angina perioperative management -act like a professor in anesthesia and explain this question to resident for md final exams
Perioperative Management of Angina - A Professor's Lecture for MD Final Exams
The Core Physiologic Framework - Never Forget This
- Coronary perfusion pressure (diastolic BP - LVEDP)
- Diastolic filling time (heart rate - slower = more time)
- Oxygen-carrying capacity (Hb, SaO2)
- Coronary vascular tone (vasospasm vs. dilation)
- Heart rate (most important - also reduces supply)
- Wall stress (afterload x radius / 2 x wall thickness - LaPlace)
- Contractility
Part 1: Preoperative Assessment
Step 1 - Urgency of Surgery (The Non-Negotiable First Step)
- Emergency surgery: Proceed immediately. Risk-stratify clinically, set up appropriate monitoring, and manage risk factors postoperatively. No time for workup.
- Urgent/elective surgery: Proceed through the full stepwise algorithm below.
Step 2 - Identify Active Cardiac Conditions (These STOP Elective Surgery)
| Condition | Example |
|---|---|
| Unstable coronary syndromes | Unstable angina, recent MI (<30 days) |
| Decompensated heart failure | NYHA Class IV, new or worsening HF |
| Significant arrhythmias | High-degree AV block, symptomatic SVT/VT |
| Severe valvular disease | Severe AS (AVA <1 cm²), severe symptomatic MR |
- MI within 7 days = "active" condition - do NOT proceed
- MI within 1 month with myocardium still at ischemic risk = also "active" - delay
- Old MI with no ischemic territory at risk = low risk - proceed after full algorithm
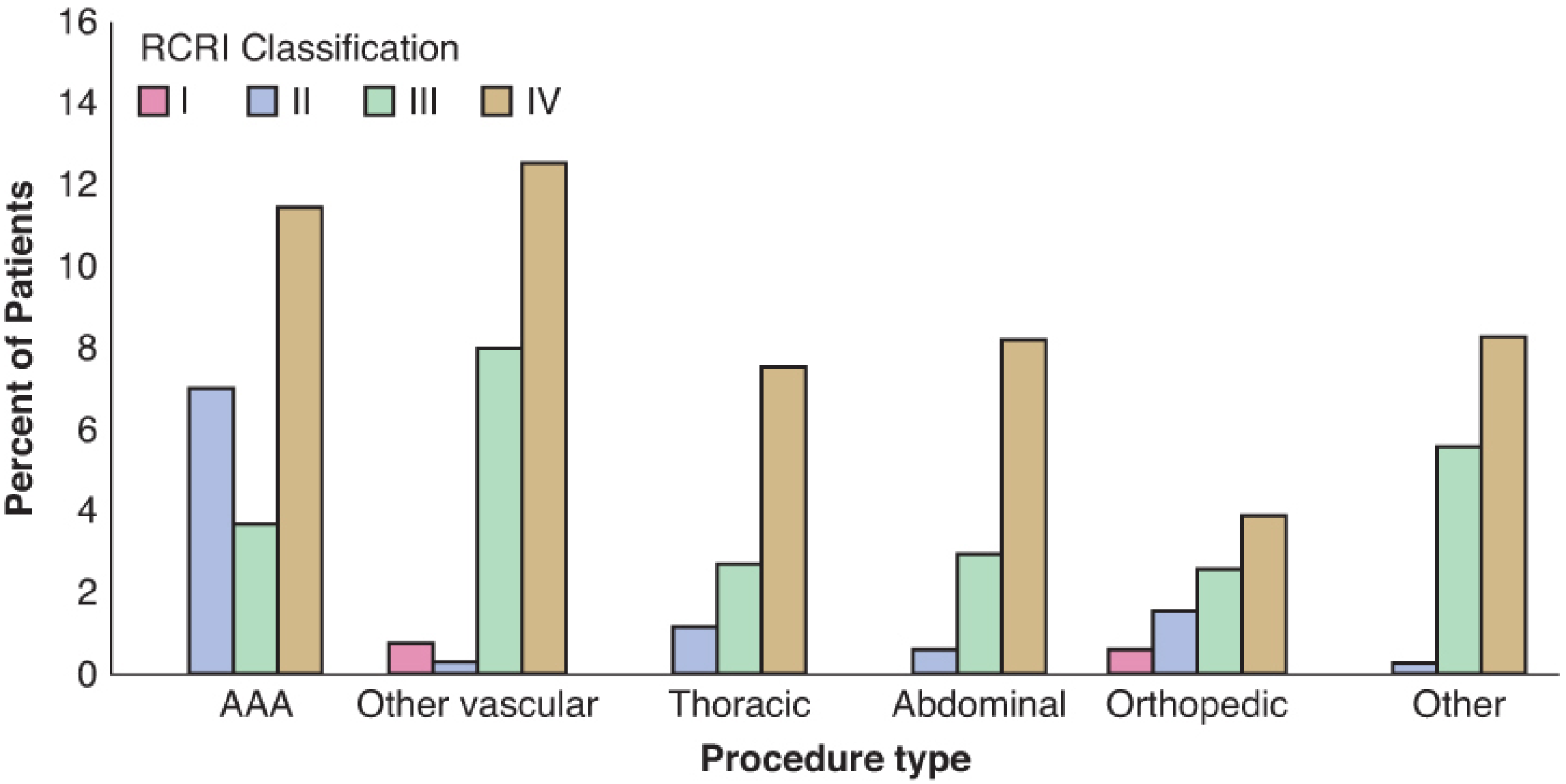
Step 3 - Estimate Perioperative MACE Risk (Surgery-Specific + Clinical Risk)
| Risk Category | Expected MACE | Examples |
|---|---|---|
| Low | <1% | Superficial procedures, cataract, breast, endoscopic, ambulatory |
| Intermediate | 1-5% | Carotid endarterectomy, intraperitoneal, intrathoracic, orthopedic, head & neck, prostate |
| High (Vascular) | >5% | Aortic repair, peripheral vascular revascularization |
The Revised Cardiac Risk Index (RCRI) - Lee's Index
- High-risk type of surgery
- History of ischemic heart disease
- History of congestive heart failure
- History of cerebrovascular disease (TIA/stroke)
- Insulin-dependent diabetes mellitus
- Preoperative serum creatinine ≥2.0 mg/dL
| RCRI Class | Points | Risk of MACE |
|---|---|---|
| I | 0 | ~0.4% |
| II | 1 | ~0.9% |
| III | 2 | ~6.6% |
| IV | ≥3 | ~11% |
Step 4 - Functional Capacity (Metabolic Equivalents - METs)
| METs | Activity | Clinical Significance |
|---|---|---|
| 1 MET | Eating, dressing, desk work | Minimal - severe limitation |
| 4 METs | Climbing 1-2 flights of stairs, walking briskly on flat ground | The critical threshold |
| 7-8 METs | Heavy housework, golf, moderate swimming | Good capacity |
| >10 METs | Strenuous sports (tennis, basketball, squash) | Excellent capacity |
The Full ACC/AHA Decision Algorithm
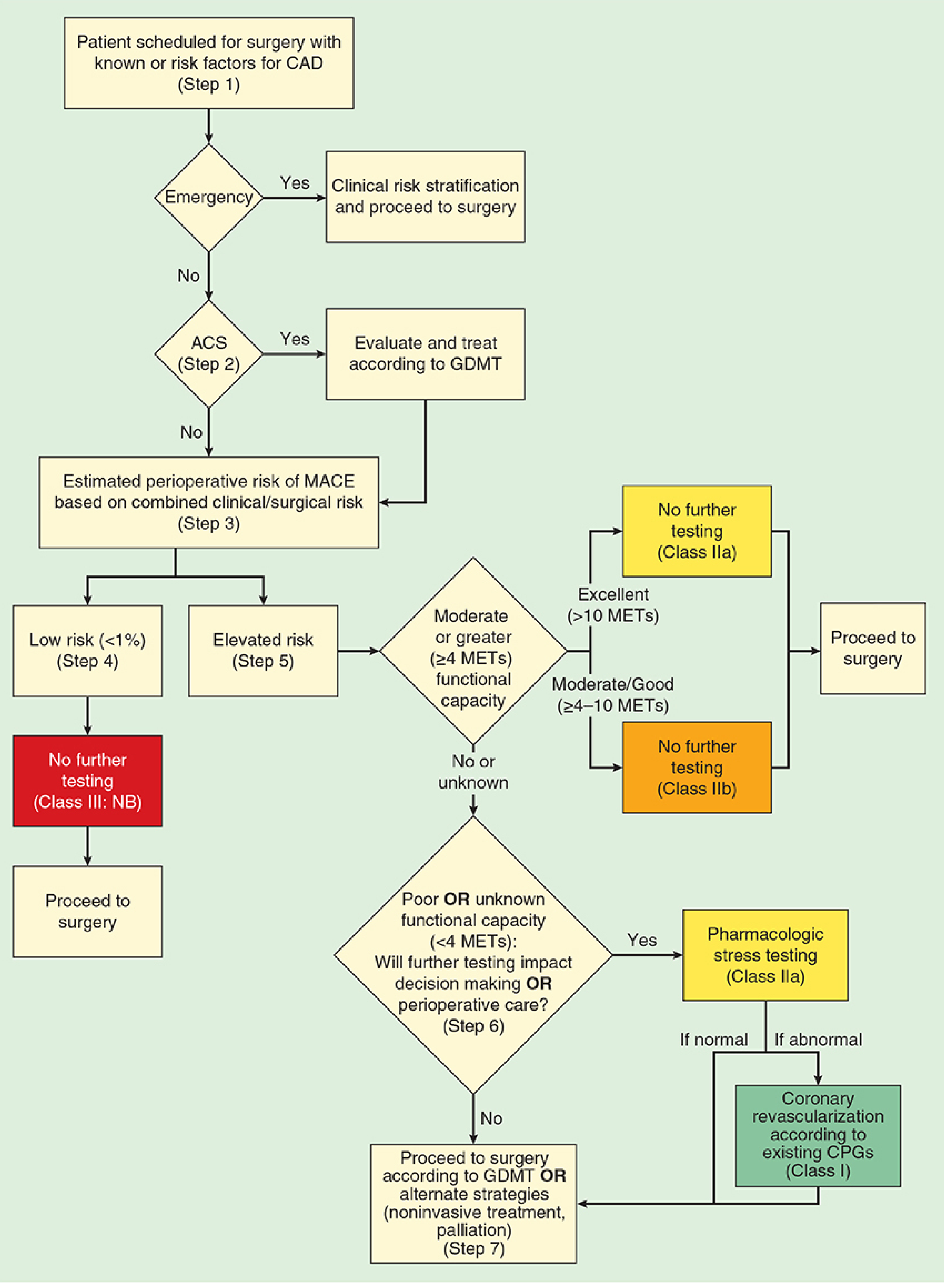
- Emergency? → Proceed, manage clinically
- ACS present? → Cardiology referral, GDMT (STEMI/NSTEMI CPGs)
- Estimate MACE risk (RCRI + surgical risk)
- Low risk (<1%) → No further testing, proceed
- Elevated risk → Go to functional capacity assessment
- Functional capacity ≥4 METs?
- Moderate/good (4-10 METs) → Proceed (Class IIb: no further testing)
- Excellent (>10 METs) → Proceed (Class IIa)
- Poor or unknown (<4 METs) → Question 5
- Will further testing change management?
