indications
- Focal (partial) onset seizures
- Primary generalized tonic-clonic seizures
- Myoclonic seizures (e.g., juvenile myoclonic epilepsy)
- Also used as a second-line agent in status epilepticus (after benzodiazepines fail)
Why Was She Admitted? Can't This Be OPD?
This depends critically on the clinical context. Based on your description (fever + known seizure disorder + given levetiracetam), here are the likely reasons for admission:
Reasons Admission Is Warranted
| Scenario | Why Admit |
|---|---|
| Seizure with fever - cause unknown | Fever + seizure in a known epileptic could mean meningitis, encephalitis, or a CNS infection. This must be ruled out before discharge. |
| Complex/prolonged seizure | Any seizure lasting >5 min, multiple seizures in one episode, or seizure with focal features requires inpatient workup. |
| Altered consciousness post-seizure | If she has not returned to baseline (prolonged post-ictal state), she cannot go home. |
| Status epilepticus (or near-status) | If she required IV levetiracetam in emergency (second-line agent), she needs monitoring for respiratory depression, hypotension. |
| New or breakthrough seizure | A seizure despite being on existing medication ("breakthrough seizure") needs medication review and neurological assessment. |
| Fever source needs investigation | The fever itself may be from a serious infection (UTI, sepsis, CNS infection) that triggered the seizure. |
When OPD / Discharge IS Acceptable
According to Rosen's Emergency Medicine, a patient with a simple febrile seizure (single episode, short duration, full recovery, no neurological deficit) can be sent home with:
- Instructions on recurrence risk (>33%)
- Fever management guidance
- Emergency seizure protocol education
- Close follow-up with their neurologist/pediatrician
The Key Question
The reason she is NOT on OPD basis is likely because:
- The fever source hasn't been identified yet - meningitis/encephalitis must be excluded
- She may have had a complex or prolonged seizure
- She needed IV medication (levetiracetam IV is used when oral is not feasible, typically in acute/emergency settings)
- Her neurological status post-seizure may not have fully normalized
Summary
- Levipil works by binding SV2A on synaptic vesicles, reducing glutamate/GABA release and calcium influx, thereby suppressing abnormal neuronal firing.
- Admission is needed when fever + seizure combination raises concern for CNS infection, the seizure was complex/prolonged, the patient hasn't returned to baseline, or the underlying cause of the fever needs urgent workup.
- OPD discharge is appropriate only after the fever source is identified as benign, the seizure was simple and brief, and the patient has fully recovered to baseline.
She doesn't has seizures and fever,she has guiddines and simeizures
Asking for Preferences
Asking for Preferences
Finding Sources
Finding Sources
Searching the Web
seizure with giddiness dizziness admission criteria vs outpatient epilepsy management
Finding Sources
Finding Sources
Reading File
Finding Sources
I now have excellent content. Here is a full, corrected answer:
The Patient: Giddiness + Seizures (Known Epileptic), Given Levipil
What is the Connection Between Giddiness and Seizures?
This is clinically very important. Giddiness/vertigo can be directly related to epilepsy in two ways:
1. Vertigo as an Aura of a Seizure
As stated in Adams and Victor's Principles of Neurology:
"Vertigo may constitute the aura of an epileptic seizure... electrical stimulation of the posterolateral temporal lobe or inferior parietal lobule adjacent to the Sylvian fissure may evoke intense vertigo."
In this case, the giddiness she feels is the warning sign (aura) just before the seizure begins - it originates from cortical activity in the temporal/parietal region. The sensation typically lasts seconds before seizure activity takes over.
2. Vertiginous Epilepsy
A rare form where the seizure itself presents predominantly as vertigo/dizziness, with the patient feeling movement of their body or the environment around them.
3. Post-ictal Dizziness
Giddiness may also occur after a seizure (post-ictal phase) due to the brain's recovery period.
So in this patient, giddiness is not a separate problem - it is part of the seizure disorder itself.
What Does Levipil (Levetiracetam) Do?
