Microscopy of endometrial. Carcinoma
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Finding Sources
I have comprehensive content. Now I'll compose the full answer.
Microscopy of Endometrial Carcinoma
Endometrial carcinoma has two main histologic types with distinct microscopic appearances: endometrioid carcinoma (80-85% of cases) and serous carcinoma (~15%). Their microscopy differs dramatically.
Endometrial Hyperplasia (Precursor Lesion)
Before invasion, the precursor stages are recognizable on H&E:
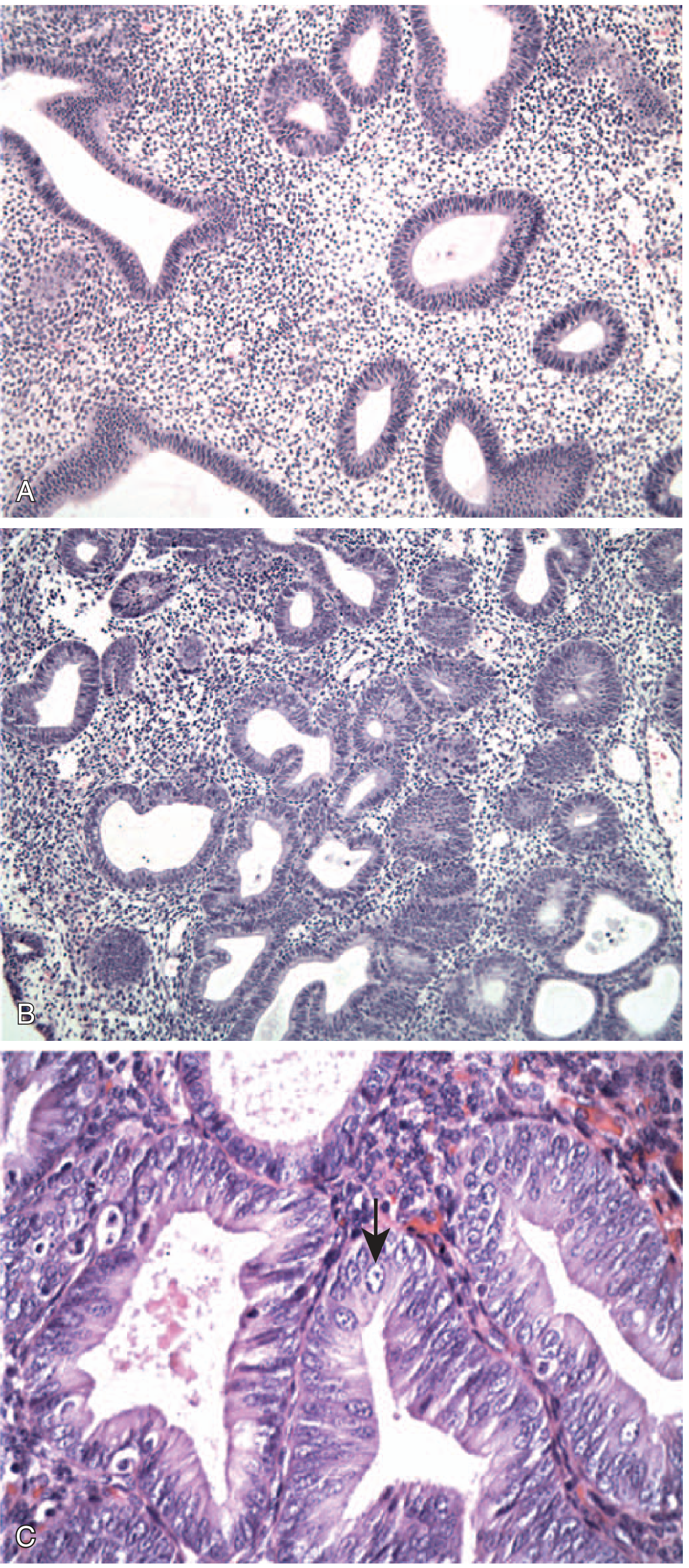
FIG. 17.11 - Endometrial hyperplasia. (A) Without atypia: mild glandular crowding and cystic dilation. (B) With atypia: glandular crowding + cellular atypia. (C) High magnification of atypical hyperplasia: rounded vesicular nuclei with prominent nucleoli (arrow). - Robbins & Kumar Basic Pathology