- Yes → Pharmacologic stress testing (Class IIa). If abnormal → coronary revascularization per existing CPGs
- No → Proceed per GDMT or consider alternate/palliative strategy
Preoperative Testing - When to Order What
- Indicated for patients with known CAD, significant arrhythmia, peripheral artery disease, cerebrovascular disease prior to intermediate/high-risk surgery (Class IIa)
- May be considered in asymptomatic patients before intermediate/high-risk surgery (Class IIb)
- NOT useful in asymptomatic patients before low-risk surgery (Class III)
- If dyspnea of unknown origin
- Known LV dysfunction - if no echo within 1 year or significant functional change
- Reserve for elevated RCRI risk + poor/unknown functional capacity (<4 METs) + testing will change management
- Pharmacologic stress (dobutamine stress echo, nuclear perfusion imaging) when patient cannot exercise
- NOT recommended for low-risk surgery or good functional capacity (>4 METs)
Part 2: Preoperative Medical Optimization
Beta-Blockers - The Most Exam-Relevant Drug
- Continue beta-blockers in patients already receiving chronic therapy - do NOT withdraw (evidence A)
- Never start beta-blockers de novo on the day of surgery
- Consider initiating beta-blockade perioperatively (titrated, well in advance) in very select patients: intermediate/high-risk ischemia on stress testing, OR ≥3 RCRI risk factors
Statins
- Continue existing statin therapy perioperatively (evidence B) - important for plaque stabilization, anti-inflammatory effects
- Initiate statin therapy for patients undergoing vascular surgery (evidence B)
- Multiple trials show reduced perioperative MACE and mortality, especially in vascular surgery
- The LOAD trial showed no benefit from atorvastatin loading in statin-naive patients for non-vascular surgery - so be selective
ACE Inhibitors / ARBs
- Continue for heart failure or hypertension management (maintain RAAS continuity)
- Hold on the morning of surgery if used solely for hypertension - reduces risk of severe intraoperative hypotension
- Resume postoperatively when hemodynamically stable
Aspirin / Antiplatelet Therapy
- Continuing aspirin does NOT prevent cardiovascular complications perioperatively
- BUT does increase major bleeding risk (which is itself a risk factor for perioperative stroke)
- General recommendation: hold aspirin 72 hours before surgery for most patients
- Exception: consider continuing in patients with high-risk atherosclerotic CVD or recent stroke within 9 months
- Most dangerous period: 4-6 weeks post-stent implantation (highest stent thrombosis risk)
- DAPT (Dual Antiplatelet Therapy) duration:
- BMS (bare metal stent): minimum 30 days DAPT before elective surgery
- DES (drug-eluting stent) for stable disease: minimum 6 months DAPT
- DES post-ACS: minimum 12 months DAPT
- Drug washout before surgery: clopidogrel - 5 days; prasugrel - 7 days; ticagrelor - 3-5 days
- If surgery truly cannot be delayed: continue aspirin, discuss with cardiology
Prophylactic Revascularization - A Common Misconception
Part 3: Intraoperative Management
Monitoring
- 5-lead ECG with ST-segment monitoring: leads II (inferior territory), V4 or V5 (anterior/lateral territory - most sensitive for LAD ischemia). Combination of II + V5 detects ~80% of ischemic events
- Arterial line for continuous BP monitoring in moderate/high-risk cases
- Central venous access as indicated
- TEE (transesophageal echocardiography): The most sensitive intraoperative monitor for ischemia - detects new regional wall motion abnormalities (RWMA) before ECG changes or hemodynamic compromise. Gold standard for high-risk cases. (Miller's Anesthesia 10e, p. 3457)
- Pulmonary artery catheter: selected cases with severe LV dysfunction or anticipated major fluid shifts
Anesthetic Goals - The Hemodynamic Targets
| Goal | Rationale |
|---|---|
| Heart rate: 60-80 bpm (or near baseline) | Reduces MVO2; prolongs diastole → improves coronary perfusion |
| Avoid tachycardia | Most dangerous determinant of ischemia - increases demand + decreases supply |
| Maintain diastolic BP | Coronary perfusion pressure depends on diastole |
| Avoid hypotension | MAP <65 mmHg = inadequate coronary perfusion |
| Avoid hypertension | Increased afterload = increased wall stress = increased MVO2 |
| Maintain normothermia | Hypothermia → shivering → catecholamine surge → tachycardia |
Choice of Anesthetic Technique
Intraoperative Ischemia - Recognition and Treatment
- ST depression >1 mm in two contiguous leads (subendocardial ischemia - most common pattern)
- ST elevation (transmural ischemia - more alarming)
- New T-wave inversions
- New LBBB
| Clinical Manifestation | Intervention |
|---|---|
| ↑ Heart rate (increased demand) | Beta-blocker IV, ↑ anesthetic depth |
| ↑ Blood pressure (increased demand) | ↑ anesthetic depth, nitroglycerin, labetalol |
| ↑ PCWP (increased demand) | Nitroglycerin |
| ↓ Heart rate (decreased supply) | Atropine, pacing |
| ↓ Blood pressure (decreased supply) | ↓ anesthetic depth, vasoconstrictors (phenylephrine/norepinephrine) |
| ↑ PCWP with low supply | Nitroglycerin + inotrope |
| No hemodynamic changes | Nitroglycerin, calcium channel blockers, consider heparin |
- Drug of choice for acute intraoperative ischemia
- Works via systemic venodilation (↓ preload, ↓ LVEDP) + coronary arterial dilation including collateral beds
- Effective at stenosed coronaries
- Caution: Higher doses cause systemic hypotension → reflex tachycardia → worsens ischemia
- Prophylactic nitroglycerin infusion does NOT prevent intraoperative ischemia or reduce cardiac complications
- Side effect at high/prolonged doses: methemoglobinemia
Part 4: Postoperative Management
High-Risk Period
- Plaque rupture + thrombosis (most common - similar to spontaneous ACS)
- Demand ischemia from tachycardia, hypotension, pain, anemia, hypoxia
Postoperative Monitoring
- Routine ECGs and troponins are NOT recommended in all patients
- In high cardiac risk patients: the benefit of routine troponin/ECG surveillance remains uncertain
- Any symptomatic event (chest pain, new hemodynamic instability, new arrhythmia, hypoxia): obtain ECG and troponin immediately and treat as ACS
Postoperative Treatment
- Treat as standard ACS protocol
- Key caveat: Bleeding risk from anticoagulants must be carefully weighed against thrombotic risk given recent surgery
- Dual antiplatelet therapy decisions require surgical team input regarding bleeding risk
- Urgent cardiology consultation
- Consider coronary angiography/PCI timing based on clinical stability and surgical bleeding risk
Continue Chronic Medications
- Resume beta-blockers, statins, ACE inhibitors/ARBs postoperatively as soon as patient is hemodynamically stable and tolerating oral medications
- Abrupt beta-blocker withdrawal perioperatively is associated with rebound tachycardia, hypertension, and ischemia
Summary Table for Exam Revision
| Phase | Key Actions |
|---|---|
| Preoperative | Urgency? → Active conditions? → MACE risk (RCRI + surgery) → METs → Further testing if needed |
| Medications | Continue: beta-blockers, statins. Hold morning-of or titrate: ACE-i/ARB. Antiplatelet: per stent type/indication |
| Stent patients | BMS: delay ≥30 days. DES: delay ≥6 months (stable) or 12 months (post-ACS) |
| Intraoperative | 5-lead ECG (II+V5), arterial line, consider TEE. Target HR 60-80, maintain MAP, avoid tachycardia |
| Ischemia Rx | Treat by mechanism: demand (beta-blocker, ↑ depth) vs. supply (vasopressor, ↓ depth, pacing) + nitroglycerin |
| Postoperative | Peak risk 0-72h. Silent MIs common. Routine troponin not mandatory. Treat symptoms as ACS. Resume meds early. |
Exam Hot Tips
- The single most important intraoperative monitor for ischemia = TEE (wall motion abnormalities precede ECG changes)
- Tachycardia is the most dangerous hemodynamic derangement in ischemic heart disease - it both increases demand AND decreases supply
- POISE trial lesson = high-dose perioperative beta-blocker initiation reduces MI but increases stroke and death; always titrate slowly in advance
- Prophylactic revascularization before noncardiac surgery is NOT indicated (CARP trial)
- <4 METs = poor functional capacity = increased perioperative cardiac risk
- Nitroglycerin prophylaxis infusion = does NOT prevent intraoperative ischemia
- DES stent = minimum 6 months (stable) or 12 months (post-ACS) before elective surgery to complete DAPT
- Most perioperative MIs are silent - don't wait for chest pain postoperatively in a sedated patient
cardiac arrest in ot - causes with recent guidelines - act like professor in anesthesia and explain it to resident with viva questions
"cardiac arrest" AND "operating room" AND "perioperative"
PMID: 37218626
Cardiac Arrest in the Operating Theatre - A Professor's Teaching Lecture for MD Final Viva
Section 1: Epidemiology and Why the OT is Unique
- Cardiac arrest occurs in approximately 1 in every 10,000 anesthetics when the cause is anesthesia-related
- Data from the ACS NSQIP database shows a broader incidence - 1 in every 203 surgical patients - with over 70% dying within one month
- When cardiac arrest is purely anesthesia-related, successful resuscitation occurs approximately 90% of the time
- Overall in-hospital survival to discharge is ~25% for perioperative cardiac arrest
- The patient is already fully monitored - you see it the moment it happens
- There is immediate expert personnel present
- All resuscitation equipment is at hand - defibrillator, drugs, airway
Section 2: Classification of Causes - The "ANESTHESIA + H's & T's" Framework
- Anesthesia/surgery-specific causes (unique to OT)
- General ACLS causes (H's and T's - same as anywhere else)
Stream A: OT-Specific Causes (The Examiner's Favorites)
1. Airway Catastrophe - Hypoxia from Failed Intubation / Oesophageal Intubation
2. Drug-Related Causes
- Epinephrine IV is the first-line drug - 0.1-0.5 mg (1:10,000) IV boluses, escalating as needed. NOT just IM.
- Stop the trigger
- Aggressive IV fluids (1-2 L rapid)
- Bronchodilators (salbutamol nebulized or IV)
- Antihistamines and corticosteroids are secondary
- Stop injection immediately
- Airway management, 100% O2, IV access
- Seizures: benzodiazepine (NOT propofol - cardiovascular depression)
- 20% Lipid Emulsion (Intralipid) - the specific antidote:
- Bolus: 1.5 mL/kg over 1 minute
- Infusion: 0.25 mL/kg/min
- Repeat bolus every 3-5 min if no response
- Maximum total dose: 10 mL/kg over first 30 minutes
- For cardiac arrest: standard ACLS + lipid emulsion
- Avoid propofol as lipid emulsion substitute (insufficient lipid load, adds cardiac depression)
3. Total Spinal / High Spinal Anesthesia
- Hand/arm tingling (cervical root involvement)
- Intercostal paralysis
- Diaphragm paralysis (C3-5)
- Apnea + LOC (brainstem)
- Cardiac arrest
- 100% O2, secure airway (intubate)
- Vasopressors (epinephrine/phenylephrine IV) for hypotension
- Atropine/epinephrine for bradycardia
- Psychological support and reassurance (patient may be conscious initially)
- Block resolves with time - generally recovers fully
4. Malignant Hyperthermia (MH)
- Stop trigger agents immediately
- Call for help + MH hotline
- Dantrolene 2.5 mg/kg IV rapidly, repeat until ETCO2 falls (continue until crisis resolves, up to 10 mg/kg or more)
- 100% O2 at high flows to wash out volatile agents
- Active cooling (cold IV fluids, ice packs, cooled lavage)
- Treat hyperkalemia aggressively (cardiac arrest from K+ is a major risk)
- Bicarbonate for severe acidosis
- Continue surgery only if life-threatening
5. Venous Air Embolism (VAE)
- Flood surgical field / stop air entry
- Aspirate via right heart/CVP catheter
- Place patient left lateral decubitus + Trendelenburg (Durant maneuver) - moves air bubble away from right ventricular outflow tract
- 100% O2 to dissolve air (NO nitrous oxide - it expands air bubble)
- CPR if arrest occurs - chest compressions may fragment large bolus
6. Tension Pneumothorax
7. Cardiac Tamponade
8. Acute Coronary Syndrome / Massive MI
Stream B: The H's and T's (AHA 2020 ACLS Guidelines)
| H's | T's |
|---|---|
| Hypovolemia - massive hemorrhage | Tension pneumothorax |
| Hypoxia - airway failure, aspiration | Tamponade (cardiac) |
| Hydrogen ion (Acidosis) | Toxins - drugs, local anesthetics |
| Hypo/Hyperkalemia | Thrombosis, pulmonary (massive PE) |
| Hypothermia - cold irrigation, prolonged surgery | Thrombosis, coronary (MI) |
| Hypoglycemia |
Section 3: Recognition in the OT
- SpO2 waveform loss (first sign often)
- ETCO2 sudden drop to zero (no cardiac output = no CO2 delivery to lungs)
- Arterial line trace goes flat
- ECG: VF, pulseless VT, asystole, PEA
- Surgical field: sudden "empty" vessels, no bleeding
- During good CPR, ETCO2 should be >10 mmHg
- ETCO2 >40 mmHg during CPR = very likely ROSC
- Helps guide compression quality without interrupting CPR
Section 4: The OT Cardiac Arrest Algorithm - 2020 AHA / 2023 ESAIC-ESTES
Immediate Response (First 30 seconds)
- Call for help - designate team leader immediately
- Confirm cardiac arrest - pulse check <10 seconds
- Start high-quality CPR - 30:2 if not intubated; continuous compressions if intubated
- Apply defibrillator pads
- Assess rhythm
CPR Quality Standards (2020 AHA)
| Parameter | Target |
|---|---|
| Rate | 100-120 compressions/min |
| Depth | 5-6 cm sternum depression |
| Recoil | Full chest recoil (no leaning) |
| Interruptions | Minimize - <10 sec pause |
| Ventilation (intubated) | 1 breath every 6 seconds (10/min) |
| Ventilation rate | DO NOT over-ventilate - increases intrathoracic pressure, reduces venous return |
Shockable vs. Non-Shockable Rhythms
- Shock immediately: Biphasic 120-200J, monophasic 360J
- Resume CPR immediately after shock (do NOT check pulse first)
- Epinephrine 1 mg IV every 3-5 minutes (after 2nd shock)
- Amiodarone 300 mg IV bolus (after 3rd shock) - for refractory VF/VT
- Internal defibrillation (open chest): 10-50J if chest is open
- CPR immediately
- Epinephrine 1 mg IV as soon as possible, then every 3-5 minutes
- Identify and treat H's and T's
- Atropine: NOT recommended for asystole/PEA (insufficient evidence, not harmful but not helpful)
- All benefit comes from alpha-adrenergic vasoconstriction
- Increases aortic diastolic pressure → increases coronary perfusion pressure → improves myocardial blood flow
- Beta effects are actually detrimental (increase post-ROSC arrhythmias and O2 demand)
Section 5: OT-Specific Modifications to Standard ACLS
-
Airway advantage: The anesthesiologist can maintain a definitive airway immediately - use it. Continuous capnography during CPR is essential.