Unique Mechanism of Action
Levetiracetam works through a completely novel mechanism different from all older anti-epileptic drugs:
- Binds SV2A (Synaptic Vesicle Protein 2A) - a protein on nerve terminals that regulates how neurotransmitter-filled vesicles are released
- By binding SV2A, it reduces the excessive release of glutamate (the main excitatory neurotransmitter that drives seizures)
- Also inhibits N-type calcium channels and blocks calcium release from intracellular stores, reducing neuronal hyperexcitability
- Net result: dampens abnormal, synchronous neuronal firing that produces seizures
(Goodman & Gilman's Pharmacological Basis of Therapeutics)
Why is it a Good Choice?
- Works against focal seizures, generalized tonic-clonic seizures, and myoclonic seizures
- No CYP450 interactions - safe to combine with other drugs
- Oral and IV forms available
- Minimal protein binding - predictable blood levels
- Also used as a second-line emergency agent when benzodiazepines fail in status epilepticus
Why Admitted? Can't She Be Treated OPD?
Reasons She Needs Admission
| Clinical Concern | Why It Requires Inpatient Care |
|---|---|
| Giddiness + seizure = possible aura, meaning seizure may not be fully controlled | Dose optimization of Levipil needs monitoring |
| Breakthrough seizure (seizure despite being on medication) | Needs drug level check, dose adjustment, possible add-on drug - unsafe to do this unsupervised |
| Risk of seizure recurrence within hours | Patient needs to be observed for further episodes in a monitored setting |
| Giddiness can cause falls | A known epileptic with active giddiness is at high fall/injury risk - unsafe at home |
| IV Levipil may have been given | IV administration requires hospital monitoring (for blood pressure, respiratory status) |
| Need for workup | EEG, MRI brain, drug levels, electrolytes - these require inpatient coordination |
| Safety during post-ictal state | Altered consciousness or confusion post-seizure means the patient cannot be discharged |
When OPD IS Acceptable
OPD management is fine for a stable, well-controlled epileptic who:
- Had no recent seizure or only a single brief self-terminating episode
- Has fully returned to baseline with no giddiness/confusion
- Is already on a stable, optimized dose of anti-epileptic medication
- Has a reliable caregiver at home
- Does NOT have breakthrough seizures
This patient - with active giddiness + seizure in a known epileptic - does not meet OPD criteria. The combination suggests her epilepsy is currently not well controlled, which requires inpatient assessment, drug optimization, and safety monitoring.
Bottom line: Her giddiness is likely a seizure aura (part of the epilepsy itself), Levipil is suppressing the abnormal neuronal firing via SV2A, and she is admitted because an epileptic with active symptoms and a possible breakthrough seizure cannot be safely managed outside a hospital until her condition is stabilized.
Tell everything about ild in simple and in short
Reading File
Finding Sources
Searching the Web
interstitial lung disease ILD overview causes diagnosis treatment 2024
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
I now have comprehensive information from Goldman-Cecil Medicine (the definitive internal medicine textbook) and Fishman's Pulmonary Diseases. Here is a clear, simple, thorough answer:
ILD - Interstitial Lung Disease (Simple & Short)
🫁 What Is It?
ILD is not one disease - it is a whole group of 200+ lung conditions that all share one thing in common:
The interstitium (the tissue walls surrounding the air sacs / alveoli) gets inflamed and/or scarred (fibrosis), making the lungs stiff and reducing the ability to get oxygen into the blood.
Think of the lung like a sponge. Normally it's soft and flexible. In ILD, the sponge gets thick, stiff, and scarred - so it can't absorb oxygen well.
