Explain about sulphonamides
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive content from authoritative textbooks. Let me compile the full, detailed answer.
Sulphonamides (Sulfonamides)
Sulphonamides were among the first synthetic antibacterial agents ever developed - their introduction in the 1930s marked a turning point in the treatment of bacterial infections. They remain clinically relevant today, especially in fixed combinations with dihydrofolate reductase inhibitors.
1. Chemistry & Structure
Sulphonamides are structural analogues of para-aminobenzoic acid (PABA). They share the core sulfonamide group (-SO₂NH₂) attached to an aromatic amine. Different substituents on the nitrogen of the sulfonamide moiety give rise to different compounds with varying pharmacokinetic profiles.
Chemical structures: Sulphonamides and their PABA analogue
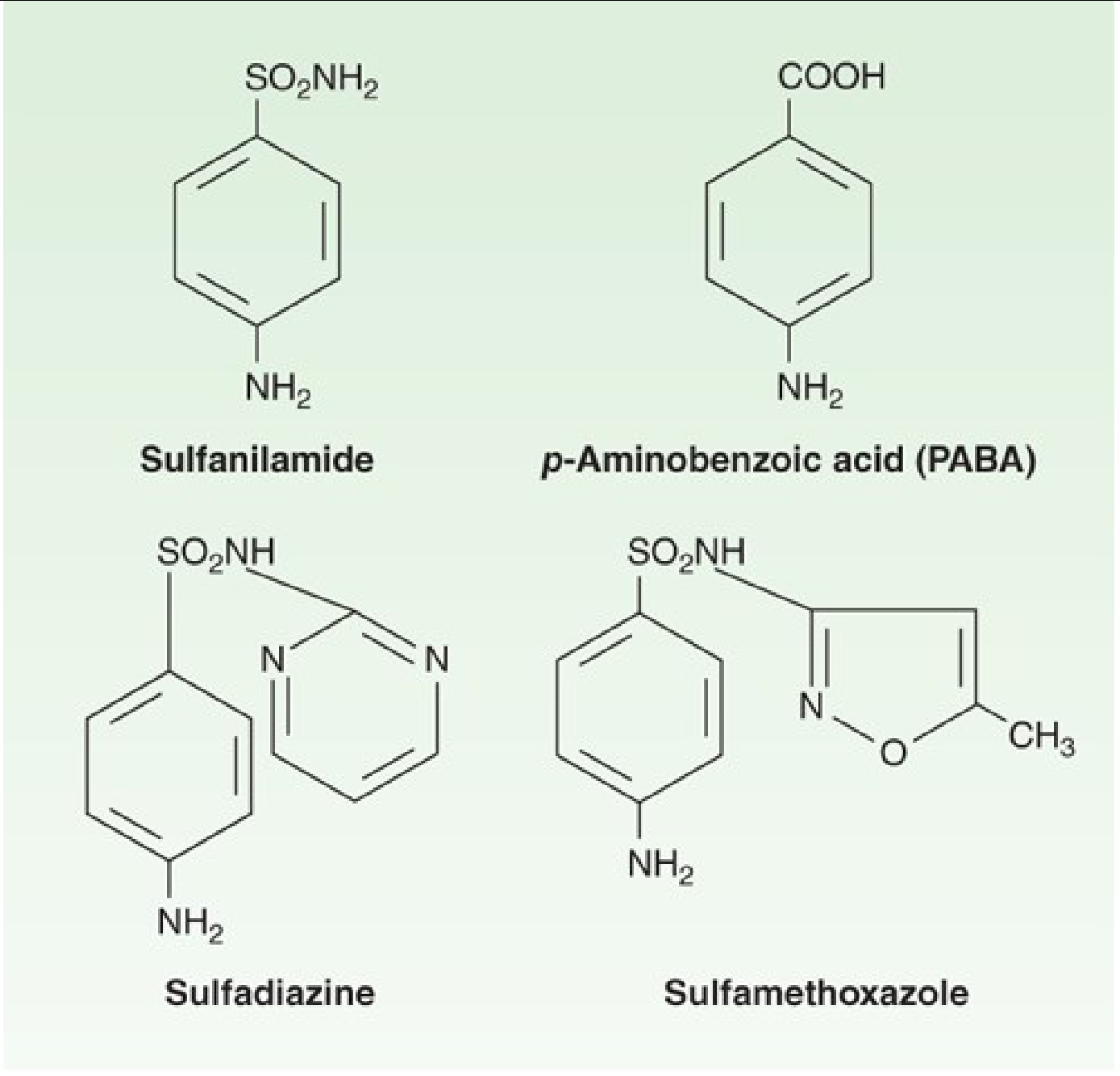
Structures of sulfonamides compared to PABA - Katzung's Basic & Clinical Pharmacology, 16th Edition
2. Mechanism of Action
Key principle: Susceptible organisms (unlike mammals) cannot use exogenous folate - they must synthesize it from PABA. Sulfonamides exploit this difference.