-
Open Chest Cardiac Massage (OCCM): In cardiac surgery cases or when chest is already open - internal cardiac massage is far more efficient than external compressions (generates higher cardiac output). Use internal paddles for defibrillation starting at 10J.
-
Position: External CPR in prone-positioned patients - place pads at T7 and right shoulder; compressions at same location as standard. Do NOT routinely reposition prone patients unless compressions are completely ineffective.
-
Drug delivery: Intraosseous (IO) access - humeral IO is rapid and allows 100 mL/min flow. If no IV access, use IO. Do NOT use endotracheal route as primary route.
-
TEE: Provides real-time diagnosis of cause (wall motion abnormality, pericardial effusion, RV failure, PE) without interrupting compressions. Gold standard for intraoperative diagnosis.
-
Surgical control of hemorrhage: If cardiac arrest is due to surgical hemorrhage, surgical hemostasis takes priority alongside CPR.
-
REBOA (Resuscitative Endovascular Balloon Occlusion of the Aorta): In select trauma cases, can temporize hemorrhagic cardiac arrest by occluding descending aorta - complex, requires specific training and infrastructure.
Section 6: Drugs in OT Cardiac Arrest - Quick Reference
| Drug | Dose | Indication |
|---|---|---|
| Epinephrine | 1 mg IV every 3-5 min | VF, PEA, Asystole - ALL rhythms |
| Amiodarone | 300 mg IV bolus, then 150 mg | Refractory VF/VT (after 3rd shock) |
| Lidocaine | 1-1.5 mg/kg IV | Alternate to amiodarone if not available |
| Atropine | NOT recommended in arrest | No benefit in asystole/PEA |
| Calcium gluconate | 10-20 mL of 10% IV | Hyperkalemia, hypocalcemia, Ca-channel blocker OD |
| Sodium bicarbonate | 1 mEq/kg IV | Hyperkalemia, tricyclic antidepressant OD, severe acidosis >10 min arrest |
| Dantrolene | 2.5 mg/kg IV bolus | Malignant hyperthermia |
| 20% Lipid emulsion | 1.5 mL/kg bolus then 0.25 mL/kg/min | LAST (local anesthetic toxicity) |
| Magnesium sulfate | 1-2 g IV | Torsades de pointes, hypomagnesemia |
| Vasopressin | 40 units IV (single dose) | Can replace 1st or 2nd dose of epinephrine |
Section 7: Post-Resuscitation Care (Post-ROSC)
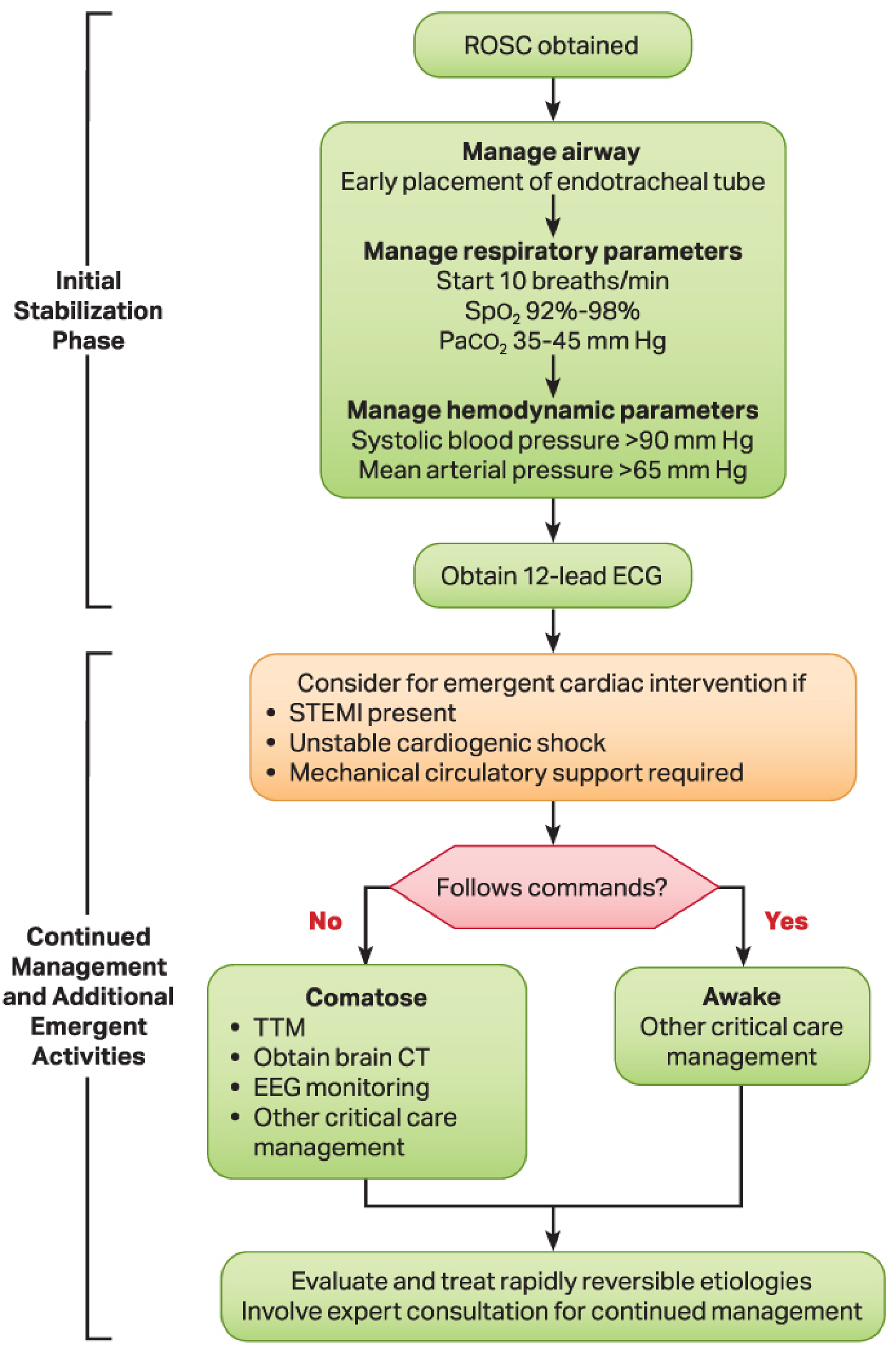
Initial Stabilization Phase:
- Secure airway with ETT + confirm with waveform capnography
- Ventilate at 10 breaths/min (start)
- Titrate FiO2: SpO2 92-98% (avoid hyperoxia - generates free radicals)
- Titrate ventilation: PaCO2 35-45 mmHg (avoid hypocapnia - causes cerebral vasoconstriction)
- Systolic BP >90 mmHg, MAP >65 mmHg
- Vasopressors/inotropes as needed
Continued Management:
- If patient is comatose (not following commands) after ROSC → TTM at 32-36°C for 24 hours
- Prevents secondary neurological injury from reperfusion
- Use cooling device with feedback loop
- Monitor core temperature continuously (esophageal, rectal, bladder)
- TTM + EEG monitoring + brain CT are all part of the comatose post-arrest bundle
- Maintain normoglycemia (hyperglycemia worsens neurological outcome)
- Continuous or intermittent EEG (detect subclinical seizures)
- Lung-protective ventilation
- Avoid hyperthermia after TTM completion
Section 8: DNAR Orders in the OT
- Up to 60% of anesthesiologists mistakenly believe DNAR orders are automatically suspended in the OT
- This is legally and ethically wrong - advance directives are binding
- ASA, American College of Surgeons, AORN, and The Joint Commission all require reconsideration, not abandonment, of DNAR in the perioperative period
- The discussion must occur preoperatively, must be documented, and must be shared with the full OT team
- Families have successfully sued for damages when DNAR instructions were ignored
Section 9: Prevention - The Anesthesiologist's Priority
| Prevention Strategy | Target |
|---|---|
| Capnography monitoring | Detect oesophageal intubation, monitor CPR quality |
| Difficult airway algorithm preparation | Avoid CICO situation |
| Test dose in regional anesthesia | Detect intravascular injection (LAST) |
| Incremental local anesthetic injection | Limit LAST risk |
| Avoid succinylcholine in at-risk patients | Prevent hyperkalemic arrest |
| MH triggering agent avoidance (susceptible patients) | Prevent MH crisis |
| Dantrolene stocked within OR | MH emergency readiness |
| Regular simulation and drill practice | Team performance in crisis |
| Crew Resource Management (CRM) | Communication errors reduced |
| Cognitive aids / checklists | Stanford Emergency Manuals in every OT |
VIVA QUESTIONS - Rapid Fire
Approximately 1 in 10,000 anesthetics when purely anesthesia-related; 1 in 203 surgical patients in the broader NSQIP database.
Because patients are already fully monitored, arrest is recognized immediately, expert personnel are present, and all resuscitation equipment is immediately available. When anesthesia-related, ROSC approaches 90%.
H's: Hypovolemia, Hypoxia, Hydrogen ion (acidosis), Hypo/Hyperkalemia, Hypothermia, Hypoglycemia. T's: Tension pneumothorax, Tamponade, Toxins, Thrombosis-pulmonary, Thrombosis-coronary.
Epinephrine 1 mg IV every 3-5 minutes. Its benefit is entirely through alpha-adrenergic vasoconstriction - increases aortic diastolic pressure → raises coronary perfusion pressure → improves myocardial blood flow. Beta effects are not beneficial during arrest.
Tension pneumothorax. Stop ventilation briefly to confirm, immediately perform needle decompression at 2nd intercostal space, midclavicular line, followed by intercostal tube thoracostomy. Do NOT wait for CXR in haemodynamic compromise.
Succinylcholine-induced hyperkalemia. Upregulation of extrajunctional acetylcholine receptors causes massive K+ efflux. Treatment: standard CPR, calcium gluconate 10 mL IV (membrane stabilization), insulin + dextrose, sodium bicarbonate. Avoid succinylcholine in any patient with >4 days of denervation, burns, prolonged immobilization, or critical illness.
LAST - Local Anesthetic Systemic Toxicity. Specific treatment is 20% lipid emulsion: 1.5 mL/kg bolus over 1 minute → infusion at 0.25 mL/kg/min. Repeat bolus every 3-5 min. Maximum 10 mL/kg over 30 min. Standard ACLS simultaneously. Avoid propofol as a substitute - it adds cardiovascular depression and the lipid concentration is insufficient.
Unexplained tachycardia + rising ETCO2 (most important early sign) + masseter spasm (after succinylcholine) + metabolic acidosis + hyperkalemia + hyperthermia (late). Specific treatment: Dantrolene 2.5 mg/kg IV bolus (repeat until ETCO2 falls), plus stop triggers, active cooling, treat hyperkalemia. Dantrolene prevents Ca2+ release from sarcoplasmic reticulum by blocking RYR1 channels.