📋 Types / Classification
(Goldman-Cecil Medicine)
| Category | Examples |
|---|---|
| Idiopathic (unknown cause) | IPF (Idiopathic Pulmonary Fibrosis) - most common and most serious; Nonspecific Interstitial Pneumonia (NSIP) |
| Smoking-related | Respiratory Bronchiolitis-ILD; Desquamative Interstitial Pneumonia (DIP) |
| Connective Tissue Disease | Rheumatoid arthritis, Scleroderma, SLE, Sjogren's, Polymyositis |
| Hypersensitivity (inhaled antigens) | Farmer's lung (moldy hay), Bird fancier's lung (bird droppings/feathers) |
| Drug-induced | Bleomycin, Amiodarone, Methotrexate, Nitrofurantoin |
| Occupational/Environmental | Asbestosis (shipyard), Silicosis (sandblasting), Berylliosis (aerospace) |
| Sarcoidosis | Granulomas in the lung |
| Acute forms | Cryptogenic Organizing Pneumonia (COP), Acute Interstitial Pneumonia (AIP) |
⚠️ Causes / Risk Factors
- Smoking (especially for RB-ILD, DIP)
- Autoimmune/connective tissue diseases (RA, scleroderma, lupus)
- Environmental/occupational exposure (birds, molds, dust, asbestos, silica)
- Drugs (chemo drugs, amiodarone, methotrexate, nitrofurantoin)
- Radiation to the chest
- Genetic/inherited (familial IPF)
- Unknown (idiopathic) - the most common form (IPF) has no known cause
😮💨 Symptoms
| Symptom | Details |
|---|---|
| Breathlessness (dyspnea) | Starts with exertion, gets worse over time - the hallmark symptom |
| Dry cough | Non-productive, persistent |
| Fatigue | Due to low oxygen |
| Clubbing of fingers | Especially in IPF |
| Velcro crackles | Fine crackling sound at lung bases on listening - very characteristic |
| Cyanosis | Bluish lips/fingers in advanced disease |
🔬 Diagnosis
- History - age, smoking, occupation, birds/molds at home, drugs used
- Chest X-ray - bilateral haziness ("ground glass"), lower zone involvement
- HRCT (High Resolution CT) - the most important test; shows honeycombing pattern in IPF, ground-glass in NSIP
- Pulmonary Function Tests (PFTs) - shows restrictive pattern (low FVC, low TLC, low DLCO)
- Bronchoalveolar lavage (BAL) - fluid washout to look at cell types
- Lung biopsy (video-assisted thoracoscopic surgery / VATS) - gold standard when diagnosis is unclear
- Blood tests / serology - ANA, anti-CCP, anti-Scl70 to find autoimmune cause
💊 Treatment
| Cause | Treatment |
|---|---|
| IPF | Antifibrotic drugs: Nintedanib (pan-tyrosine kinase inhibitor) or Pirfenidone - slow progression, do NOT reverse fibrosis |
| Autoimmune-related ILD | Immunosuppressants: steroids (prednisolone), mycophenolate, azathioprine, cyclophosphamide |
| Hypersensitivity Pneumonitis | Remove the cause (stop bird exposure, fix moldy environment) + steroids |
| Drug-induced ILD | Stop the offending drug immediately |
| Sarcoidosis | Corticosteroids |
| All severe ILD | Oxygen therapy, pulmonary rehab |
| End-stage / severe | Lung transplantation |
📌 Key Points to Remember
| Fact | Detail |
|---|---|
| Most common ILD | IPF - older adults (>50 yrs), men, smokers |
| Worst prognosis | IPF - median survival only 3-5 years from diagnosis |
| Only in women of childbearing age | Lymphangioleiomyomatosis (LAM) |
| Smokers only | RB-ILD, DIP |
| Young adults | Sarcoidosis |
| Pathognomonic HRCT finding | Honeycombing + traction bronchiectasis in IPF |
| PFT pattern | Always restrictive (not obstructive) |
| Classic auscultation finding | Bilateral basal Velcro crackles |
Bottom line: ILD = group of lung diseases where the lung scaffold gets inflamed/scarred → stiff lungs → can't breathe well. Key to management is finding the cause (drug? bird? autoimmune?) because removing the cause is often the best treatment. When no cause is found (IPF), antifibrotic drugs like nintedanib and pirfenidone slow the scarring but cannot reverse it.