Endometrioid Carcinoma - Microscopic Features
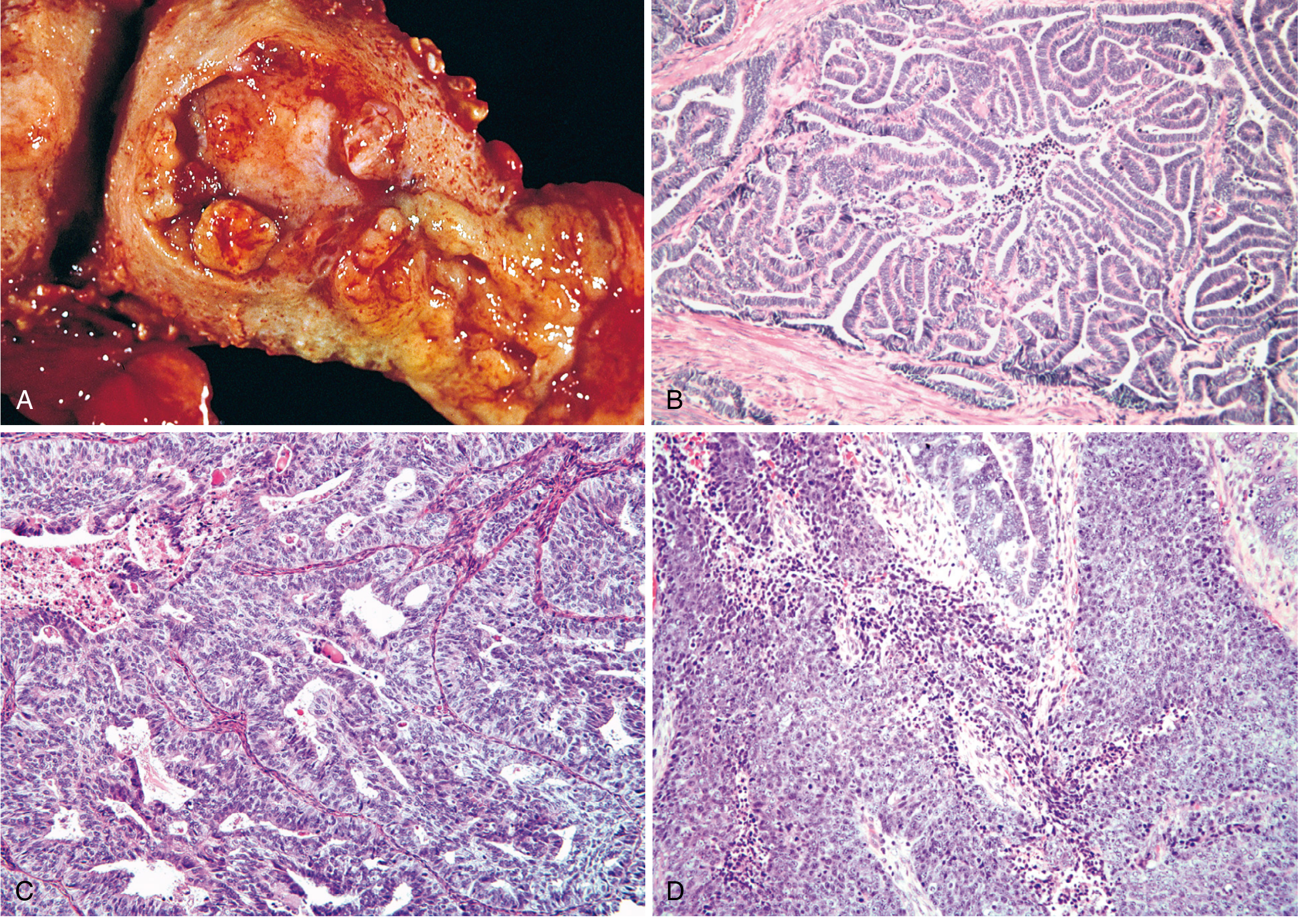
FIG. 22.24 - (A) Gross fungating mass. (B) Grade 1 well-differentiated endometrioid adenocarcinoma with preserved glandular architecture, back-to-back glands, no intervening stroma. (C) Grade 2 moderately differentiated with glandular architecture plus solid areas. (D) Grade 3 poorly differentiated with predominantly solid growth. - Robbins, Cotran & Kumar Pathologic Basis of Disease
Key microscopic features of endometrioid carcinoma:
Glandular architecture: The tumor closely mimics proliferative endometrium. Glands are crowded back-to-back with loss of intervening stroma ("gland-to-gland" apposition).