Single biphasic shock (120-200J; manufacturer-specific) → immediate CPR resumption (do NOT pulse check) → 2 minutes CPR → rhythm check. If VF persists: shock → CPR. Epinephrine 1 mg IV after 2nd shock. Amiodarone 300 mg IV after 3rd shock. Internal defibrillation (open chest): start at 10J, increase as needed.
After the 3rd failed defibrillation attempt in refractory VF or pulseless VT. Dose: 300 mg IV rapid bolus during arrest, then 150 mg supplements as needed. Maximum 2g/day. It improves survival to hospital admission (3 randomized trials) but has not shown survival to discharge benefit. Lidocaine 1-1.5 mg/kg is the alternative if amiodarone is unavailable.
The ABCDE approach: (A) Oesophageal intubation / tube displacement, (B) Circuit disconnection, (C) Cardiac arrest / massive pulmonary embolism (no blood reaching lungs), (D) Massive air embolism. First check patient (is pulse present?), check airway, check circuit. ETCO2 also correlates with CPR quality - a rising ETCO2 during CPR indicates improving cardiac output.
Per 2023 ESAIC guidelines: place defibrillator pads at T7 (posterior) and right shoulder (anterior). Compressions are applied at the same position as standard (lower third of sternum against the table). Do not routinely turn the patient supine unless compressions are definitively ineffective - repositioning wastes critical time.
Targeted Temperature Management at 32-36°C for 24 hours in comatose patients (those not following commands) after ROSC. Reduces secondary neurological injury from reperfusion. Do NOT allow hyperthermia. Monitor temperature continuously. Accompany with EEG monitoring (detect subclinical seizures), brain CT, and normoglycemia. Neuroprognostication should not occur before 48-72 hours post-arrest.
No. This is a common misconception - 60% of anesthesiologists erroneously believe this. DNAR must be reconsidered, not abandoned in the perioperative period. Anesthesiologist must discuss with patient, document the agreement, and communicate with the full OT team preoperatively. Advance directives are legally binding. Courts have awarded damages when DNAR was overridden without consent.
TEE is the gold standard intraoperative diagnostic tool during cardiac arrest. It can identify: new RWMA (myocardial infarction), pericardial effusion/tamponade, right heart failure (PE), hypovolemia (empty heart), massive air embolism, and the adequacy of compressions - all without interrupting CPR. The 2023 ESAIC guidelines support its use in the OT setting.
Summary Framework for Exam
Cardiac Arrest in OT
│
├── RECOGNIZE (< 10 sec): Monitor loss, no pulse
│
├── CALL FOR HELP + START CPR (100-120/min, 5-6 cm)
│
├── DEFIBRILLATOR ON → Shockable? → Shock + CPR
│ ↓ Non-shockable?
│ CPR + Epinephrine
│
├── FIX THE CAUSE (H's & T's + OT-specific)
│ ├── Airway failure → Reoxygenate, eFONA
│ ├── Anaphylaxis → Epinephrine IV + fluids
│ ├── LAST → Lipid emulsion 20%
│ ├── Total spinal → Airway + vasopressors
│ ├── MH → Dantrolene + cooling
│ ├── VAE → Durant maneuver + O2
│ ├── Tension PTx → Needle decompression
│ ├── Tamponade → Pericardiocentesis
│ └── Hyperkalemia → Ca2+, bicarb, insulin
│
└── POST-ROSC → TTM (if comatose), STEMI? → Cath lab
SpO2 92-98%, PaCO2 35-45, MAP >65
- Barash's Clinical Anesthesia 9e, Chapter 58 (pp. 4896-4948)
- Miller's Anesthesia 10e (pp. 634, 6127, 1973)
- Hinkelbein J et al. "Cardiac arrest in the perioperative period: a consensus guideline." Eur J Anaesthesiol. 2023 Oct (PMID: 37218626) - ESAIC/ESTES Practice Guideline
- AHA 2020 Guidelines for CPR and ECC (Circulation. 2020;142:S366-S468)
- ASRA Local Anesthetic Systemic Toxicity Checklist (2020)
- Morgan & Mikhail's Clinical Anesthesiology 7e
create me a ppt on differences between the 10th edition millers anaesthesia textbook to 9th ed millers - and explain to me the changes with reasons
Miller's Anesthesia 10th edition vs 9th edition new chapters changes updates 2025
https://inspectioncopy.elsevier.com/book/details/97803239359…
Miller's Anesthesia 9th edition table of contents chapters list Gropper 2020
https://www.us.elsevierhealth.com/millers-anesthesia-2-volum…
https://shop.elsevier.com/books/millers-anesthesia-2-volume-…
mkdir -p /home/daytona/workspace/millers-pptx && ls /home/daytona/workspace/millers-pptx/
~/millers-pptx/build.js
const pptxgen = require("pptxgenjs");
const pres = new pptxgen();
pres.layout = "LAYOUT_WIDE"; // 13.3" x 7.5"
pres.title = "Miller's Anesthesia: 10th vs 9th Edition - Key Changes";
pres.author = "Orris Medical Education";
// ─── COLOUR PALETTE ───────────────────────────────────────────────────────────
const C = {
navy: "0A1628", // dominant dark
blue: "1565C0", // primary accent
teal: "00838F", // secondary accent
gold: "F9A825", // highlight accent
white: "FFFFFF",
ltgray: "F0F4F8",
midgray: "90A4AE",
darkgray:"37474F",
green: "2E7D32",
red: "B71C1C",
orange: "E65100",
purple: "6A1B9A",
};
// ─── HELPERS ──────────────────────────────────────────────────────────────────
function titleSlide(title, subtitle) {
const s = pres.addSlide();
// full dark background
s.addShape(pres.ShapeType.rect, { x:0, y:0, w:"100%", h:"100%", fill:{color:C.navy} });
// gold accent bar
s.addShape(pres.ShapeType.rect, { x:0, y:0, w:0.08, h:"100%", fill:{color:C.gold} });
// decorative horizontal rule
s.addShape(pres.ShapeType.rect, { x:0.5, y:4.1, w:12.3, h:0.04, fill:{color:C.gold} });
// "MILLER'S ANESTHESIA" label
s.addText("MILLER'S ANESTHESIA", {
x:0.6, y:0.9, w:12, h:0.6,
fontSize:13, bold:true, color:C.gold, fontFace:"Calibri", charSpacing:8,
});
// main title
s.addText(title, {
x:0.6, y:1.5, w:12, h:2.2,
fontSize:44, bold:true, color:C.white, fontFace:"Calibri", lineSpacingMultiple:1.1,
});
// subtitle
s.addText(subtitle, {
x:0.6, y:4.3, w:12, h:0.7,
fontSize:22, color:C.midgray, fontFace:"Calibri", italic:true,
});
// edition badges
s.addShape(pres.ShapeType.roundRect, { x:0.6, y:5.4, w:2.8, h:0.7, fill:{color:C.red}, rectRadius:0.1 });
s.addText("9th Edition 2019", { x:0.6, y:5.4, w:2.8, h:0.7, fontSize:14, bold:true, color:C.white, align:"center", valign:"middle" });
s.addShape(pres.ShapeType.rect, { x:3.6, y:5.6, w:1.0, h:0.25, fill:{color:C.gold} });
s.addText("→", { x:4.2, y:5.35, w:0.6, h:0.8, fontSize:30, color:C.gold, align:"center", valign:"middle" });
s.addShape(pres.ShapeType.roundRect, { x:5.0, y:5.4, w:2.8, h:0.7, fill:{color:C.green}, rectRadius:0.1 });
s.addText("10th Edition 2024", { x:5.0, y:5.4, w:2.8, h:0.7, fontSize:14, bold:true, color:C.white, align:"center", valign:"middle" });
// footer
s.addText("A comprehensive comparison for residents & anesthesiologists", {
x:0.6, y:6.7, w:12, h:0.5, fontSize:11, color:C.midgray, fontFace:"Calibri", italic:true,
});
return s;
}
function sectionDivider(sectionNum, sectionTitle, subtitle) {
const s = pres.addSlide();
s.addShape(pres.ShapeType.rect, { x:0, y:0, w:"100%", h:"100%", fill:{color:C.blue} });
s.addShape(pres.ShapeType.rect, { x:0, y:0, w:"100%", h:0.08, fill:{color:C.gold} });
s.addShape(pres.ShapeType.rect, { x:0, y:7.42, w:"100%", h:0.08, fill:{color:C.gold} });
// section number
s.addText(`SECTION ${sectionNum}`, {
x:0.6, y:1.2, w:12, h:0.6,
fontSize:13, bold:true, color:C.gold, fontFace:"Calibri", charSpacing:8,
});
s.addText(sectionTitle, {
x:0.6, y:1.9, w:12, h:2.0,
fontSize:42, bold:true, color:C.white, fontFace:"Calibri",
});
s.addShape(pres.ShapeType.rect, { x:0.6, y:4.2, w:3.5, h:0.05, fill:{color:C.gold} });
s.addText(subtitle, {
x:0.6, y:4.5, w:11, h:0.8,
fontSize:18, color:"D1E8FF", fontFace:"Calibri", italic:true,
});
return s;
}
function contentSlide(title, accentColor, items, notes) {
// items: array of {label, text, color?} OR array of strings for bullets
const s = pres.addSlide();
// light background
s.addShape(pres.ShapeType.rect, { x:0, y:0, w:"100%", h:"100%", fill:{color:C.ltgray} });
// left accent bar
s.addShape(pres.ShapeType.rect, { x:0, y:0, w:0.06, h:"100%", fill:{color:accentColor} });
// title bar
s.addShape(pres.ShapeType.rect, { x:0, y:0, w:"100%", h:1.1, fill:{color:accentColor} });
s.addText(title, {
x:0.25, y:0.08, w:12.8, h:0.9,
fontSize:26, bold:true, color:C.white, fontFace:"Calibri", valign:"middle", margin:0,
});
// content area
if (notes) {
s.addText(notes, {
x:0.25, y:6.7, w:13, h:0.55,
fontSize:10, color:C.midgray, fontFace:"Calibri", italic:true,
});
}
return s;
}
function addBulletBox(slide, x, y, w, h, title, bullets, titleColor, bgColor) {
slide.addShape(pres.ShapeType.roundRect, { x, y, w, h, fill:{color:bgColor||C.white}, line:{color:C.midgray, width:0.5}, rectRadius:0.12 });
slide.addText(title, {
x:x+0.12, y:y+0.06, w:w-0.24, h:0.38,
fontSize:13, bold:true, color:titleColor||C.blue, fontFace:"Calibri", margin:0,
});
const bulletItems = bullets.map((b,i) => ({
text: b,
options: { bullet:true, breakLine: i < bullets.length-1, fontSize:11.5, color:C.darkgray, fontFace:"Calibri" }
}));
slide.addText(bulletItems, {
x:x+0.12, y:y+0.48, w:w-0.24, h:h-0.58,
fontFace:"Calibri",
});
}
function compareBoxes(slide, leftTitle, leftItems, rightTitle, rightItems, leftColor, rightColor) {
// VS layout: left half = old, right half = new
addBulletBox(slide, 0.25, 1.25, 6.1, 5.8, `9th Ed — ${leftTitle}`, leftItems, leftColor||C.red, C.white);
addBulletBox(slide, 6.95, 1.25, 6.1, 5.8, `10th Ed — ${rightTitle}`, rightItems, rightColor||C.green, C.white);
// arrow between
slide.addText("➜", { x:6.15, y:3.7, w:0.7, h:0.8, fontSize:28, color:C.gold, align:"center", valign:"middle" });
}
// ══════════════════════════════════════════════════════════════════════════════
// SLIDE 1 — TITLE
// ══════════════════════════════════════════════════════════════════════════════
titleSlide(
"10th vs 9th Edition\nKey Changes & Why They Matter",
"A Structured Comparison for Residents, Trainees & Attendings"
);
// ══════════════════════════════════════════════════════════════════════════════
// SLIDE 2 — OVERVIEW AT-A-GLANCE
// ══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.ShapeType.rect, { x:0, y:0, w:"100%", h:"100%", fill:{color:C.navy} });
s.addShape(pres.ShapeType.rect, { x:0, y:0, w:0.06, h:"100%", fill:{color:C.gold} });
s.addText("AT A GLANCE — SIDE BY SIDE", {
x:0.25, y:0.12, w:13, h:0.7,
fontSize:22, bold:true, color:C.gold, fontFace:"Calibri", charSpacing:4,
});
// left panel