Sulfonamides act as competitive inhibitors of dihydropteroate synthase, the enzyme that converts PABA into dihydrofolic acid. Blocking this step prevents the downstream synthesis of tetrahydrofolate, which is required for purine synthesis and ultimately DNA replication.
The folate synthesis pathway and sites of drug action:
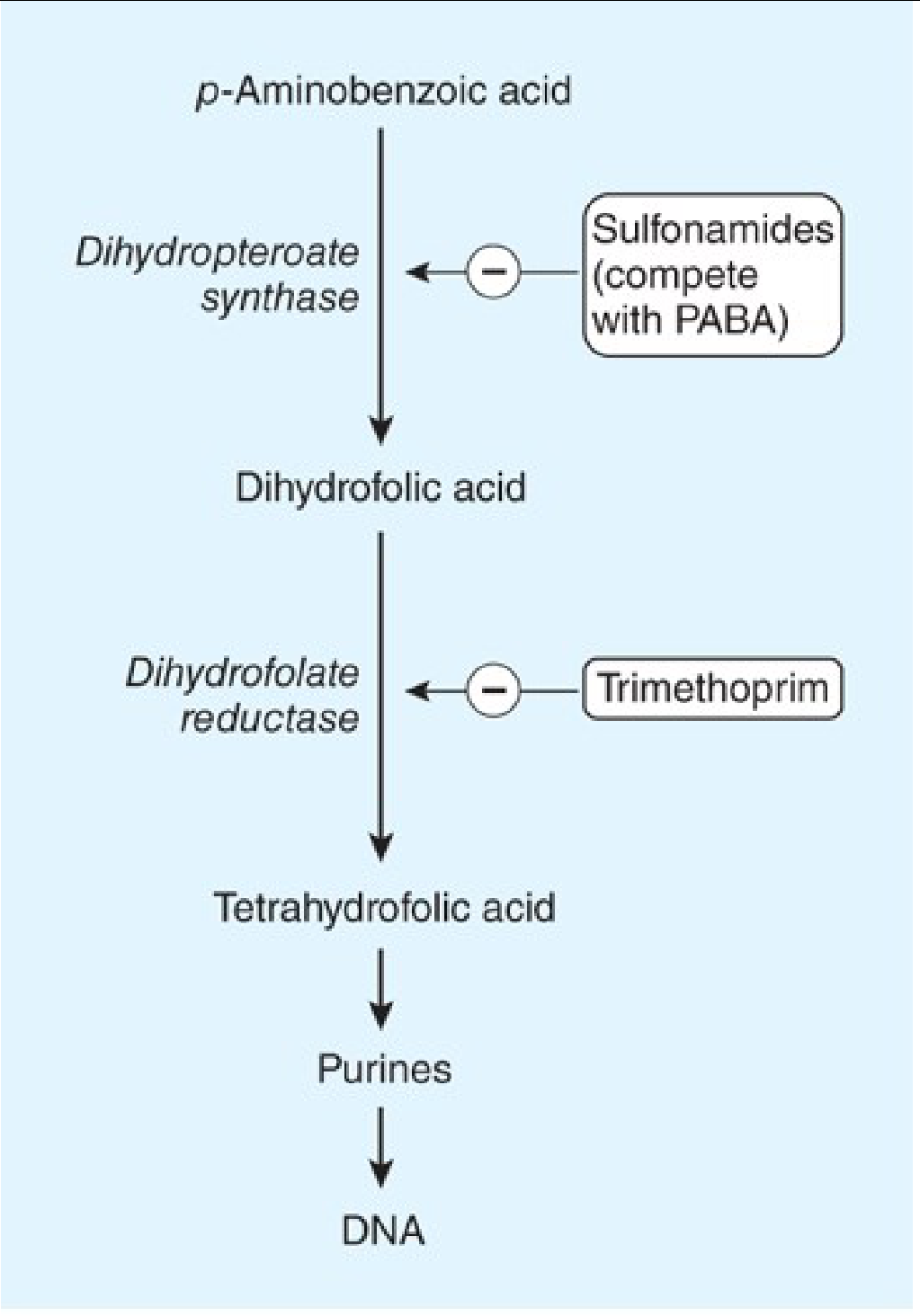
Actions of sulfonamides and trimethoprim on folate synthesis - Katzung's Basic & Clinical Pharmacology, 16th Edition
The action is bacteriostatic (not bactericidal) when used alone. When combined with trimethoprim (a dihydrofolate reductase inhibitor), the combination achieves sequential blockade of two steps in the same pathway, producing synergistic bactericidal activity.
3. Antimicrobial Spectrum
Sulphonamides inhibit a broad range of organisms:
| Category | Examples |
|---|---|
| Gram-positive bacteria | Staphylococcus, Streptococcus |
| Gram-negative enteric bacteria | E. coli, Klebsiella pneumoniae, Salmonella, Shigella, Enterobacter |
| Other bacteria | Nocardia spp., Chlamydia trachomatis |
| Protozoa | Toxoplasma gondii, some malarial parasites |
Organisms NOT covered:
- Anaerobes (poor activity)
- Pseudomonas aeruginosa (intrinsically resistant)
- Rickettsiae (growth may actually be stimulated by sulphonamides)
4. Pharmacokinetics
Sulphonamides are broadly divided into three groups based on route and absorption:
A. Oral, Absorbable
- Absorbed from stomach and small intestine
- Distributed widely to tissues, body fluids, CNS/CSF, placenta, and fetus