(Goldman-Cecil Medicine, Fishman's Pulmonary Diseases and Disorders)
Pain abdomen, vomiting,loose stools, non blood tingedd
Finding Sources
Finding Sources
Searching the Web
abdominal pain vomiting non bloody loose stools differential diagnosis causes treatment
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive, high-quality content from Tintinalli's Emergency Medicine. Here is the full, simple, clinical answer:
Pain Abdomen + Vomiting + Loose Stools (Non-Bloody) - Full Clinical Picture
🔍 What Is This?
This is the classic presentation of Acute Gastroenteritis - inflammation of the stomach and intestines causing the triad of:
- Abdominal pain/cramps
- Vomiting
- Loose, non-bloody watery diarrhea
🦠 Causes (By Onset Time)
(Tintinalli's Emergency Medicine)
| Onset After Eating | Organism | Mechanism |
|---|---|---|
| 1-6 hours | S. aureus toxin, B. cereus (preformed toxin), Norovirus | Preformed toxin already in food → rapid vomiting + cramps |
| 6-24 hours | B. cereus (diarrhea toxin), C. perfringens | Toxin produced after ingestion |
| 24-48 hours | Salmonella, Enterotoxigenic E. coli (ETEC), Rotavirus | Bacterial invasion or toxin disrupts gut lining |
| 2-6 days | Campylobacter, Shigella, Vibrio cholerae, Yersinia | Deeper invasion, may cause bloody diarrhea |
| 1-2+ weeks | Giardia, Entamoeba, Cryptosporidium, Hepatitis A | Parasites, chronic/traveler's diarrhea |
Non-bloody diarrhea specifically = most commonly viral (Norovirus, Rotavirus) or enterotoxin-mediated (ETEC, C. perfringens, S. aureus) - toxins cause fluid shift into the gut without destroying the intestinal lining.
⚠️ Differential Diagnoses (Don't Miss These)
| Condition | Clues |
|---|---|
| Viral gastroenteritis | Most common; self-limiting, afebrile or mild fever, community outbreak |
| Food poisoning | Multiple people affected, rapid onset after a specific meal |
| Acute appendicitis | Pain starts around navel then shifts to RLQ, vomiting, may have loose stools post-perforation - must rule out! |
| Acute pancreatitis | Severe epigastric pain radiating to back, vomiting |
| Cholera | Profuse rice-water stools, severe dehydration rapidly |
| IBS flare | Chronic recurrent history, no fever |
| Early IBD | Recurrent, may have blood later |
| Ectopic pregnancy | In women of reproductive age - check always |
| Mesenteric ischemia | Elderly, severe pain out of proportion to examination |
Key differentiator: Non-bloody stools points away from invasive bacteria (Shigella, STEC) and toward secretory/toxin-mediated or viral cause.
🏥 When to Do Tests?
Tests are NOT needed in every patient. Do stool culture / investigations only if:
- Bloody diarrhea
- Fever ≥38.5°C
- Illness lasting >1 week
- Severe abdominal pain
- Elderly (≥70 yrs), immunocompromised, pregnant
- Recent antibiotic use or hospitalization
- Traveler's diarrhea
For routine non-bloody diarrhea - no stool culture needed.
💊 Treatment
(Tintinalli's Emergency Medicine, IDSA 2017 Guidelines)
Step 1 - Rehydration (Most Important)
- ORS (Oral Rehydration Solution) - WHO recommends glucose-containing ORS (e.g., Pedialyte, Electral)
- IV fluids (Normal Saline or Ringer's Lactate) only if patient cannot tolerate oral fluids or has severe dehydration
Step 2 - Symptomatic Drugs
| Drug | Use | Caution |
|---|---|---|
| Ondansetron (antiemetic) | Reduces vomiting, shortens ED stay | Safe in adults and older children |
| Loperamide (Imodium) | Reduces diarrhea in mild-moderate non-bloody cases in adults | Avoid in children, fever, bloody diarrhea - may prolong illness |
| Domperidone/Metoclopramide | Alternative antiemetics | |
| Antispasmodics (e.g., hyoscine) | Abdominal cramps |
Step 3 - Antibiotics?