s.addShape(pres.ShapeType.roundRect, { x:0.25, y:1.0, w:6.1, h:6.0, fill:{color:"1A2744"}, rectRadius:0.15 });
s.addShape(pres.ShapeType.roundRect, { x:0.35, y:1.0, w:6.0, h:0.5, fill:{color:C.red}, rectRadius:0.1 });
s.addText("9th EDITION (2019)", { x:0.35, y:1.0, w:6.0, h:0.5, fontSize:15, bold:true, color:C.white, align:"center", valign:"middle" });
const col9 = [
"Published: 2019",
"Editors: Gropper, Miller, Eriksson, Fleisher,\n Wiener-Kronish, Cohen, Leslie",
"Total Chapters: ~90 chapters",
"4 New Chapters (vs 8th ed):",
" • Extreme Environments (High/Low Pressure)",
" • Immediate & Long-Term Complications",
" • Clinical Research",
" • Interpreting Medical Literature",
"Focus: neurotoxicity, palliation,\n sleep/wake disorders",
"Echocardiography: Ch 37 (standard echo only)",
"No dedicated Immune System chapter",
"No Emergency Preparedness chapter",
"Streamlined several topics vs 8th ed",
];
const col9Items = col9.map((t,i)=>({text:t, options:{bullet:i>2&&i<9, breakLine:i<col9.length-1, fontSize:11.5, color:i===0||i===1||i===2?C.gold:C.white, bold:i===0||i===2, fontFace:"Calibri"}}));
s.addText(col9Items, { x:0.45, y:1.62, w:5.8, h:5.2, fontFace:"Calibri" });
// right panel
s.addShape(pres.ShapeType.roundRect, { x:6.95, y:1.0, w:6.1, h:6.0, fill:{color:"1A2744"}, rectRadius:0.15 });
s.addShape(pres.ShapeType.roundRect, { x:7.05, y:1.0, w:6.0, h:0.5, fill:{color:C.green}, rectRadius:0.1 });
s.addText("10th EDITION (2024)", { x:7.05, y:1.0, w:6.0, h:0.5, fontSize:15, bold:true, color:C.white, align:"center", valign:"middle" });
const col10 = [
"Published: 2024",
"Editors: Gropper, Eriksson, Fleisher, Cohen,\n Leslie + New: Oluwaseun Johnson-Akeju",
"Total Chapters: ~87 chapters",
"2 Brand-New Chapters:",
" • Immune System & Anesthetic Management",
" • Emergency Preparedness in Healthcare",
"Major Expansions:",
" • POCUS (point-of-care ultrasound)",
" • COVID-19 & infection control protocols",
" • Sustainability in anesthesia",
" • Global health equity",
" • Pediatric / neonatal / congenital cardiac",
" • Perioperative neurocognitive disorders",
"New section structure: more logical flow",
];
const col10Items = col10.map((t,i)=>({text:t, options:{bullet:i>2&&i<14, breakLine:i<col10.length-1, fontSize:11.5, color:i===0||i===1||i===2?C.gold:C.white, bold:i===0||i===2||i===6, fontFace:"Calibri"}}));
s.addText(col10Items, { x:7.1, y:1.62, w:5.8, h:5.2, fontFace:"Calibri" });
// vs badge
s.addShape(pres.ShapeType.roundRect, { x:6.3, y:3.7, w:0.72, h:0.72, fill:{color:C.gold}, rectRadius:0.36 });
s.addText("VS", { x:6.3, y:3.7, w:0.72, h:0.72, fontSize:16, bold:true, color:C.navy, align:"center", valign:"middle" });
}
// ══════════════════════════════════════════════════════════════════════════════
// SECTION 1 — NEW CHAPTERS
// ══════════════════════════════════════════════════════════════════════════════
sectionDivider(1, "Brand-New Chapters", "Two entirely new chapters added to the 10th edition — reflecting the evolution of the specialty");
// Slide: New Chapter 1 — Immune System
{
const s = pres.addSlide();
s.addShape(pres.ShapeType.rect, { x:0, y:0, w:"100%", h:"100%", fill:{color:C.ltgray} });
s.addShape(pres.ShapeType.rect, { x:0, y:0, w:"100%", h:1.15, fill:{color:C.purple} });
s.addShape(pres.ShapeType.rect, { x:0, y:0, w:0.06, h:"100%", fill:{color:C.purple} });
s.addText("NEW CHAPTER | Chapter 26", { x:0.25, y:0.05, w:13, h:0.35, fontSize:12, color:"D1C4E9", bold:true, charSpacing:5, margin:0 });
s.addText("The Immune System: Implications for Anesthetic Management", {
x:0.25, y:0.38, w:13, h:0.7, fontSize:22, bold:true, color:C.white, fontFace:"Calibri", margin:0,
});
// Why added box
s.addShape(pres.ShapeType.roundRect, { x:0.25, y:1.3, w:6.2, h:2.8, fill:{color:"EDE7F6"}, rectRadius:0.12, line:{color:C.purple, width:1} });
s.addText("WHY THIS CHAPTER WAS ADDED", { x:0.4, y:1.38, w:5.9, h:0.4, fontSize:12, bold:true, color:C.purple, margin:0 });
s.addText([
{ text: "COVID-19 pandemic", options:{bold:true, breakLine:true} },
{ text: " revealed critical gaps in understanding how anesthetics modulate immune function — viral pneumonia patients required unique anesthetic & ICU approaches.\n\n", options:{breakLine:false} },
{ text: "Growing evidence", options:{bold:true, breakLine:true} },
{ text: " that volatile agents, propofol, and opioids exert profound immunomodulatory effects affecting infection, cancer recurrence, and organ rejection.", options:{} },
], { x:0.4, y:1.82, w:5.9, h:2.15, fontSize:11.5, color:C.darkgray, fontFace:"Calibri" });
// What it covers
s.addShape(pres.ShapeType.roundRect, { x:6.7, y:1.3, w:6.35, h:2.8, fill:{color:"EDE7F6"}, rectRadius:0.12, line:{color:C.purple, width:1} });
s.addText("WHAT IT COVERS", { x:6.85, y:1.38, w:6.0, h:0.4, fontSize:12, bold:true, color:C.purple, margin:0 });
const immuneItems = [
"Innate vs adaptive immunity — anesthesia effects",
"Volatile anesthetics (sevoflurane, isoflurane): anti-inflammatory effects via cytokine modulation",
"Propofol: immunosuppressive properties — clinical relevance in oncology patients",
"Opioids (morphine, fentanyl): immune suppression — links to surgical site infections",
"COVID-19 protocols: airway management, PPE, aerosol-generating procedures",
"Perioperative infection control in high-risk patients",
"Implications for organ transplantation & cancer surgery",
];
s.addText(immuneItems.map((t,i)=>({text:t, options:{bullet:true, breakLine:i<immuneItems.length-1, fontSize:11, color:C.darkgray, fontFace:"Calibri"}})), {
x:6.85, y:1.82, w:6.0, h:2.15,
});
// Clinical impact
s.addShape(pres.ShapeType.roundRect, { x:0.25, y:4.25, w:12.8, h:2.8, fill:{color:C.purple}, rectRadius:0.12 });
s.addText("CLINICAL IMPACT FOR THE ANESTHESIOLOGIST", { x:0.45, y:4.35, w:12.4, h:0.4, fontSize:13, bold:true, color:C.gold, margin:0 });
const impactItems = [
"Cancer patients: choice of anesthetic technique (regional vs. GA) may affect tumor recurrence — this chapter synthesizes the evidence",
"Transplant patients: understanding immunosuppression interactions with anesthetic drugs",
"Sepsis & critical illness: anesthetic immunomodulation in ICU patients",
"Post-COVID surgical patients: modified airway & ventilation protocols",
];
s.addText(impactItems.map((t,i)=>({text:t, options:{bullet:true, breakLine:i<impactItems.length-1, fontSize:11.5, color:C.white, fontFace:"Calibri"}})), {
x:0.45, y:4.78, w:12.4, h:2.15,
});
}
// Slide: New Chapter 2 — Emergency Preparedness
{
const s = pres.addSlide();
s.addShape(pres.ShapeType.rect, { x:0, y:0, w:"100%", h:"100%", fill:{color:C.ltgray} });
s.addShape(pres.ShapeType.rect, { x:0, y:0, w:"100%", h:1.15, fill:{color:C.orange} });
s.addShape(pres.ShapeType.rect, { x:0, y:0, w:0.06, h:"100%", fill:{color:C.orange} });
s.addText("NEW CHAPTER | Chapter 85", { x:0.25, y:0.05, w:13, h:0.35, fontSize:12, color:"FFE0B2", bold:true, charSpacing:5, margin:0 });
s.addText("Emergency Preparedness in Healthcare", {
x:0.25, y:0.38, w:13, h:0.7, fontSize:26, bold:true, color:C.white, fontFace:"Calibri", margin:0,
});
s.addShape(pres.ShapeType.roundRect, { x:0.25, y:1.3, w:6.2, h:2.75, fill:{color:"FFF3E0"}, rectRadius:0.12, line:{color:C.orange, width:1} });
s.addText("WHY THIS CHAPTER WAS ADDED", { x:0.4, y:1.38, w:5.9, h:0.4, fontSize:12, bold:true, color:C.orange, margin:0 });
s.addText([
{ text: "COVID-19 pandemic (2020-2022)", options:{bold:true, breakLine:true} },
{ text: " exposed catastrophic gaps in hospital preparedness — supply chains, surge capacity, PPE protocols, and staff safety.\n\n", options:{} },
{ text: "Anesthesiologists", options:{bold:true} },
{ text: " are de facto first responders in mass-casualty, biological, and chemical events — requiring formalized training not previously in the text.", options:{} },
], { x:0.4, y:1.82, w:5.9, h:2.1, fontSize:11.5, color:C.darkgray, fontFace:"Calibri" });
s.addShape(pres.ShapeType.roundRect, { x:6.7, y:1.3, w:6.35, h:2.75, fill:{color:"FFF3E0"}, rectRadius:0.12, line:{color:C.orange, width:1} });
s.addText("WHAT IT COVERS", { x:6.85, y:1.38, w:6.0, h:0.4, fontSize:12, bold:true, color:C.orange, margin:0 });
const prepItems = [
"Hospital incident command systems (HICS)",
"Mass-casualty incident (MCI) triage & anesthetic management",
"Pandemic protocols: COVID-19 lessons for future outbreaks",
"Chemical & biological warfare agent exposure",
"PPE protocols & donning/doffing for aerosol-generating procedures",
"Surge capacity planning for OR & ICU",
"Psychological resilience & staff support in crises",
"Communication frameworks during disasters",
];
s.addText(prepItems.map((t,i)=>({text:t, options:{bullet:true, breakLine:i<prepItems.length-1, fontSize:11, color:C.darkgray, fontFace:"Calibri"}})), {
x:6.85, y:1.82, w:6.0, h:2.1,
});
s.addShape(pres.ShapeType.roundRect, { x:0.25, y:4.2, w:12.8, h:2.85, fill:{color:C.orange}, rectRadius:0.12 });
s.addText("WHY THIS MATTERS TO YOU AS AN ANESTHESIOLOGIST", { x:0.45, y:4.3, w:12.4, h:0.4, fontSize:13, bold:true, color:C.white, margin:0 });
s.addText([
{ text: "Pre-COVID: ", options:{bold:true} },
{ text: "Emergency preparedness was scattered across surgical texts, disaster medicine manuals, and institution-specific protocols. No single anesthesia resource addressed it comprehensively.\n\n", options:{} },
{ text: "Post-COVID: ", options:{bold:true} },
{ text: "This chapter consolidates everything — from respiratory protection to psychological safety of anesthesia providers — making it exam-relevant and operationally essential.", options:{} },
], { x:0.45, y:4.75, w:12.4, h:2.15, fontSize:11.5, color:C.white, fontFace:"Calibri" });
}
// ══════════════════════════════════════════════════════════════════════════════
// SECTION 2 — STRUCTURAL CHANGES
// ══════════════════════════════════════════════════════════════════════════════
sectionDivider(2, "Structural & Editorial Changes", "How the book was reorganized — and why it matters for how you learn");
// Chapter structure comparison
{
const s = pres.addSlide();
s.addShape(pres.ShapeType.rect, { x:0, y:0, w:"100%", h:"100%", fill:{color:C.ltgray} });
s.addShape(pres.ShapeType.rect, { x:0, y:0, w:"100%", h:1.1, fill:{color:C.teal} });
s.addShape(pres.ShapeType.rect, { x:0, y:0, w:0.06, h:"100%", fill:{color:C.teal} });
s.addText("Chapter Structure & Organization", { x:0.25, y:0.15, w:13, h:0.75, fontSize:26, bold:true, color:C.white, margin:0 });