Grading (FIGO 1-3):
- Grade 1 (well differentiated): Almost entirely well-formed glands; minimal solid component (<5%). Cells show mild atypia, elongated nuclei.
- Grade 2 (moderately differentiated): Well-formed glands mixed with solid sheets that make up 6-50% of the tumor. Moderate cytologic atypia.
- Grade 3 (poorly differentiated): Predominantly solid growth pattern (>50% solid). Marked nuclear atypia, prominent nucleoli, frequent mitoses.
Distinguished from hyperplasia by:
- Desmoplastic stromal reaction around invading glands
- Confluent glandular growth without intervening stroma
- Papillary growth patterns
- Myometrial invasion
Squamous differentiation: Up to 20% of endometrioid carcinomas contain foci of squamous metaplasia. In low-grade tumors, the squamous elements appear benign (morules); in high-grade tumors they may be frankly malignant.
Tumor-infiltrating lymphocytes (TILs): Tumors with DNA mismatch repair defects (MLH1 loss by promoter methylation) or polymerase-epsilon (POLE) mutations often show abundant infiltrating T cells - an indicator of microsatellite instability.
Serous Endometrial Carcinoma - Microscopic Features
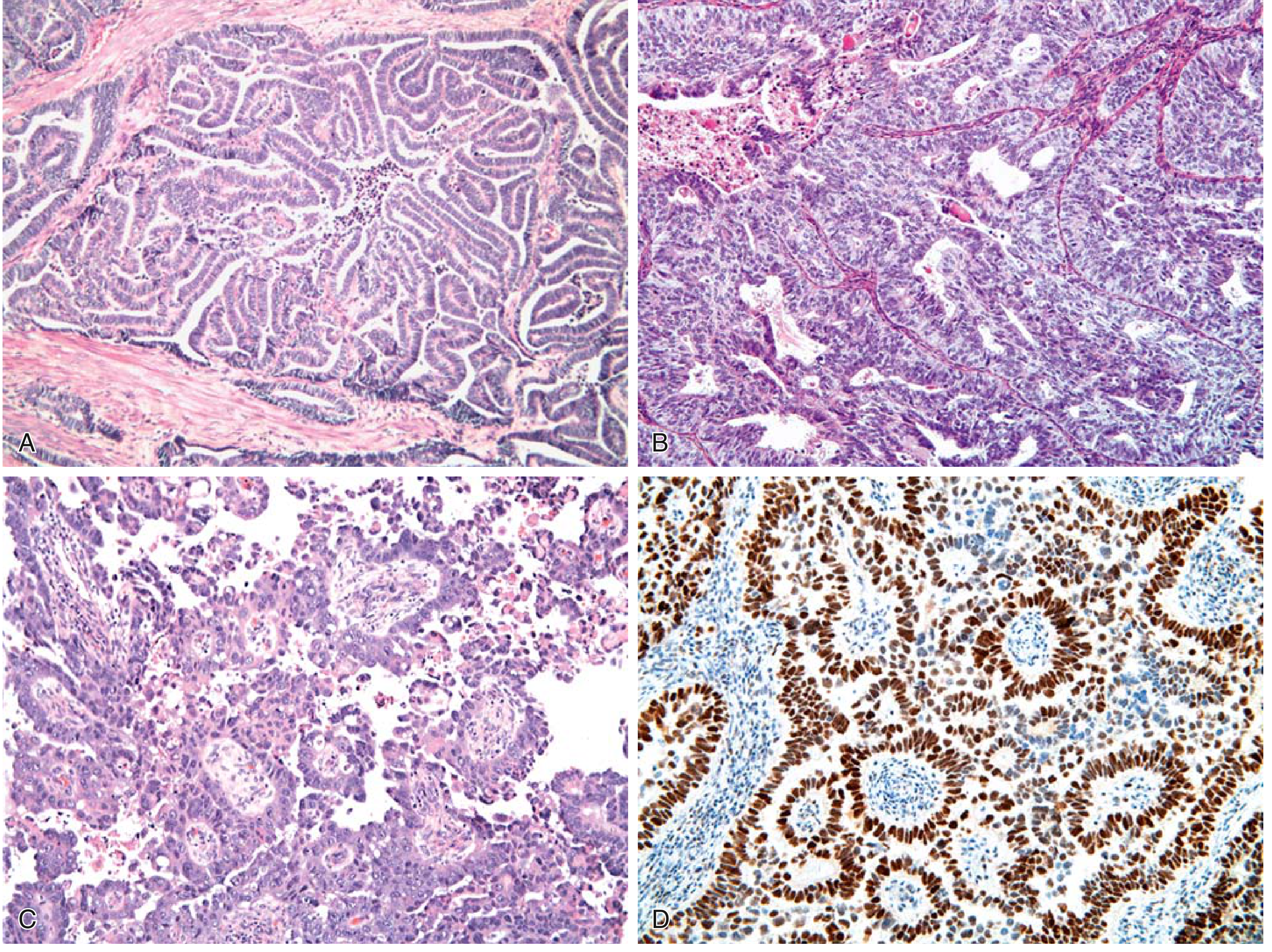
FIG. 17.12 - (A) Endometrioid type grade 1 with glandular infiltration into myometrium. (B) Grade 3 with solid growth. (C) Serous carcinoma with papilla formation and marked cytologic atypia. (D) Diffuse strong p53 IHC staining (brown nuclei) = TP53 mutation. - Robbins & Kumar Basic Pathology
Key microscopic features of serous carcinoma:
| Feature | Detail |
|---|---|
| Architecture | Papillary tufts and complex branching papillae; can also form glands |