Most cases do NOT need antibiotics - viral and self-limited bacterial causes are the majority.
Give antibiotics only for:
- Infants <3 months
- Immunocompromised with severe illness
- Fever + bloody diarrhea + suspected Shigella
- Travelers with high fever or sepsis signs
If antibiotics needed: Oral ciprofloxacin 500 mg BD or levofloxacin 500 mg OD for 3 days.
⚠️ Do NOT give antibiotics if STEC (E. coli O157) is suspected - increases risk of life-threatening HUS (Hemolytic Uremic Syndrome)
🚨 Red Flags - Admit the Patient If:
- Severe dehydration (sunken eyes, dry mouth, reduced urine output, altered consciousness)
- Can't keep any fluids down
- Bloody diarrhea
- High fever
- Severe constant (not crampy) abdominal pain - rule out appendicitis, pancreatitis
- Elderly, infant, immunocompromised
📋 Simple Summary
Non-bloody loose stools + vomiting + pain = Acute Gastroenteritis
↓
Most likely: Viral OR food poisoning (toxin-mediated)
↓
Treatment: ORS + antiemetic + loperamide (adults only)
↓
No antibiotics unless red flags
↓
Admit only if severe dehydration or red flags present
(Tintinalli's Emergency Medicine - A Comprehensive Study)
A patient with febrile illness under evaluation ,what and will be evaluated
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is the complete, simple guide to evaluating a febrile illness:
Febrile Illness Under Evaluation - Complete Approach
🌡️ What Does "Febrile Illness Under Evaluation" Mean?
It means a patient has fever but the cause is not yet clear. The goal is to systematically work through history → examination → investigations to find what is causing the fever.
If fever persists >3 weeks with temp >38.3°C and no diagnosis after 3 days inpatient (or 3 OPD visits) - it becomes Fever of Unknown Origin (FUO).
📊 Four Big Categories of Causes
(Frameworks for Internal Medicine - shown in diagram above)
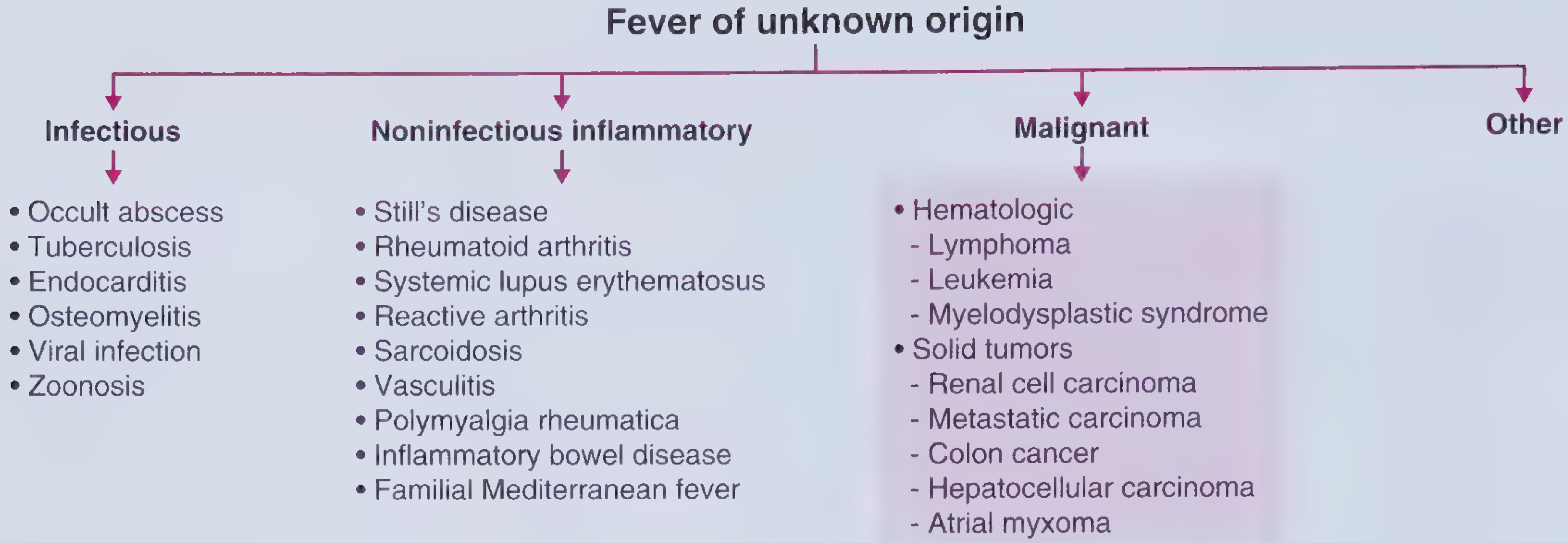
| Category | Common Causes |
|---|---|
| Infectious | TB, abscess, endocarditis, osteomyelitis, viral (CMV, EBV, HIV), zoonoses |
| Non-infectious Inflammatory | Rheumatoid arthritis, SLE, Still's disease, sarcoidosis, vasculitis, IBD |
| Malignant | Lymphoma, leukemia, renal cell carcinoma, HCC, colon cancer, atrial myxoma |
| Other | Drug fever, pulmonary embolism, alcoholic hepatitis, thyroiditis, factitious fever |
📋 STEP 1 - History (What to Ask)
Basic Information
- Age & sex - helps narrow (IPF in >50 yrs men; lymphoma in young adults; SLE in young women)
- Duration of fever - acute (<2 weeks) vs. prolonged (FUO)
- Pattern of fever - continuous, intermittent, remittent, hectic