// Table header
const headers = ["Feature", "9th Edition (2019)", "10th Edition (2024)", "Reason for Change"];
const rows = [
["Total chapters", "~90 chapters", "~87 chapters", "Redundant topics merged; cleaner flow"],
["Echocardiography", "Ch 37: Perioperative Echocardiography only", "Ch 33: Echocardiography AND POCUS combined", "POCUS exploded in clinical practice post-2019"],
["Neurologic monitoring", "Ch 39 & 40 (two chapters — Neurologic Monitoring + Depth of Anesthesia)", "Ch 35 & 36 (renamed, updated, restructured)", "Reflects new BIS/EEG data and awareness monitoring guidelines"],
["Immune chapter", "None", "Ch 26 — dedicated immune chapter (NEW)", "COVID-19 and cancer anesthesia evidence base"],
["Emergency preparedness", "Ch 68 — Disasters (limited)", "Ch 85 — Full Emergency Preparedness chapter (NEW)", "Pandemic lessons; anesthesiologist role in disaster response"],
["Pediatric section", "4 chapters (76-79)", "Expanded pediatric coverage (5 chapters 70-75)", "Growing complexity of pediatric subspecialties"],
["Post-op cognitive issues", "Ch 83 — 'Cognitive Dysfunction & Long-Term Complications'", "Ch 78 — 'Perioperative Neurocognitive Disorders' (renamed)", "2018 renaming consensus (NCD/POCD replaced by PACD/POCD/PODS terminology)"],
["Section numbering", "8 sections", "8 sections but reordered", "Better logical flow from basic to clinical science"],
];
const colW = [2.0, 3.1, 3.1, 4.6];
const colX = [0.2, 2.22, 5.34, 8.46];
const rowH = 0.55;
const startY = 1.2;
// header row
headers.forEach((h,ci) => {
s.addShape(pres.ShapeType.rect, { x:colX[ci], y:startY, w:colW[ci], h:0.5, fill:{color:C.teal} });
s.addText(h, { x:colX[ci]+0.05, y:startY, w:colW[ci]-0.1, h:0.5, fontSize:11, bold:true, color:C.white, valign:"middle", margin:0 });
});
// data rows
rows.forEach((row, ri) => {
const y = startY + 0.5 + ri * rowH;
row.forEach((cell, ci) => {
const bg = ri % 2 === 0 ? C.white : "E8F4FD";
s.addShape(pres.ShapeType.rect, { x:colX[ci], y, w:colW[ci], h:rowH, fill:{color:bg}, line:{color:"D0D7DE", width:0.3} });
s.addText(cell, { x:colX[ci]+0.06, y:y+0.03, w:colW[ci]-0.12, h:rowH-0.06, fontSize:9.5, color:C.darkgray, valign:"middle", shrinkText:true });
});
});
}
// ══════════════════════════════════════════════════════════════════════════════
// SECTION 3 — POCUS
// ══════════════════════════════════════════════════════════════════════════════
sectionDivider(3, "POCUS — Point-of-Care Ultrasound", "The single biggest technology update in the 10th edition");
{
const s = pres.addSlide();
s.addShape(pres.ShapeType.rect, { x:0, y:0, w:"100%", h:"100%", fill:{color:C.ltgray} });
s.addShape(pres.ShapeType.rect, { x:0, y:0, w:"100%", h:1.1, fill:{color:C.teal} });
s.addShape(pres.ShapeType.rect, { x:0, y:0, w:0.06, h:"100%", fill:{color:C.teal} });
s.addText("POCUS: From Echo to Bedside Ultrasound — Chapter 33", { x:0.25, y:0.15, w:13, h:0.75, fontSize:24, bold:true, color:C.white, margin:0 });
// left = 9th
s.addShape(pres.ShapeType.roundRect, { x:0.25, y:1.2, w:6.1, h:5.9, fill:{color:C.white}, rectRadius:0.12, line:{color:C.red, width:1.5} });
s.addShape(pres.ShapeType.roundRect, { x:0.25, y:1.2, w:6.1, h:0.5, fill:{color:C.red}, rectRadius:0.1 });
s.addText("9th Edition — Ch 37: Perioperative Echocardiography", { x:0.35, y:1.2, w:5.9, h:0.5, fontSize:11.5, bold:true, color:C.white, align:"center", valign:"middle" });
const items9 = [
"Focused on TEE (transesophageal echocardiography)",
"TTE (transthoracic) briefly covered",
"No dedicated POCUS section",
"Ultrasound for regional anesthesia in a separate chapter",
"No lung ultrasound protocols",
"No vascular access ultrasound in this chapter",
"Limited guidance on POCUS in critical care",
"Basic perioperative echo views described",
];
s.addText(items9.map((t,i)=>({text:t, options:{bullet:true, breakLine:i<items9.length-1, fontSize:11, color:C.darkgray, fontFace:"Calibri"}})), {
x:0.4, y:1.82, w:5.8, h:5.1,
});
// VS
s.addShape(pres.ShapeType.roundRect, { x:6.28, y:3.5, w:0.74, h:0.74, fill:{color:C.gold}, rectRadius:0.37 });
s.addText("VS", { x:6.28, y:3.5, w:0.74, h:0.74, fontSize:16, bold:true, color:C.navy, align:"center", valign:"middle" });
// right = 10th
s.addShape(pres.ShapeType.roundRect, { x:7.0, y:1.2, w:6.1, h:5.9, fill:{color:C.white}, rectRadius:0.12, line:{color:C.green, width:1.5} });
s.addShape(pres.ShapeType.roundRect, { x:7.0, y:1.2, w:6.1, h:0.5, fill:{color:C.green}, rectRadius:0.1 });
s.addText("10th Edition — Ch 33: Echo AND POCUS", { x:7.1, y:1.2, w:5.9, h:0.5, fontSize:11.5, bold:true, color:C.white, align:"center", valign:"middle" });
const items10 = [
"Full TEE & TTE (transthoracic) coverage with updated views",
"DEDICATED POCUS section — adults AND pediatrics",
"Lung ultrasound: B-lines, pneumothorax, effusion protocols",
"Vascular access POCUS — arterial, venous",
"POCUS in cardiac arrest (FEEL protocol)",
"Focused abdominal & renal POCUS",
"Pediatric POCUS applications expanded",
"POCUS image acquisition technique & pitfalls",
"Integration with regional anesthesia workflows",
];
s.addText(items10.map((t,i)=>({text:t, options:{bullet:true, breakLine:i<items10.length-1, fontSize:11, color:C.darkgray, fontFace:"Calibri", bold:i===1||i===4}})), {
x:7.15, y:1.82, w:5.8, h:5.1,
});
}
// ══════════════════════════════════════════════════════════════════════════════
// SECTION 4 — KEY CLINICAL CHAPTER UPDATES
// ══════════════════════════════════════════════════════════════════════════════
sectionDivider(4, "Major Clinical Chapter Updates", "Updated guidelines, new evidence, and expanded clinical content");
// Neurocognitive disorders
{
const s = contentSlide("Perioperative Neurocognitive Disorders — Ch 78 (was Ch 83)", C.blue);
compareBoxes(s,
"Cognitive Dysfunction\n& Long-Term Complications",
[
"Terminology: POCD (Post-Op Cognitive Dysfunction) — outdated but used",
"Combined postoperative complications into one chapter",
"Limited mechanistic detail on neuroinflammation",
"No standardized diagnostic criteria presented",
"Minimal discussion of biomarkers",
"Delirium covered briefly",
],
"Perioperative\nNeurocognitive Disorders",
[
"UPDATED terminology per 2018 consensus: PACD (Acute) / POCD (Delayed) / PODS (Delayed onset) / Periop NCD",
"Dedicated separate chapter — expanded substantially",
"Neuroinflammation: IL-6, TNF-α, microglial activation mechanisms",
"EEG-based monitoring for suppression and burst-suppression",
"Biomarkers: GFAP, NfL, tau, S100β perioperative role",
"Prevention: BIS-guided anaesthesia reduces POCD incidence",
"Dexmedetomidine evidence for PACD prevention in ICU",
],
C.red, C.green
);
}
// Airway management
{
const s = contentSlide("Airway Management in the Adult — Ch 40 (was Ch 44)", C.navy);
compareBoxes(s,
"Airway Management\n(9th Edition)",
[
"DAS/ASA difficult airway algorithm (2013 versions)",
"Videolaryngoscopy mentioned but not front-and-centre",
"Supraglottic airways: LMA, i-gel covered",
"CICO concept included but not emphasized",
"Cricothyroidotomy: standard surgical technique",
"Awake intubation: fiberoptic as gold standard",
"Limited coverage of high-flow nasal oxygen (HFNO)",
],
"Airway Management\n(10th Edition)",
[
"Updated DAS (2015) & ASA (2022) difficult airway guidelines fully incorporated",
"Videolaryngoscopy: prominent role — first-line in many scenarios",
"eFONA (emergency front-of-neck access) expanded with scalpel-bougie technique",
"HFNO (high-flow nasal oxygen) — apneic oxygenation protocols",
"THRIVE (Transnasal Humidified Rapid-Insufflation Ventilatory Exchange) covered",
"Awake intubation: combined VL + FOB techniques",
"COVID-19 airway modifications (donning, closed-circuit techniques)",
],
C.red, C.green
);
}
// Pharmacology — opioids & NMB
{
const s = contentSlide("Pharmacology Updates — Opioids, NMBDs & Intravenous Anesthetics", C.teal);
compareBoxes(s,
"9th Edition\nPharmacology Coverage",
[
"Opioid crisis mentioned but limited perioperative guidance",
"Sugammadex: established but dosing controversies unresolved",
"Remimazolam: mentioned only",
"Dexmedetomidine: limited perioperative role described",
"IV drug delivery: TIVA algorithms present",
"No specific opioid-sparing multimodal analgesia framework",
],
"10th Edition\nPharmacology Coverage",
[
"Opioid-sparing / opioid-free anesthesia (OFA) — expanded framework",
"Sugammadex: updated dosing, reversal at profound block, safety evidence",
"Remimazolam: full coverage — pharmacokinetics, clinical use, reversal (flumazenil)",
"Dexmedetomidine: expanded role — ICU sedation, opioid sparing, PACD prevention",
"TIVA: updated TCI models (Eleveld propofol, Minto remifentanil)",
"Multimodal analgesia: ketamine, dexamethasone, lidocaine infusion, NSAIDs",
"Opioid-induced hyperalgesia — mechanisms and clinical relevance",
],
C.red, C.green
);
}
// ══════════════════════════════════════════════════════════════════════════════
// SECTION 5 — NEW CONTENT THEMES
// ══════════════════════════════════════════════════════════════════════════════
sectionDivider(5, "New Content Themes & Topics", "Cross-cutting themes that permeate the entire 10th edition");
// Sustainability + Global health
{
const s = pres.addSlide();
s.addShape(pres.ShapeType.rect, { x:0, y:0, w:"100%", h:"100%", fill:{color:C.ltgray} });
s.addShape(pres.ShapeType.rect, { x:0, y:0, w:"100%", h:1.1, fill:{color:C.green} });
s.addShape(pres.ShapeType.rect, { x:0, y:0, w:0.06, h:"100%", fill:{color:C.green} });
s.addText("Two Major New Themes: Sustainability & Global Health Equity", { x:0.25, y:0.15, w:13, h:0.75, fontSize:22, bold:true, color:C.white, margin:0 });
// Box 1 — Sustainability
s.addShape(pres.ShapeType.roundRect, { x:0.25, y:1.2, w:6.0, h:5.95, fill:{color:C.white}, rectRadius:0.12, line:{color:C.green, width:1.5} });
s.addShape(pres.ShapeType.rect, { x:0.25, y:1.2, w:6.0, h:0.5, fill:{color:C.green} });
s.addText("🌱 SUSTAINABILITY IN ANESTHESIA", { x:0.35, y:1.2, w:5.8, h:0.5, fontSize:13, bold:true, color:C.white, align:"center", valign:"middle" });
const sustItems = [
"NOT in 9th edition — entirely new content",
"Volatile anesthetic agents contribute to greenhouse gas emissions:",
" • Desflurane: GWP 2540× CO₂ over 100 years",
" • Sevoflurane: GWP 130× CO₂",
" • Isoflurane: GWP 510× CO₂",
"Desflurane: many centres globally discontinuing due to climate impact",