| Cytologic atypia | Marked - high nuclear-to-cytoplasmic ratio, hyperchromasia, prominent nucleoli |
| Mitoses | Numerous, often atypical |
| Grade | Always high-grade by definition, regardless of architectural pattern |
| Precursor (SEIC) | Serous endometrial intraepithelial carcinoma - malignant cells confined to epithelial surface only, identical morphology |
| p53 IHC | Diffuse, strong nuclear positivity (mutant p53 accumulates) - key distinguishing feature |
Serous vs. endometrioid distinction: Both can form glands, but serous carcinoma shows far greater nuclear atypia. When architecture alone is ambiguous, p53 IHC helps - diffuse block positivity (or complete absence/"null pattern") indicates TP53 mutation.
Comparison Summary
| Feature | Endometrioid | Serous |
|---|---|---|
| Frequency | 80-85% | ~15% |
| Architecture | Glandular (back-to-back glands) | Papillary tufts, complex papillae |
| Cytologic atypia | Mild to moderate (G1-G2); severe (G3) | Always severe/high-grade |
| p53 IHC | Focal/weak (wild-type pattern) | Diffuse strong or null (mutant pattern) |
| Precursor | Atypical hyperplasia | Serous endometrial intraepithelial carcinoma (SEIC) |
| Molecular hallmark | PTEN, PIK3CA, KRAS mutations; MMR defects | TP53 mutations (>90%) |
| Associated setting | Estrogen excess (obesity, perimenopausal) | Endometrial atrophy (older postmenopausal) |
| Prognosis | Good (stage I: ~90% 5-year survival) | Poor (5-year survival 18-27%) |
Sources: Robbins & Kumar Basic Pathology (9780323790185); Robbins, Cotran & Kumar Pathologic Basis of Disease (9780443264528)
This is a shared conversation. Sign in to Orris to start your own chat.