Key History Points
| Area | What to Ask |
|---|---|
| Travel history | Malaria, typhoid, dengue, leishmaniasis |
| Occupation | Farming (brucellosis, leptospirosis), healthcare worker |
| Animal/Bird contact | Zoonoses - cat scratch (Bartonella), birds (psittacosis), farm animals (Q fever) |
| Sexual history | HIV, gonorrhea, syphilis |
| Drug history | Drug fever (antibiotics, NSAIDs, antiepileptics can cause fever) |
| Dental procedures | Endocarditis |
| Weight loss | Malignancy, TB |
| Night sweats | TB, lymphoma |
| Joint pains | Reactive arthritis, SLE, Still's disease |
| Rash | SLE, meningococcemia, dengue, typhoid (rose spots) |
| Recent surgeries / IV lines | Hospital-acquired infection, abscess |
| Family history | Familial Mediterranean Fever (FMF) especially in Mediterranean ethnicity |
| Immunocompromised | HIV, steroids, chemotherapy - think atypical organisms |
🩺 STEP 2 - Physical Examination (What to Look For)
| Finding | Suggests |
|---|---|
| Lymphadenopathy | Lymphoma, EBV, TB, HIV |
| Splenomegaly | Malaria, EBV, typhoid, leukemia, endocarditis |
| Hepatomegaly / jaundice | Hepatitis, liver abscess, HCC, alcoholic hepatitis |
| Heart murmur | Endocarditis (especially after dental work) |
| Skin rash | SLE, dengue, meningococcemia, drug fever |
| Joint swelling | RA, reactive arthritis, Still's disease |
| Neck stiffness | Meningitis |
| Fundus exam | Roth spots (endocarditis), papilloedema (raised ICP - meningitis) |
| Conjunctival suffusion | Leptospirosis |
| Tender neck | Thyroiditis |
| Clubbing | Infective endocarditis, lung abscess, IBD |
| Pulse-temperature dissociation (pulse slow despite high fever) | Typhoid, brucellosis, Legionella |
🔬 STEP 3 - Investigations (What to Order)
Tier 1 - Always Do First (Routine)
| Test | What It Tells You |
|---|---|
| CBC with differential | Leukocytosis (bacterial), leukopenia (viral/typhoid/SLE), eosinophilia (parasites), anemia (malaria/chronic disease), thrombocytopenia (dengue/malaria) |
| ESR / CRP | Elevated = active inflammation; helps monitor response to treatment |
| LFT (Liver Function Test) | Hepatitis, liver abscess, drug fever, HCC |
| RFT (Kidney Function Test) | Leptospirosis, sepsis, renal TB |
| Urine routine + culture | UTI, renal TB |
| Blood culture x 3 | Bacteremia, endocarditis - draw before starting antibiotics |
| Chest X-ray | TB, pneumonia, sarcoidosis (hilar lymphadenopathy), lung abscess |
| Blood sugar | Immunocompromise from diabetes |
Tier 2 - Based on Clinical Clues
| Test | When to Order |
|---|---|