- Protein binding: 20% to over 90% (varies by agent)
- Therapeutic blood levels: 40-100 mcg/mL
- Peak levels: 2-6 hours after oral administration
- Metabolism: acetylation or glucuronidation in the liver
- Excretion: primarily renal (glomerular filtration); dose reduction required in renal failure
Key agents: Sulfamethoxazole (used as TMP-SMX), sulfadiazine, sulfadoxine (long-acting)
B. Oral, Nonabsorbable
- Sulfasalazine - acts locally in the gut; used in inflammatory bowel disease. The sulphonamide component (sulfapyridine) is split off by colonic bacteria from the active moiety (5-aminosalicylic acid/mesalamine).
C. Topical
- Sodium sulfacetamide - ophthalmic drops/ointment for bacterial conjunctivitis
- Mafenide acetate - topical; used for burn wounds; inhibits carbonic anhydrase as a side effect, can cause metabolic acidosis
- Silver sulfadiazine - widely used for burn wound prophylaxis; may slow wound healing
5. Resistance Mechanisms
Sulphonamide resistance can arise through several mechanisms:
- Overproduction of PABA - overwhelms the competitive inhibition
- Altered dihydropteroate synthase - low-affinity enzyme for sulfonamides (commonly plasmid-encoded - transferable resistance)
- Impaired drug permeability - reduced uptake into bacteria
- Use of exogenous folate - some bacteria lack the folate synthesis pathway entirely and import folate from the environment, making them intrinsically resistant
Many formerly susceptible species (meningococci, pneumococci, streptococci, staphylococci, gonococci) are now widely resistant.