"Low-flow anesthesia techniques to reduce agent consumption",
"TIVA (propofol) as a more environmentally friendly alternative",
"Nitrous oxide: stratospheric ozone depletion — clinical re-evaluation",
"Green anesthesia movement: WFSA + ASA sustainability initiatives",
"Medical waste reduction protocols in OR",
];
s.addText(sustItems.map((t,i)=>({text:t, options:{bullet:i>0, breakLine:i<sustItems.length-1, fontSize:10.5, color:C.darkgray, fontFace:"Calibri", bold:i===0||i===6}})), {
x:0.4, y:1.82, w:5.7, h:5.2,
});
// Box 2 — Global health
s.addShape(pres.ShapeType.roundRect, { x:6.95, y:1.2, w:6.1, h:5.95, fill:{color:C.white}, rectRadius:0.12, line:{color:C.teal, width:1.5} });
s.addShape(pres.ShapeType.rect, { x:6.95, y:1.2, w:6.1, h:0.5, fill:{color:C.teal} });
s.addText("🌍 GLOBAL HEALTH EQUITY", { x:7.05, y:1.2, w:5.9, h:0.5, fontSize:13, bold:true, color:C.white, align:"center", valign:"middle" });
const globalItems = [
"Significantly expanded from 9th edition",
"The global surgical burden: 5 billion people lack access to safe surgery",
"Lancet Commission on Global Surgery — anesthesia as a public health priority",
"Low/middle income countries (LMIC):",
" • Ketamine as the workhorse anesthetic in resource-limited settings",
" • Spinal anesthesia without complex monitoring",
" • Oxygen supply challenges and alternatives",
"Training & capacity building — task-shifting, nurse anesthetists",
"WHO Global Pulse Oximetry Project",
"Global disparities in perioperative mortality (maternal mortality esp.)",
"New editor Johnson-Akeju brings African/global perspective",
];
s.addText(globalItems.map((t,i)=>({text:t, options:{bullet:i>0, breakLine:i<globalItems.length-1, fontSize:10.5, color:C.darkgray, fontFace:"Calibri", bold:i===0||i===10}})), {
x:7.1, y:1.82, w:5.8, h:5.2,
});
}
// COVID-19 & Infection Control
{
const s = pres.addSlide();
s.addShape(pres.ShapeType.rect, { x:0, y:0, w:"100%", h:"100%", fill:{color:C.ltgray} });
s.addShape(pres.ShapeType.rect, { x:0, y:0, w:"100%", h:1.1, fill:{color:C.navy} });
s.addShape(pres.ShapeType.rect, { x:0, y:0, w:0.06, h:"100%", fill:{color:C.gold} });
s.addText("COVID-19 Impact on Anesthetic Practice — New Content Throughout", { x:0.25, y:0.15, w:13, h:0.75, fontSize:22, bold:true, color:C.white, margin:0 });
// 3-column grid
const cols = [
{ x:0.25, title:"Airway\nManagement", color:C.blue, items:[
"Closed-circuit intubation techniques",
"N95/FFP3 respirator protocols",
"Video laryngoscopy as first-line in COVID",
"Aerosol-generating procedure (AGP) classification",
"Rapid-sequence intubation modifications",
"Extubation in COVID — PPE & risk stratification",
]},
{ x:4.5, title:"ICU &\nCritical Care", color:C.teal, items:[
"ARDS management: prone positioning protocols",
"Awake prone positioning (APP) — novel technique",
"High-flow nasal oxygen (HFNO) evidence",
"Non-invasive ventilation in COVID ARDS",
"Dexamethasone: RECOVERY trial evidence",
"Anticoagulation in COVID coagulopathy",
]},
{ x:8.75, title:"OR Safety &\nInfection Control", color:C.purple, items:[
"OR negative pressure design considerations",
"Terminal OR cleaning protocols",
"PPE donning/doffing algorithms",
"Elective surgery postponement criteria",
"Vaccination status and perioperative risk",
"Post-COVID lung function assessment",
]},
];
const bw = 4.0;
cols.forEach(col => {
s.addShape(pres.ShapeType.roundRect, { x:col.x, y:1.2, w:bw, h:5.9, fill:{color:C.white}, rectRadius:0.12, line:{color:col.color, width:1.5} });
s.addShape(pres.ShapeType.rect, { x:col.x, y:1.2, w:bw, h:0.65, fill:{color:col.color} });
s.addText(col.title, { x:col.x+0.1, y:1.2, w:bw-0.2, h:0.65, fontSize:13, bold:true, color:C.white, align:"center", valign:"middle" });
s.addText(col.items.map((t,i)=>({text:t, options:{bullet:true, breakLine:i<col.items.length-1, fontSize:11, color:C.darkgray, fontFace:"Calibri"}})), {
x:col.x+0.15, y:1.95, w:bw-0.3, h:4.95,
});
});
s.addText("9th Edition (published 2019): Pre-COVID — none of this content existed", {
x:0.25, y:7.1, w:13, h:0.3, fontSize:10, color:C.midgray, italic:true, align:"center",
});
}
// ══════════════════════════════════════════════════════════════════════════════
// SECTION 6 — SUBSPECIALTY UPDATES
// ══════════════════════════════════════════════════════════════════════════════
sectionDivider(6, "Subspecialty Updates", "Pediatrics, regional, critical care, and special populations");
// Pediatric
{
const s = contentSlide("Pediatric Anesthesia — Expanded & Restructured (Ch 70-75)", C.blue);
compareBoxes(s,
"9th Edition Pediatrics\n(4 chapters: 76-79)",
[
"Pediatric Regional: Ch 76",
"General Pediatric Anesthesia: Ch 77 (broad, single chapter)",
"Cardiac Surgery Pediatrics: Ch 78",
"Pediatric & Neonatal ICU: Ch 79",
"Limited congenital heart disease depth",
"POCUS in children: minimal coverage",
"Neonatal physiology: covered in general chapter",
],
"10th Edition Pediatrics\n(5+ chapters: 70-75)",
[
"Expanded to 5-6 chapters — significantly more detail",
"Separate dedicated neonatal anesthesia content",
"Congenital cardiac anesthesia: greatly expanded",
"Pediatric POCUS: dedicated section (unique to 10th ed)",
"Pediatric regional anesthesia: ultrasound-guided techniques front-and-centre",
"Neonatal physiology & pharmacology: expanded",
"Paediatric critical care: updated mechanical ventilation protocols",
],
C.red, C.green
);
}
// Critical care
{
const s = contentSlide("Critical Care Medicine — Section VII Updates", C.teal);
compareBoxes(s,
"9th Edition Critical Care\n(Ch 84-87)",
[
"ECMO: Ch 86 — basics covered",
"CPR/ACLS: AHA 2015 guidelines",
"Neurocritical care: standard coverage",
"No specific ARDS protocol integration",
"Vasopressor protocols: older evidence base",
"Liberation from mechanical ventilation: standard criteria",
],
"10th Edition Critical Care\n(Ch 79-82)",
[
"ECMO: updated with expanded VA-ECMO & VV-ECMO for COVID ARDS",
"CPR/ACLS: AHA 2020 guidelines — new compression targets, TTM update (32-36°C)",
"Neurocritical care: updated TBI protocols, multimodal monitoring",
"ARDS: Berlin definition, COVID-ARDS nuances, driving pressure concept",
"Vasopressors: norepinephrine-first evidence (CATS/SOAP-II), vasopressin role",
"Dexmedetomidine: evidence for ICU sedation and delirium prevention",
"Liberation: updated ventilator weaning SBT protocols",
],
C.red, C.green
);
}
// Regional
{
const s = contentSlide("Regional Anesthesia — Ch 42 (was Ch 46): US-Guided Techniques", C.purple);
compareBoxes(s,
"9th Edition Regional\n(Ch 46: Peripheral Nerve Blocks)",
[
"Ultrasound guidance: covered but not the central focus",
"Traditional landmark & nerve stimulator techniques still prominent",
"LAST: covered in local anesthetic chapter",
"Fascial plane blocks: mentioned (e.g., TAP block)",
"FICB, serratus, PECS: limited coverage",
"No formal LAST checklist referenced",
"Opioid-sparing role of regional: mentioned",
],
"10th Edition Regional\n(Ch 42: US-Guided Regional + POCUS)",
[
"Ultrasound-guided approach: primary methodology throughout",
"Landmark techniques retained as backup only",
"LAST: updated ASRA 2020 checklist — lipid emulsion protocols",
"Erector spinae plane (ESP) block — full new coverage",
"PECS I & II, serratus, quadratus lumborum (QL) blocks — expanded",
"Fascial plane blocks for thoracic surgery (ESPB, paravertebral)",
"Continuous nerve block catheters & ambulatory regional",
"Opioid-free anesthesia protocols with regional as core",
],
C.red, C.green
);
}
// ══════════════════════════════════════════════════════════════════════════════
// SECTION 7 — EDITORIAL CHANGES
// ══════════════════════════════════════════════════════════════════════════════
sectionDivider(7, "Editorial & Presentation Changes", "New editor, book design, and readability improvements");
{
const s = pres.addSlide();
s.addShape(pres.ShapeType.rect, { x:0, y:0, w:"100%", h:"100%", fill:{color:C.ltgray} });
s.addShape(pres.ShapeType.rect, { x:0, y:0, w:"100%", h:1.1, fill:{color:C.darkgray} });
s.addShape(pres.ShapeType.rect, { x:0, y:0, w:0.06, h:"100%", fill:{color:C.gold} });
s.addText("Editorial Board, Book Design & Usability Changes", { x:0.25, y:0.15, w:13, h:0.75, fontSize:24, bold:true, color:C.white, margin:0 });
// Editors comparison
s.addShape(pres.ShapeType.roundRect, { x:0.25, y:1.2, w:6.1, h:2.8, fill:{color:C.white}, rectRadius:0.12, line:{color:C.red, width:1.5} });
s.addShape(pres.ShapeType.rect, { x:0.25, y:1.2, w:6.1, h:0.45, fill:{color:C.red} });
s.addText("9th Edition Editors", { x:0.35, y:1.2, w:5.9, h:0.45, fontSize:13, bold:true, color:C.white, align:"center", valign:"middle" });
s.addText([
{ text: "Lead: ", options:{bold:true} },{ text: "Michael A. Gropper, MD, PhD\n", options:{} },
{ text: "Ronald D. Miller, MD, MS\n", options:{} },
{ text: "Lars I. Eriksson, MD\n", options:{} },
{ text: "Lee A. Fleisher, MD\n", options:{} },
{ text: "Jeanine P. Wiener-Kronish, MD\n", options:{} },
{ text: "Neal H. Cohen, MD, MPH, MS\n", options:{} },
{ text: "Kate Leslie, MD\n", options:{} },
], { x:0.4, y:1.75, w:5.8, h:2.1, fontSize:11.5, color:C.darkgray, fontFace:"Calibri" });
s.addShape(pres.ShapeType.roundRect, { x:6.95, y:1.2, w:6.1, h:2.8, fill:{color:C.white}, rectRadius:0.12, line:{color:C.green, width:1.5} });
s.addShape(pres.ShapeType.rect, { x:6.95, y:1.2, w:6.1, h:0.45, fill:{color:C.green} });
s.addText("10th Edition Editors", { x:7.05, y:1.2, w:5.9, h:0.45, fontSize:13, bold:true, color:C.white, align:"center", valign:"middle" });
s.addText([
{ text: "Lead: ", options:{bold:true} },{ text: "Michael A. Gropper, MD, PhD\n", options:{} },
{ text: "Lars I. Eriksson, MD\n", options:{} },
{ text: "Lee A. Fleisher, MD\n", options:{} },
{ text: "Neal H. Cohen, MD, MPH, MS\n", options:{} },
{ text: "Kate Leslie, MD\n", options:{} },
{ text: "Oluwaseun Johnson-Akeju, MD ", options:{bold:true} },{ text: "★ NEW\n", options:{color:C.gold, bold:true} },
{ text: "Ronald Miller: retired from active editorial role", options:{color:C.midgray, italic:true} },
], { x:7.1, y:1.75, w:5.8, h:2.1, fontSize:11.5, color:C.darkgray, fontFace:"Calibri" });
// Design changes
s.addShape(pres.ShapeType.roundRect, { x:0.25, y:4.15, w:12.8, h:3.4, fill:{color:C.white}, rectRadius:0.12, line:{color:C.darkgray, width:1} });
s.addText("Book Design & Pedagogical Changes", { x:0.4, y:4.25, w:12.5, h:0.4, fontSize:13, bold:true, color:C.darkgray, margin:0 });