| Peripheral blood smear | Malaria, dengue - if travel history or thrombocytopenia |
| Dengue NS1 / IgM / IgG | Fever + thrombocytopenia + rash |
| Widal test / Typhidot | Sustained fever + relative bradycardia + rose spots |
| HIV test | Any unexplained prolonged fever |
| Mantoux / IGRA (Quantiferon TB) | Suspected TB - cough, night sweats, weight loss |
| Sputum AFB / culture | TB |
| ANA, anti-dsDNA, complement | Suspected SLE - young woman, joint pains, rash |
| Rheumatoid factor, anti-CCP | Suspected RA |
| Serum ferritin | Very high (>10,000) → Still's disease |
| LDH | Lymphoma |
| Echocardiography | Suspected endocarditis, atrial myxoma |
| Urine / serum protein electrophoresis | Multiple myeloma |
| AFP (alpha-fetoprotein) | Suspected HCC |
Tier 3 - Advanced (If Still No Diagnosis)
| Test | When |
|---|---|
| CT chest / abdomen / pelvis | Abscess, lymphoma, malignancy, miliary TB |
| MRI spine | Osteomyelitis (most common site in FUO) |
| PET scan | Occult malignancy or infection |
| Bone marrow biopsy | Suspected leukemia, lymphoma, TB, leishmania |
| Lymph node biopsy | Lymphadenopathy - TB, lymphoma, sarcoidosis |
| Liver biopsy | Hepatic TB, granulomatous hepatitis |
| Bronchoalveolar lavage (BAL) | Miliary TB, atypical pneumonia |
| Serology | Leptospirosis, Brucella, Q fever (Coxiella), Bartonella, CMV, EBV |
⚠️ Key Points to Remember
| Point | Detail |
|---|---|
| Always take blood cultures before starting antibiotics | Pre-treatment cultures are critical |
| Drug fever is diagnosis of exclusion | Fever resolves within 2 days of stopping the drug |
| Pulse-temp dissociation | Important clue for typhoid / brucellosis |
| Lymphoma in FUO = bad prognosis | Rapid progression |
| PE can cause fever | In 50% of cases - do D-dimer / CTPA if suspected |
| Most common site of osteomyelitis in FUO | Spine - order MRI spine |
| Factitious fever | Consider in healthcare workers with "fever" but who look completely well |
🗂️ Simple Summary
Febrile illness under evaluation
↓
HISTORY: Duration, travel, animals, drugs, weight loss, night sweats
↓
EXAMINATION: Lymph nodes, spleen, liver, heart, skin, joints
↓
TIER 1 TESTS: CBC, CRP/ESR, blood culture x3, urine culture, CXR, LFT, RFT
↓
TIER 2 TESTS: Based on clinical clues (malaria smear, dengue, Widal, ANA, HIV...)
↓
TIER 3 TESTS: CT/MRI, biopsy, PET scan if still no diagnosis
↓
FOUR CAUSES: Infectious | Inflammatory | Malignant | Other
(Frameworks for Internal Medicine, Tintinalli's Emergency Medicine)
This is a shared conversation. Sign in to Orris to start your own chat.