6. Clinical Uses
Sulphonamides are rarely used as single agents today due to widespread resistance. Their main role is in fixed-dose combinations.
| Clinical Use | Drug Combination |
|---|---|
| Pneumocystis jirovecii pneumonia (PCP) | TMP-SMX (drug of choice) |
| Toxoplasma gondii (toxoplasmosis) | Sulfadiazine + pyrimethamine (first-line) |
| Nocardiosis | TMP-SMX |
| UTIs (uncomplicated) | TMP-SMX |
| Acute otitis media, sinusitis | TMP-SMX |
| Malaria (second-line, some regions) | Sulfadoxine + pyrimethamine (Fansidar) |
| Inflammatory bowel disease | Sulfasalazine |
| Burn wound prophylaxis | Silver sulfadiazine, mafenide acetate |
| Bacterial conjunctivitis | Sodium sulfacetamide (ophthalmic) |
7. Adverse Effects
Sulphonamides have a significant adverse effect profile:
Hypersensitivity Reactions
- Fever and rashes (most common)
- Morbilliform, urticarial, scarlatinal, purpuric rashes
- Stevens-Johnson syndrome (SJS) / Toxic Epidermal Necrolysis (TEN) - severe, potentially life-threatening
- Erythema multiforme, erythema nodosum
- Serum sickness-like syndrome
- Drug reaction with eosinophilia and systemic symptoms (DRESS)
Renal Toxicity
- Crystalluria and obstructive nephropathy (particularly with older, less soluble sulphonamides)
- Adequate hydration and alkalinization of urine help prevent this
Hematological Effects
- Hemolytic anemia (especially in patients with G6PD deficiency)
- Agranulocytosis
- Aplastic anemia
- Thrombocytopenia
Other Effects
- Kernicterus in neonates - sulphonamides displace bilirubin from albumin; contraindicated in neonates and near-term pregnancy
- Hepatotoxicity (rare)
- Photosensitivity
- GI intolerance (nausea, vomiting)
- In AIDS patients on TMP-SMX: unusually high incidence of toxic effects
8. Drug Interactions
- Warfarin: sulphonamides potentiate anticoagulant effect (displace from protein binding, inhibit CYP2C9)
- Phenytoin: increased phenytoin levels (protein displacement + metabolism inhibition)
- Sulfonylureas: cross-reactivity concerns (structurally related); risk of hypoglycemia
- Methotrexate: additive bone marrow suppression
- Cyclosporine: increased nephrotoxicity
9. Contraindications
- Neonates and near-term pregnancy (risk of kernicterus)
- Known hypersensitivity to sulphonamides
- Severe renal/hepatic impairment (use with caution/dose adjustment)
- G6PD deficiency (relative contraindication - risk of hemolysis)
10. Cross-Reactivity Note
Many drugs contain a sulfonamide moiety (thiazide diuretics, loop diuretics except ethacrynic acid, sulfonylureas, COX-2 inhibitors). Historically these were considered cross-allergenic with antimicrobial sulphonamides, but more recent evidence suggests cross-reactivity between antibiotic sulphonamides and non-antibiotic sulfonamide-containing drugs is uncommon, due to structural differences. Ethacrynic acid is the only loop diuretic that is NOT a sulphonamide derivative, making it a preferred choice in patients with sulphonamide allergy.
Summary Table: Key Sulphonamides
| Drug | Route | Key Use |
|---|---|---|
| Sulfamethoxazole | Oral | Combined with TMP - broad indications |
| Sulfadiazine | Oral | Toxoplasmosis (with pyrimethamine) |
| Sulfadoxine | Oral | Long-acting; malaria (with pyrimethamine) |
| Sulfasalazine | Oral | IBD, rheumatoid arthritis |
| Silver sulfadiazine | Topical | Burn wound prophylaxis |
| Mafenide acetate | Topical | Burn wounds |
| Sodium sulfacetamide | Ophthalmic | Bacterial conjunctivitis |
Sources:
- Katzung's Basic and Clinical Pharmacology, 16th Edition, Chapter 46
- Goodman & Gilman's The Pharmacological Basis of Therapeutics
- Sherris & Ryan's Medical Microbiology, 8th Edition
- Jawetz, Melnick & Adelberg's Medical Microbiology, 28th Edition
This is a shared conversation. Sign in to Orris to start your own chat.