const designItems = [
["Chapter structure", "More cohesive logical progression from basic science → clinical application throughout both volumes"],
["Key points boxes", "Expanded 'Key Points' summary boxes at chapter start — exam-targeted"],
["Online content", "Updated online videos, interactive figures, and clinical cases"],
["Reading ease", "Dense 9th ed text restructured with subheadings for easier navigation in 10th ed"],
["Evidence grading", "Updated RCT and guideline references — post-2019 literature incorporated throughout"],
["Special populations", "Expanded coverage: elderly, obese, pregnant, and LMIC patients given more space"],
];
designItems.forEach(([label, text], i) => {
const y = 4.7 + i * 0.43;
s.addText(label + ":", { x:0.4, y, w:2.2, h:0.38, fontSize:11, bold:true, color:C.blue, margin:0 });
s.addText(text, { x:2.65, y, w:10.2, h:0.38, fontSize:11, color:C.darkgray, fontFace:"Calibri", margin:0 });
});
}
// ══════════════════════════════════════════════════════════════════════════════
// SECTION 8 — COMPREHENSIVE CHAPTER MAP
// ══════════════════════════════════════════════════════════════════════════════
sectionDivider(8, "Side-by-Side Chapter Map", "Where to find topics — 9th vs 10th edition numbering");
{
const s = pres.addSlide();
s.addShape(pres.ShapeType.rect, { x:0, y:0, w:"100%", h:"100%", fill:{color:C.ltgray} });
s.addShape(pres.ShapeType.rect, { x:0, y:0, w:"100%", h:1.0, fill:{color:C.navy} });
s.addShape(pres.ShapeType.rect, { x:0, y:0, w:0.06, h:"100%", fill:{color:C.gold} });
s.addText("Chapter Mapping — Find the Same Topic in Each Edition", { x:0.25, y:0.12, w:13, h:0.72, fontSize:22, bold:true, color:C.white, margin:0 });
const headers2 = ["Topic", "9th Ed Chapter", "10th Ed Chapter", "Change Summary"];
const mapRows = [
["Immune System & Anesthesia", "— (Not present)", "Ch 26 ★ NEW", "Entirely new — COVID/immune evidence"],
["Emergency Preparedness", "Ch 68 (limited)", "Ch 85 ★ NEW", "Full chapter — pandemic lessons"],
["Perioperative Echocardiography + POCUS", "Ch 37", "Ch 33", "POCUS comprehensively added"],
["Airway Management", "Ch 44", "Ch 40", "Updated DAS 2015, ASA 2022, HFNO, eFONA"],
["Neurocognitive Disorders", "Ch 83", "Ch 78", "Renamed (NCD), new biomarkers, EEG monitoring"],
["Perioperative Fluid Therapy", "Ch 47", "Ch 43", "Updated GDFT targets, crystalloid vs colloid"],
["Regional Anesthesia (Peripheral)", "Ch 46", "Ch 42", "US-guided primary, ESP/PECS added, LAST update"],
["Intravenous Anesthetics", "Ch 23 (IV drugs + TIVA)", "Ch 21", "Remimazolam, updated TCI models"],
["Neuromuscular Blockers", "Ch 27", "Ch 24", "Sugammadex updated dosing, TOFR >0.9 target"],
["Opioids", "Ch 24", "Ch 22", "OIH, opioid-sparing, opioid-free anesthesia"],
["Pediatric Anesthesia", "Ch 77 (single broad chapter)", "Ch 70-72 (expanded)", "Subdivided, neonatal expanded"],
["Cardiac Surgery Anesthesia", "Ch 54", "Ch 50", "VA-ECMO, new hemodynamic targets updated"],
["Critical Care", "Ch 84", "Ch 79", "ARDS Berlin, COVID protocols, updated vasopressors"],
["CPR / ACLS", "Ch 87 — AHA 2015", "Ch 82 — AHA 2020", "Updated compression targets, TTM 32-36°C"],
["Occupational Safety", "Ch 92", "Ch 84", "COVID exposure, PPE protocols added"],
["Sustainability", "— (not present)", "Throughout + Section 1", "NEW — environmental impact of volatile agents"],
];
const hW = [3.2, 2.1, 2.1, 5.4];
const hX = [0.2, 3.42, 5.54, 7.66];
const rH = 0.37;
const sY = 1.1;
headers2.forEach((h,ci) => {
s.addShape(pres.ShapeType.rect, { x:hX[ci], y:sY, w:hW[ci], h:0.4, fill:{color:C.navy} });
s.addText(h, { x:hX[ci]+0.05, y:sY, w:hW[ci]-0.1, h:0.4, fontSize:11, bold:true, color:C.white, valign:"middle", margin:0 });
});
mapRows.forEach((row, ri) => {
const y = sY + 0.4 + ri * rH;
const bg = ri % 2 === 0 ? C.white : "EEF4FA";
row.forEach((cell, ci) => {
const textColor = ci===1 && cell.includes("Not") ? C.red : (ci===2 && cell.includes("★") ? C.green : C.darkgray);
s.addShape(pres.ShapeType.rect, { x:hX[ci], y, w:hW[ci], h:rH, fill:{color:bg}, line:{color:"D0D7DE", width:0.3} });
s.addText(cell, { x:hX[ci]+0.06, y:y+0.02, w:hW[ci]-0.12, h:rH-0.04, fontSize:9.5, color:textColor, bold:cell.includes("★"), valign:"middle", shrinkText:true });
});
});
}
// ══════════════════════════════════════════════════════════════════════════════
// SLIDE — WHAT DOES NOT CHANGE
// ══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.ShapeType.rect, { x:0, y:0, w:"100%", h:"100%", fill:{color:C.ltgray} });
s.addShape(pres.ShapeType.rect, { x:0, y:0, w:"100%", h:1.1, fill:{color:"4A6741"} });
s.addShape(pres.ShapeType.rect, { x:0, y:0, w:0.06, h:"100%", fill:{color:C.gold} });
s.addText("What Remains Unchanged — The Core of Miller's", { x:0.25, y:0.15, w:13, h:0.75, fontSize:24, bold:true, color:C.white, margin:0 });
const constant = [
["Physiology sections", "Basic cardiovascular, respiratory, renal, neurologic, and hepatic physiology — still comprehensive, considered the best basic science review in anesthesia"],
["Pharmacology foundations", "Volatile anesthetic mechanisms (Meyer-Overton, protein receptor theories), uptake & distribution, MAC concept — foundational content unchanged"],
["Monitoring principles", "Cardiovascular monitoring (arterial, CVP, PA catheter), respiratory monitoring, neuromuscular monitoring — principles stable"],
["Surgical subspecialties", "Thoracic, vascular, urologic, ENT, robotic, ambulatory anesthesia — updated content but stable organization"],
["Pain management", "Chronic pain chapter, acute postoperative pain — core content retained, evidence-updated"],
["Obstetric anesthesia", "Neuraxial techniques for labor & C-section, maternal physiology — retained and updated"],
["Book format", "Two-volume set continues; designed for both reference and study use"],
["Dr. Ronald Miller's legacy", "Founder and spirit of the book — his philosophy of evidence-based, comprehensive, physiology-first anesthesia remains unchanged"],
];
constant.forEach(([label, text], i) => {
const y = 1.2 + i * 0.74;
s.addShape(pres.ShapeType.roundRect, { x:0.25, y, w:12.8, h:0.68, fill:{color:C.white}, rectRadius:0.08, line:{color:"BDD5B8", width:0.5} });
s.addShape(pres.ShapeType.roundRect, { x:0.25, y, w:2.8, h:0.68, fill:{color:"E8F5E9"}, rectRadius:0.08 });
s.addText(label, { x:0.35, y:y+0.08, w:2.6, h:0.5, fontSize:11.5, bold:true, color:"2E7D32", fontFace:"Calibri", margin:0 });
s.addText(text, { x:3.18, y:y+0.07, w:9.75, h:0.54, fontSize:10.5, color:C.darkgray, fontFace:"Calibri", margin:0 });
});
}
// ══════════════════════════════════════════════════════════════════════════════
// FINAL SUMMARY SLIDE
// ══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.ShapeType.rect, { x:0, y:0, w:"100%", h:"100%", fill:{color:C.navy} });
s.addShape(pres.ShapeType.rect, { x:0, y:0, w:0.06, h:"100%", fill:{color:C.gold} });
s.addShape(pres.ShapeType.rect, { x:0.25, y:1.0, w:12.8, h:0.05, fill:{color:C.gold} });
s.addText("KEY TAKEAWAYS", { x:0.25, y:0.2, w:13, h:0.65, fontSize:14, bold:true, color:C.gold, charSpacing:8, margin:0 });
s.addText("What Every Resident Must Know: 9th vs 10th Edition", { x:0.25, y:0.7, w:13, h:0.3, fontSize:11, color:C.midgray, italic:true, margin:0 });
const takeaways = [
{ num:"1", title:"2 Brand-New Chapters", body:"Immune System (Ch 26) + Emergency Preparedness (Ch 85) — both reflect post-2019 world realities (COVID, cancer immunology, disaster medicine)", color:C.purple },
{ num:"2", title:"POCUS — The Biggest Technology Addition", body:"Ch 33 now combines perioperative echo AND point-of-care ultrasound — lung, vascular access, abdominal, pediatric POCUS all covered", color:C.teal },
{ num:"3", title:"New Editor Brings Global Perspective", body:"Dr. Johnson-Akeju adds global health equity emphasis — 5 billion people lack surgical access; anesthesia as public health is a new lens", color:C.blue },
{ num:"4", title:"COVID-19 Woven Throughout", body:"Airway modifications, immune chapter, ICU protocols, OR safety — the pandemic changed anesthesia and the 10th edition reflects this fully", color:C.orange },
{ num:"5", title:"Sustainability — A New Ethical Dimension", body:"Desflurane's GWP 2540× CO₂ — many centres have removed it. Green anesthesia content is entirely new to the 10th edition", color:C.green },
{ num:"6", title:"Updated Pharmacology", body:"Remimazolam, updated sugammadex dosing, opioid-free anesthesia framework, updated TCI models — stay current with 10th ed for drug questions", color:C.gold },
{ num:"7", title:"Perioperative Neurocognitive Disorders — Renamed & Expanded", body:"POCD replaced by PACD/POCD/PODS consensus terminology. New biomarkers (NfL, GFAP) and BIS-guided prevention protocols added", color:C.red },
];
takeaways.forEach((t, i) => {
const row = Math.floor(i / 4);
const col = i % 4;
const x = 0.25 + col * 3.26;
const y = 1.2 + row * 2.85;
const w = 3.15;
const h = 2.6;
s.addShape(pres.ShapeType.roundRect, { x, y, w, h, fill:{color:"0D1F35"}, rectRadius:0.15, line:{color:t.color, width:1.5} });
s.addShape(pres.ShapeType.roundRect, { x:x+0.1, y:y+0.1, w:0.5, h:0.5, fill:{color:t.color}, rectRadius:0.08 });
s.addText(t.num, { x:x+0.1, y:y+0.1, w:0.5, h:0.5, fontSize:18, bold:true, color:C.white, align:"center", valign:"middle" });
s.addText(t.title, { x:x+0.7, y:y+0.1, w:w-0.85, h:0.55, fontSize:11, bold:true, color:t.color, fontFace:"Calibri", margin:0 });
s.addText(t.body, { x:x+0.15, y:y+0.75, w:w-0.3, h:1.7, fontSize:9.5, color:C.white, fontFace:"Calibri" });
});
s.addText("Miller's Anesthesia 10th Edition (2024) — Reviewed for BJA Sept 2025: 'Gold standard reference for anaesthesia in North America'", {
x:0.25, y:7.15, w:13, h:0.28, fontSize:9, color:C.midgray, italic:true, align:"center",
});
}
// ══════════════════════════════════════════════════════════════════════════════
pres.writeFile({ fileName: "/home/daytona/workspace/millers-pptx/Millers_10th_vs_9th_Edition.pptx" })
.then(() => console.log("✅ Presentation saved successfully"))
.catch(err => console.error("❌ Error:", err));
cd /home/daytona/workspace/millers-pptx && node build.js 2>&1
ls -lh /home/daytona/workspace/millers-pptx/Millers_10th_vs_9th_Edition.pptx
differences between the 10th edition millers anaesthesia textbook to 9th ed millers - and explain to me the changes with reasons